
Abstract
Objective:
Surfactant administration has an essential role in the treatment of neonatal respiratory distress syndrome (RDS). This is coupled with the capability of a lung sonography scoring system (LUS scoring) in assessing neonatal lungs with RDS, makes evaluating the role of such a scoring system important in deciding to use surfactant therapy.
Materials and Methods:
This cross-sectional study was conducted on neonates with RDS, at a gestational age of more than 30 weeks. Using a high-frequency ultrasound transducer, neonates’ results were assessed by a radiologist, and then LUS scoring was determined in both groups, with and without the need for surfactant therapy.
Results:
The mean LUS scoring in the two groups was 9.08 ± 3.09 and 4.12 ± 2.56, respectively, which indicated a significant difference. The LUS scoring had a higher ability to predict the need for surfactant treatment, based on a receiver operating curve analysis. The best diagnostic cutoff point, for LUS scoring in predicting the need for surfactant treatment, was 6 in neonates 30–32 weeks and 7 in neonates 32–34 weeks. The use of LUS scoring had a sensitivity of 85.1%, 84% and a specificity of 87.2%, 88%, respectively.
Conclusion:
The LUS scoring may be used to help in the predicted need for surfactant therapy, in neonates with RDS.
During the last few years, the use of diagnostic lung sonography has progressed substantially. 1 In addition, significant progress has been made in using sonography in pediatrics, especially in assessing the developmental status of the fetus and infant. This diagnostic method has been very popular due to its cost-effectiveness and availability as well as its noninvasive approach. However, its sensitivity and specificity in the evaluation of neonatal disorders have been reported to be very diverse, due to the influence of various physiological and pathological factors. 2 This role has been particularly prominent in the assessment of neonatal respiratory disorders. Respiratory distress syndrome (RDS) is when the neonate has difficulty breathing, due to surfactant deficiency, at birth. Respiratory distress syndrome, also known as hyaline membrane disease, is an important clinical problem faced by preterm infants and is directly related to immature and surfactant-deficient lungs. Accordingly, various criteria have been proposed and interpreted to assess the rate of neonatal lung development, especially in the field of RDS, and sonographic assessment of fetal lung development has recently been described. 3
Overall, in neonates with RDS, the predominant ultrasound findings associated with the disorder include compact B-lines with an echogenic white appearance of the neonatal lung, the presence of thick and irregular pleural lines, and multiple subpleural pulmonary consolidations indicating alveolar collapse.4,5 These findings were able to detect RDS based on observations made with 100% sensitivity and specificity. However, it should be noted that the sonographic manifestations of RDS are not always bilaterally symmetrical and homogeneous and may be different in multiple parts of the lung.6–8
In general, pulmonary sonography has made it possible to quickly and accurately assess the natural alveolar bed of the lung. 9 In fact, sonography provides a description of the infant’s atypical respiratory status, including assessment of meconium aspiration syndrome, RDS, transient tachypnea of the newborn, and pneumothorax. Considering that in patients with RDS, the possibility of treatment with a continuous positive airway pressure approach and administration of selective surfactant can be provided. It is obvious that the changes in pulmonary function resulting from these treatments are in line with the diagnostic findings of lung sonography.10,11
Over time, with the introduction of quantitative scoring methods and systems for lung sonographic findings, it was possible to more accurately assess and classify RDS and its exacerbation or treatment process. 12 Today, such sonographic scoring systems are used among adults to predict oxygenation and to study pulmonary manifestations. 13 There has also recently been evidence of the use of such a scoring system to assess the need for surfactant administration in infants, with RDS. 14 Based on the evaluations, the neonatal lung sonographic score was completely correlated with pulmonary function indices such as oxygenation. However, it has been shown that the ability of lung sonographic scoring in predicting response to treatment and the need for surfactant administration in infants with RDS has been highly dependent on various factors such as gestational age. 15 Regarding the value of sonography, the diagnosis of neonatal RDS has demonstrated its diagnostic value and has been highly reported for this patient population.16,17 In a recent meta-analysis, the total evidence indicated a sensitivity of 92% (in the range of 89%–94%) and a specificity of 95% (in the range of 93%–97%) for the sonographic diagnosis of RDS. 18 Given that surfactant administration has a pivotal role in the treatment of neonatal RDS and the role of a lung ultrasonographic (LUS) scoring system has been well documented, it seemed important to apply this to the assessment of RDS. Therefore, the aim of this study was to determine the diagnostic accuracy of an LUS scoring system, in predicting the need for surfactant treatment, in preterm neonates suffering from RDS.
