
Abstract
Amyand’s hernia is a rare inguinal hernia where the appendix is trapped in the hernia sac. This uncommon hernia is most often revealed as an incidental finding, and the demonstration of this disease process is variable. This case study presents a scrotal sonogram of a 48-year-old male complaining of pain and swelling, without history of trauma. Sonographic images of the right inguinal region identified Amyand’s hernia that contained fat, free fluid, and the appendix. Treatment of Amyand’s hernia is highly debatable, but most cases are treated based upon classification that includes the state of the appendix, the patient’s age, septic state, and if any peritoneal involvement was identified.
A hernia is a condition in which part of an organ is displaced and protrudes through the wall of the cavity containing it. Hernias are a common condition, more often seen in males. 1 Males are more susceptible because of a persistent abdominal wall opening that allows the spermatic cords and testicular vessels to pass through. Most abdominal wall hernias are inguinal hernias (75%-80%) and inguinal repair is the most performed surgery worldwide.1–4 This case study is focused specifically on an inguinal hernia known as Amyand’s hernia. Amyand’s hernia is a rare inguinal hernia with the appendix trapped within the hernial sac. 5 Amyand’s hernia is diagnosed in 0.1% of all inguinal hernias and an inflammation of an appendix is only seen in 0.1% of cases.4–10 It is postulated that a herniated appendix has a higher risk of becoming inflamed due to the hernial neck being narrow and causing restricted blood flow, which leads to inflammation and edema. 4 Asgill et al. 11 explained how Amyand’s hernia was first described in 1731 by French surgeon Rene-Jacques Croissant de Garengeot. In 1735, it was also mentioned by Dr Claudius Amyand after he completed the first surgical appendectomy of a perforated appendix, within the inguinal canal. 5 For the purpose of this case study, the term Amyand’s hernia is used to describe the appearance of a normal appendix, within an inguinal hernia.
Case Report
A 48-year-old male presented as an outpatient for a scrotal sonogram for pain and swelling. The patient reported no previous trauma, and a sonogram was performed using a LOGIQ E Ultrasound equipment system (GE HealthCare, Waukesha, Wisconsin) and a 9.0 MHz linear-array transducer. The scrotal sonogram demonstrated normal measurements of each testicle, homogeneous echogenicity, and no definitive masses or lesions (see Figure 1). There were varicosities noted in the right scrotum (see Figure 2), but the left scrotal sac was normal. Incidentally, there was a large right inguinal hernia discovered containing fat, free fluid, and the appendix, known as Amyand’s hernia (see Figures 3–5). The wall of the appendix measured 5.0 mm and manual compression did not demonstrate reduction of the structure. Further exploration of the left inguinal canal confirmed normal anatomy and no evidence of any soft tissue masses or abnormal anatomy (see Figure 6). The patient was referred to a general surgeon for surveillance and treatment options.

A bilateral testicular sonogram that demonstrated the echogenicity of the tissue without the presence of masses or lesions.
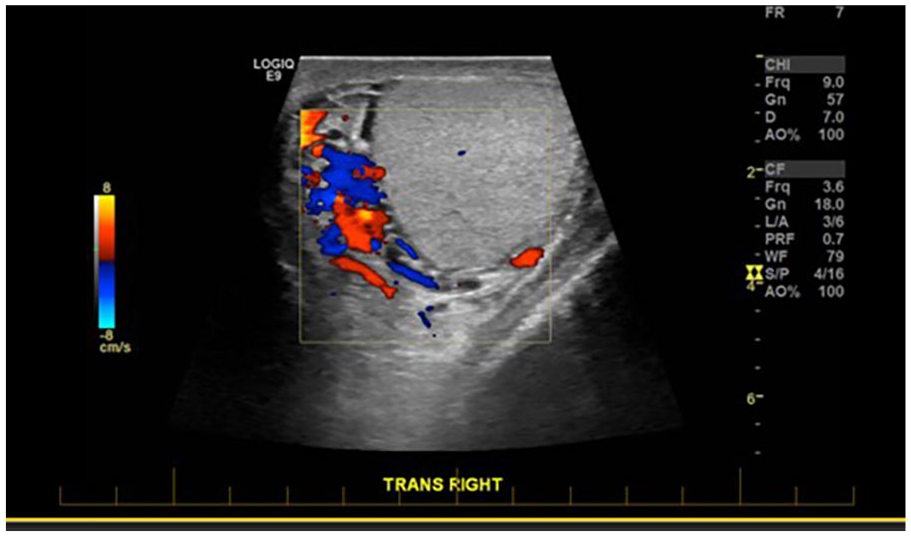
A transverse testicular sonogram that demonstrates a right varicocele.