Materials and Methods
This cross-sectional study was conducted on neonates, suffering from RDS, at a gestational age over 30 weeks hospitalized, in the neonatal intensive care unit of the host hospital from March 2019 to April 2021. In this regard, infants with genetic or congenital anomalies; patients with congenital lung disease, severe sepsis, or meconium aspiration; or patients who received surfactant in the delivery room before being assessed by sonography were excluded from the study. Before entering a neonate into the study, written informed consent was taken from the parents, based on the approved study protocol by ethical committee of Shahid Beheshti University of Medical Sciences. Neonates with RDS were classified into two groups with and without the need for surfactant based on the fraction of inspiratory oxygen (FIO2). Neonates with RDS, who required assisted ventilation with a fraction of FIO2 of more than >0.4, were categorized in the group with the need for receiving surfactant (200 mg/kg of poractant, through the intubation-surfactant-extubation technique) and others were put in the group without the need for surfactant therapy. This threshold has been modified from the one suggested by European guidelines 19 (see Figures 1 and 2).
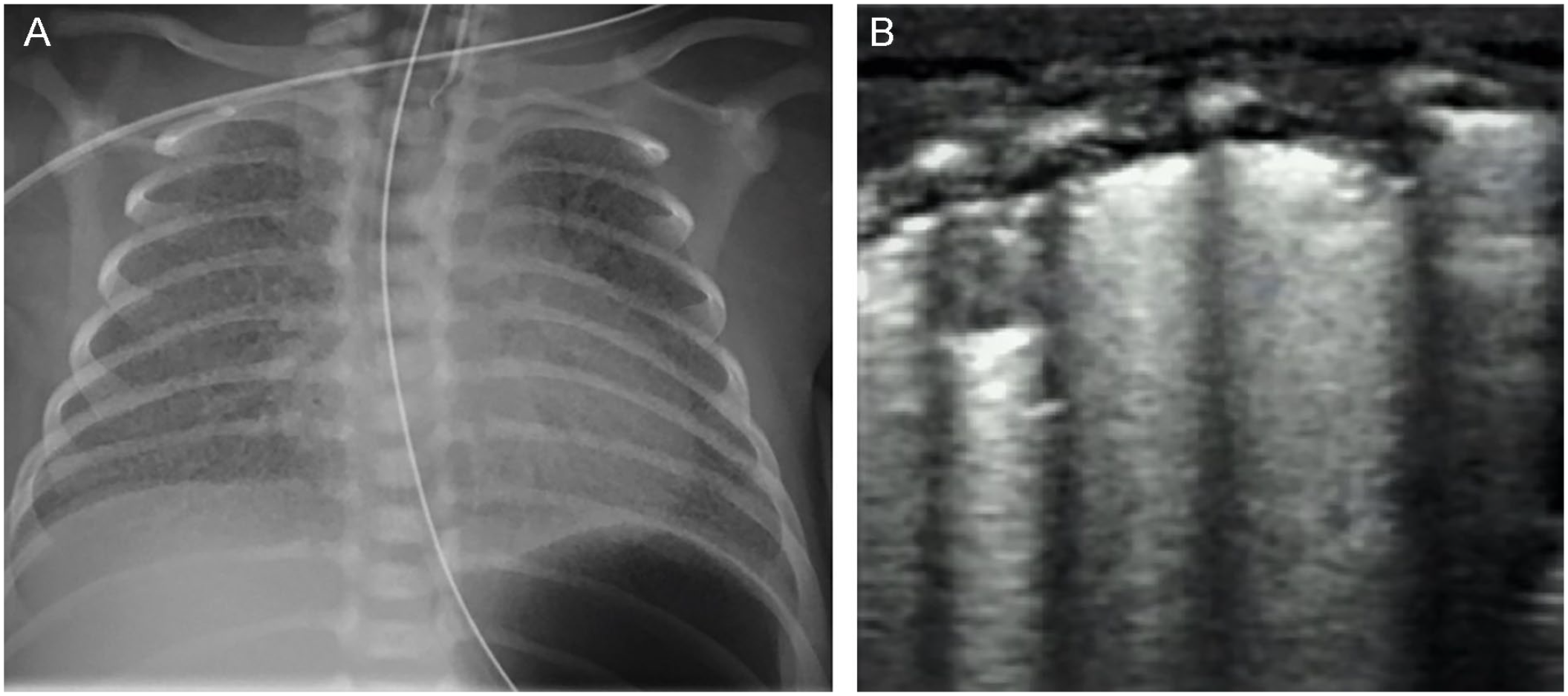
An example of chest radiograph (A) and the sonographic imaging appearance (B) of mild respiratory distress syndrome (RDS).
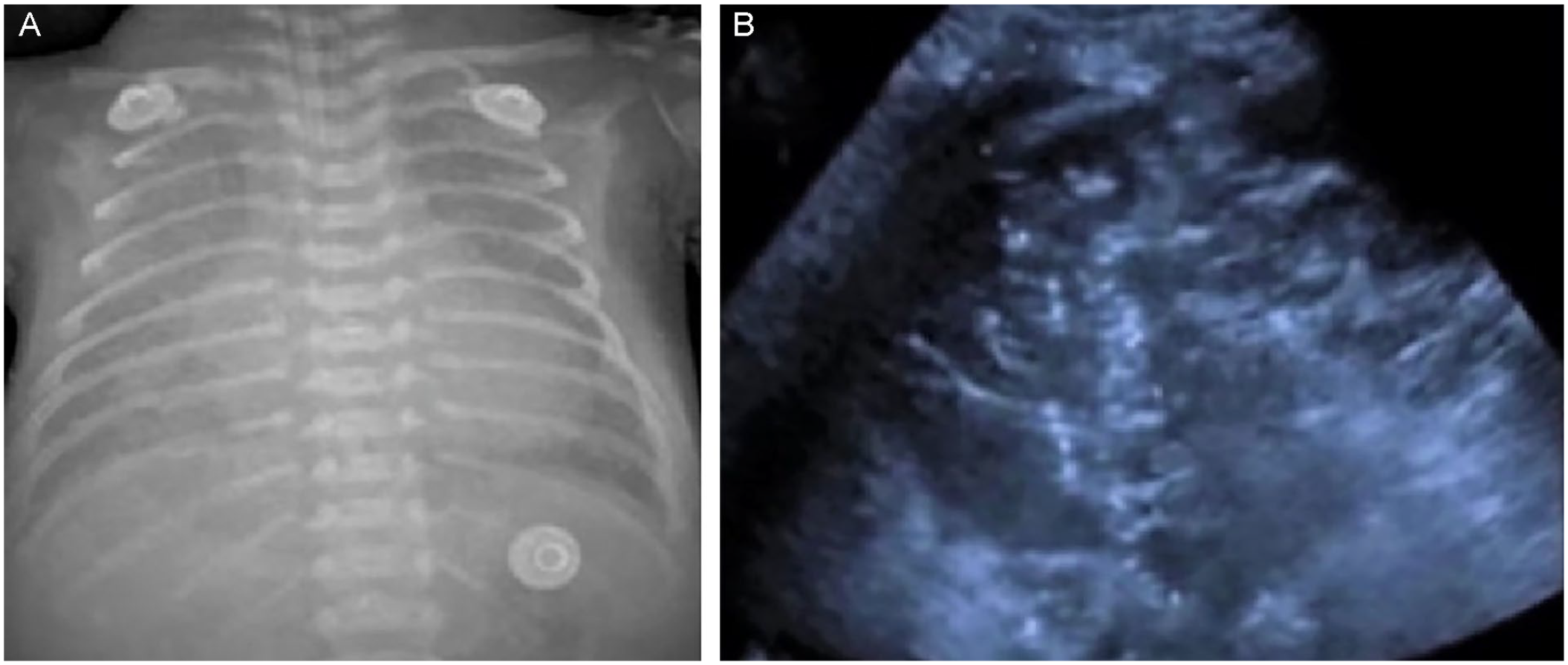
A chest radiography (A) as well as a lung sonogram (B) that demonstrates the appearance of severe respiratory distress syndrome (RDS).
LUS Imaging Protocol
A gray-scale sonogram was conducted by a diagnostic radiologist with 10 years of experience in doing pediatric ultrasonography. The radiologist was unaware of two groups of neonates with and without the need for receiving surfactant. The LUS was performed using a WS80A (Samsung Healthcare) ultrasound equipment system. The linear array transducer (5–10 MHz) was used for assessing the lungs of neonates. The LUS of neonates was done under bedside conditions, and then an LUS score was calculated for each of the neonates. According to the newly modified system by Szymański et al., 12 different lung fields are scored in the form of five levels. This provided a score of zero (A-profile), which indicated a normal lung; a score of one indicated a B-lines (B-profile); a score of two indicated a white lung; a score of three indicated a white lung with fluid alveologram; and a score of four indicated a white lung with consolidation (see Figure 3). In total, considering the four pulmonary fields anterior (left), anterior (right), posterior (left), and posterior (right), the final score is classified between 0 and 16. 12
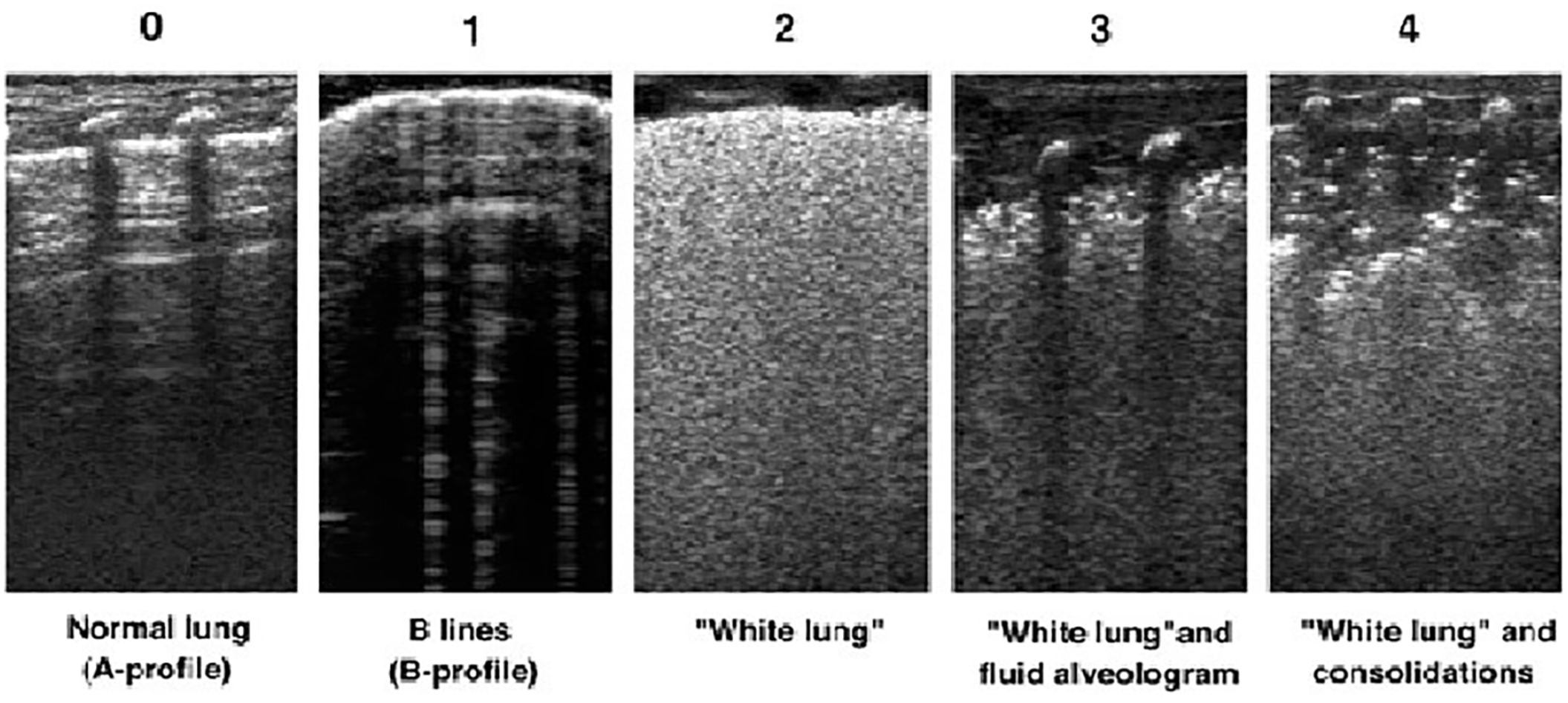
Diagnostic images provided demonstrate the lung ultrasonography scoring system in determining the severity of respiratory distress syndrome (RDS) (the scoring system is based on the work of Szymański et al). 12
Statistical Analysis
For statistical analysis, results were presented as mean ± standard deviation (SD) for quantitative variables and were summarized by frequency (percentage) for categorical variables. Continuous variables were compared using the t test or Mann-Whitney test, whenever the data have a non-normal distribution or when the assumption of equal variances was violated, across the study groups. The receiver operating curve (ROC) analysis was considered to determine the value of lung score to predict requiring surfactant therapy. In this regard, the best cutoff value for the score along with the sensitivity and specificity of this cutoff point was to be determined. A statistical P value of ≤.05 was determined and considered statistically significant. For the statistical analysis, the statistical software SPSS version 24 (SPSS Inc., Chicago, IL) was used.
Results
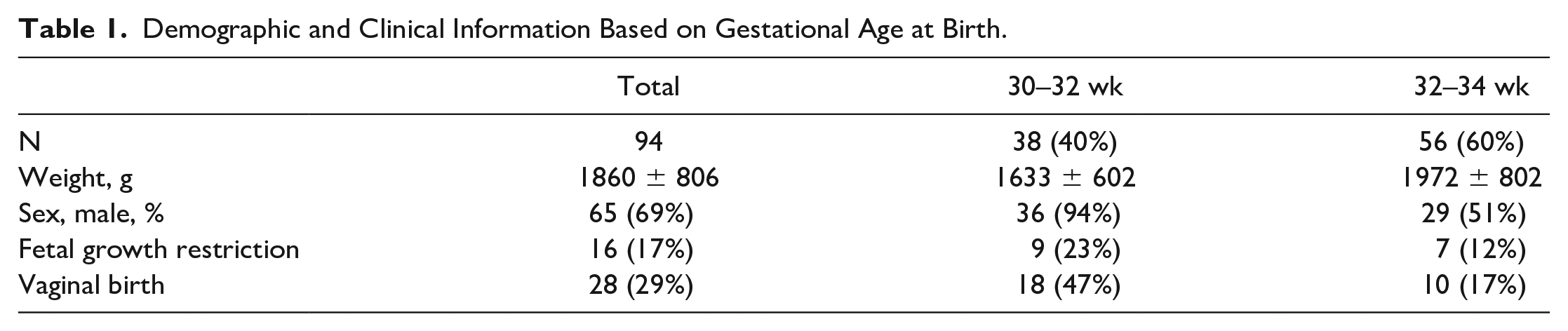
In this study, the cohort consisted of 47 neonates with RDS, who needed surfactant administration, and 47 neonates with RDS, without the requirement of surfactant administration, were included. Demographic and clinical details are provided in Table 1. There were 38 (40%) neonates with a gestational age of 30–32 weeks and 56 (60%) who were 32–34 weeks of age. The mean birth weight of cases was 1860 ± 806 g. There were 65 (69%) neonates who were of the male gender. Within the cohort, 16 (17%) patients had a history of fetal growth retardation, in which 9 (23%) were between 30 and 32 weeks of age; 28 (29%) of neonates were given birth vaginally (see Table 1).
Demographic and Clinical Information Based on Gestational Age at Birth.
The mean LUS scoring within the group with the need for surfactant and the group without the need for surfactant was 9.08 ± 3.09 and 4.12 ± 2.56, respectively, which showed a significant difference between the two groups (P < .001) (see Chart 1).
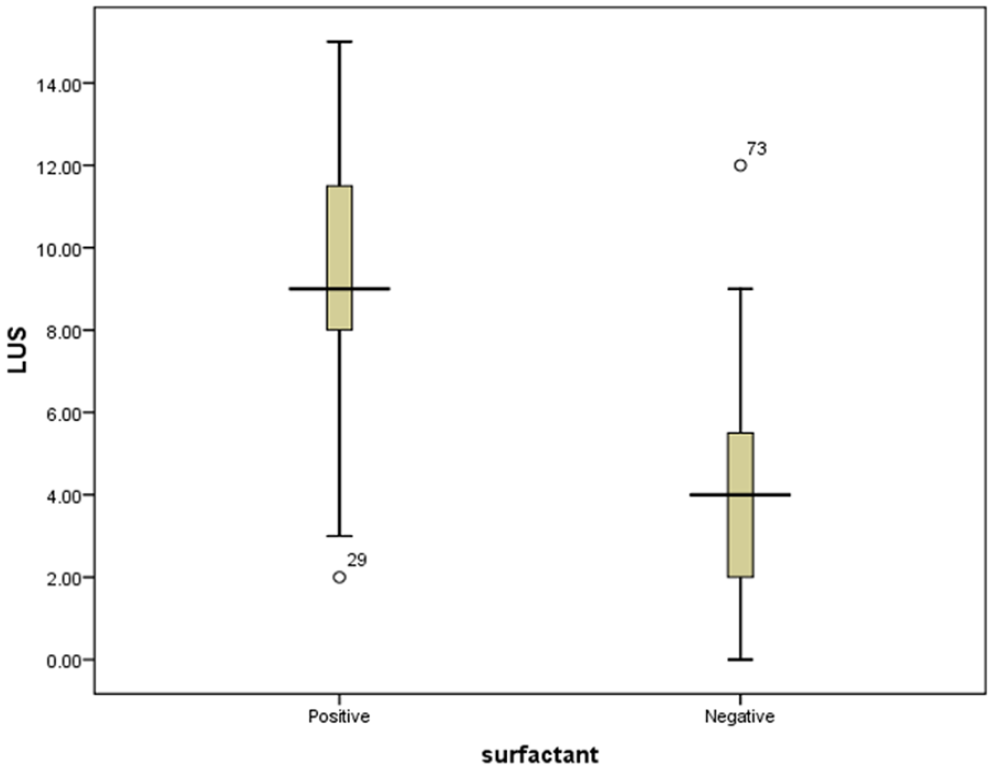
Mean lung ultrasonographic scoring in two groups of neonates with and without the need for receiving surfactant demonstrated as positive and negative, respectively.
Based on the analysis of the area under the ROC curve (AUC), the determination of LUS scoring had a high ability to predict the need for surfactant treatment (AUC = 0.885, 95% confidence interval [CI]: 0.816–0.954). Accordingly, the best cutoff point for LUS scoring in predicting the future need for surfactant treatment was 6 in neonates 30–32 weeks and 7 in neonates 32–34 weeks, with a sensitivity of 85.1%, 84% and a specificity of 87.2%, 88%, respectively. Based on these thresholds, LUS scoring for more than 6 in neonates 30–32 weeks, and 7 in neonates 32–34 weeks can predict a poorer outcome and the future need for surfactant therapy (see Chart 2 and Table 2).
Reliability of LUS Score to Be Used to Predict Surfactant Treatment.
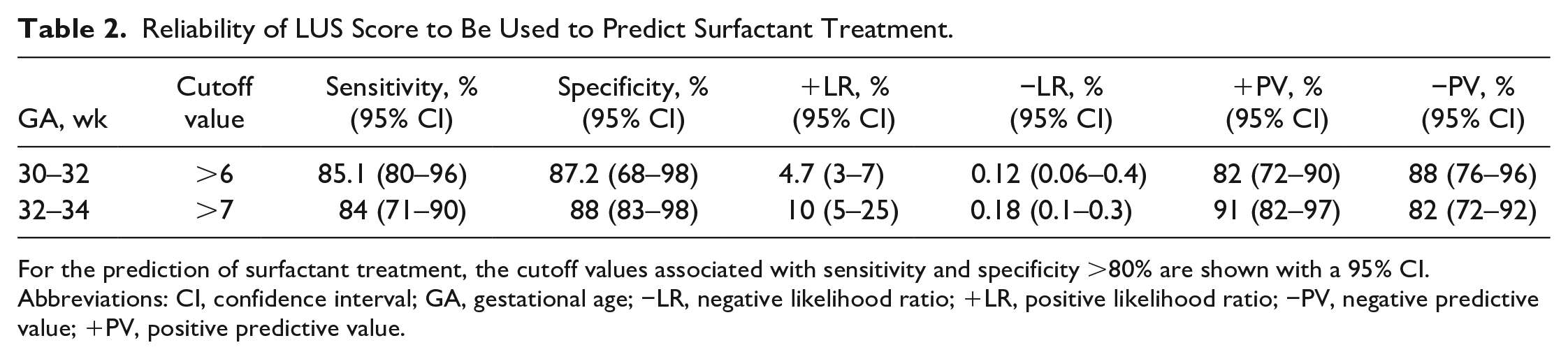
For the prediction of surfactant treatment, the cutoff values associated with sensitivity and specificity >80% are shown with a 95% CI.
Abbreviations: CI, confidence interval; GA, gestational age; −LR, negative likelihood ratio; +LR, positive likelihood ratio; −PV, negative predictive value; +PV, positive predictive value.
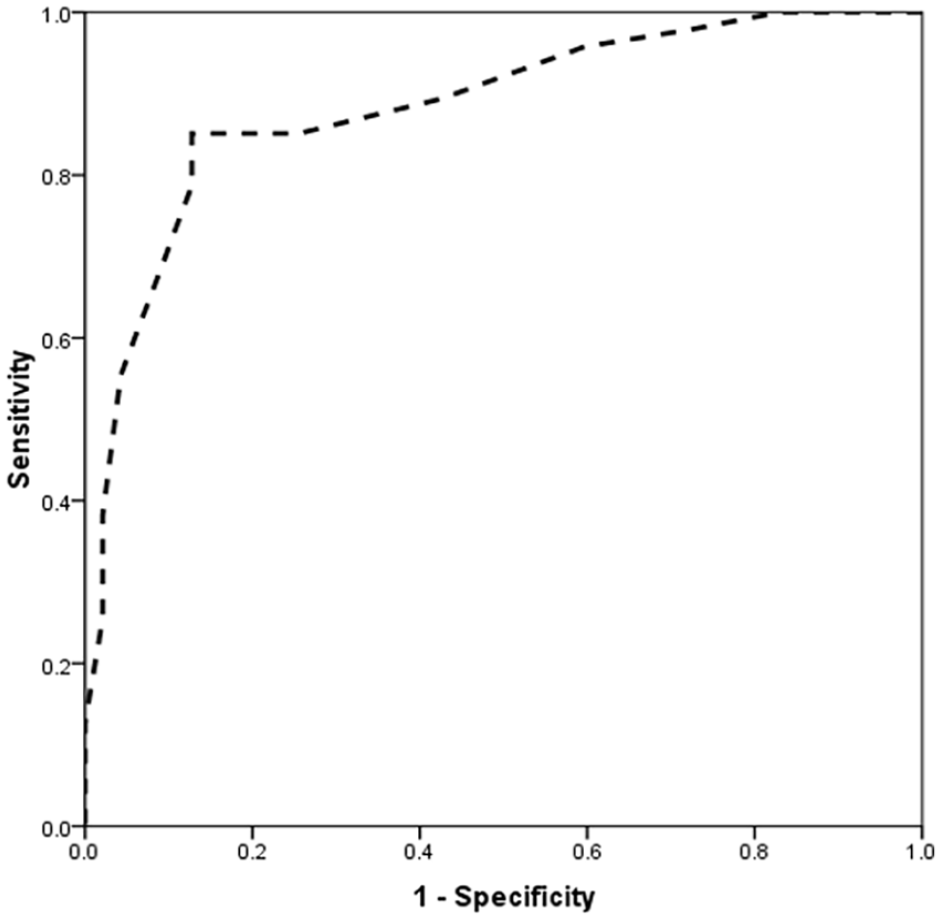
Analysis of the receiver operating curve in determining the lung ultrasonographic value in predicting the need for surfactant injection in infants with respiratory distress syndrome.
Discussion
Traditional and classical methods for assessing the need for surfactants in neonates with RDS include clinical guidelines (based on neonatal clinical manifestations) as well as radiographic evaluation of the neonatal chest. However, these methods have potential limitations. First, relying solely on clinical manifestations to determine the need for surfactant is not specific, as many pulmonary disorders, especially congenital heart and lung abnormalities, may confuse physicians in diagnosing pulmonary immaturity due to surfactant deficiency. Second, studies have shown that the likelihood of false negatives was greatly increased when using radiography. Therefore, in recent years, the use of sonograph in differentiating infants in need of surfactant has received special attention. Accordingly, the quantification of diagnostic sonographic findings and, in fact, the provision of a sonographic scoring system was meant to identify infants in need of surfactant treatment.
In the present study and in line with previous studies, in two groups with and without the need to use surfactant, it was important to evaluate the LUS and calculate the sonographic score for the lungs. In this regard, in addition to comparing the mean scores of the two groups, it was also vital to evaluate the diagnostic value of this score in distinguishing the two groups of neonates. Based on the present study results, the mean score of LUS in the group needing surfactant treatment was much higher than in patients without this requirement. Second, by analyzing the area below the ROC curve, it was demonstrated that the evaluation of the LUS score, in infants with RDS, was able to screen infants who needed treatment with surfactant. It should be noted that in the analysis of the AUC, values higher than 0.8 were considered as a definitive criterion for the value of the quantitative variable. A review of various studies showed that although in almost all of these studies, the high capability and value of LUS scoring in distinguishing the neonates of the two groups have been emphasized. The cut points related to this score were completely different, which can be due to a few important factors. First of all, most importantly, the performance, as well as the interpretation of LUS, was strongly influenced by the experience of the operator and radiologist, and it was obvious that both the interpretation of lung involvement and the determination of LUS scoring could be completely different based on this factor. Second, the neonatal clinical condition, especially their underlying clinical features, could also affect the score. In this regard, gestational age and birth weight should be considered important. But, in general, almost all studies have emphasized the value of LUS scoring in determining the subgroup of infants in need of surfactant treatment (but with different cut points from this score). In the study by De Martino et al., 20 the LUS scoring had high diagnostic accuracy to predict the need for the first dose as well as the repetition of the corresponding dose of surfactant. In this regard, the diagnostic accuracy of LUS scoring was 89% and 72%, respectively. In a study by Gregorio-Hernández et al., 21 the median score of LUS in infants receiving surfactant was much higher than in infants without surfactant which confirms the present study results. In the study by Perri et al., 22 the LUS scoring had a higher value than the radiographic score, in the need for surfactant treatment, with a sensitivity of 86% and a specificity of 88%. In the study of Brat et al., 23 infants less than 34 weeks had a cutoff score of four, on LUS, that predicted the need for surfactant injection. They were able to make such a prediction with 100% sensitivity and 61% specificity which was similar to our findings with a lower cutoff point. 23 The difference noted may be due to the LUS scoring system methods used and the diagnostic capability of the scoring system. In a study by Razak and Faden, 24 infants with an LUS score higher than five to six were found to need surfactant treatment, which was close to the results of the present study. Based on their results, this diagnostic value was much higher in infants with lower gestational ages, which was an emphasis on the potential effect of gestational age on the diagnostic accuracy of lung scores in predicting the need for surfactant treatment. Finally, in the study of Perri et al., 25 a 2-hour LUS score had a high value in predicting the need for surfactant injection, and accordingly, a score higher than seven had a sensitivity of 94% and a specificity of 60% for this purpose, which was closer to the cutting point in the present study. It is noted that in their study, the timing of postpartum sonographic evaluation was also emphasized as an important factor influencing the difference in the cutoff point of LUS score.
Limitations
This study was limited due to the study design and the sample size. Due to these limitations, generalizations should not be made, as these results are based on this cohort. However, repeated studies are encouraged to build higher levels of evidence.
Conclusion
This cohort study provides some evidence that may indicate the diagnostic value of LUS scoring in predicting the need for surfactant therapy, in neonates. In this regard, a score higher than six in neonates 30–32 weeks and seven in neonates 32–34 weeks should be further explored. These diagnostic cuff-off values may be indicative of the need for surfactant therapy with high sensitivity and specificity.
Footnotes
Ethical Approval
Before entering a neonate into the study, written informed consent was taken from the parents, based on the approved study protocol by ethical committee of Shahid Beheshti University of Medical Sciences.
Informed Consent
Before entering a neonate into the study, written informed consent was taken from the parents, based on the approved study protocol by ethical committee of Shahid Beheshti University of Medical Sciences.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.