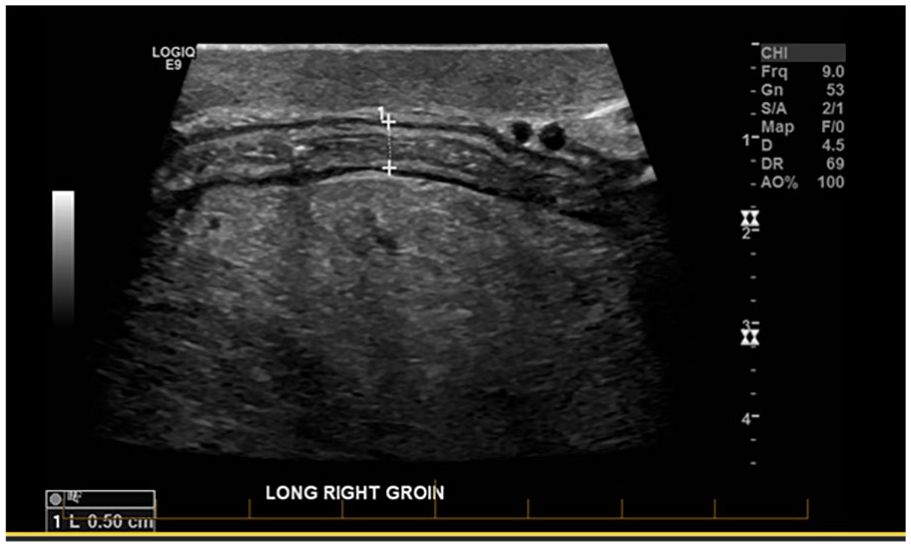
A sagittal image of the right groin that illustrated the appendix, within the inguinal canal.
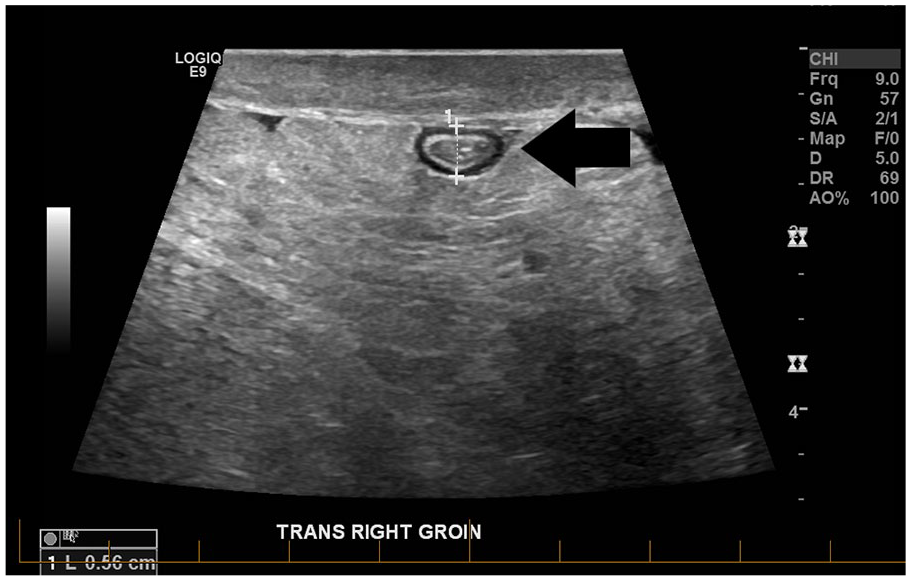
A transverse image of the right groin that depicted the appendix, within the inguinal canal.
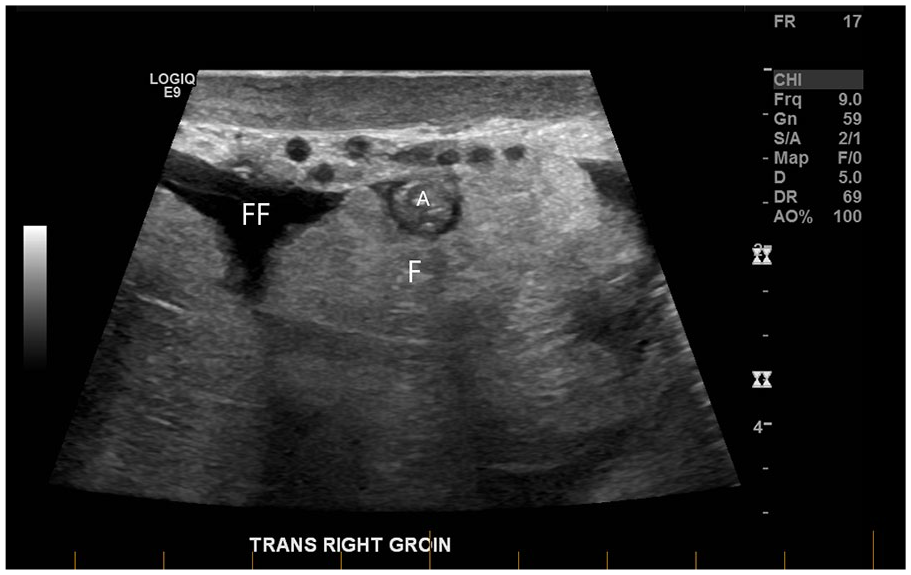
A transverse image of the right groin that demonstrated free fluid (FF), fat (F), and appendix (A), within the inguinal canal.
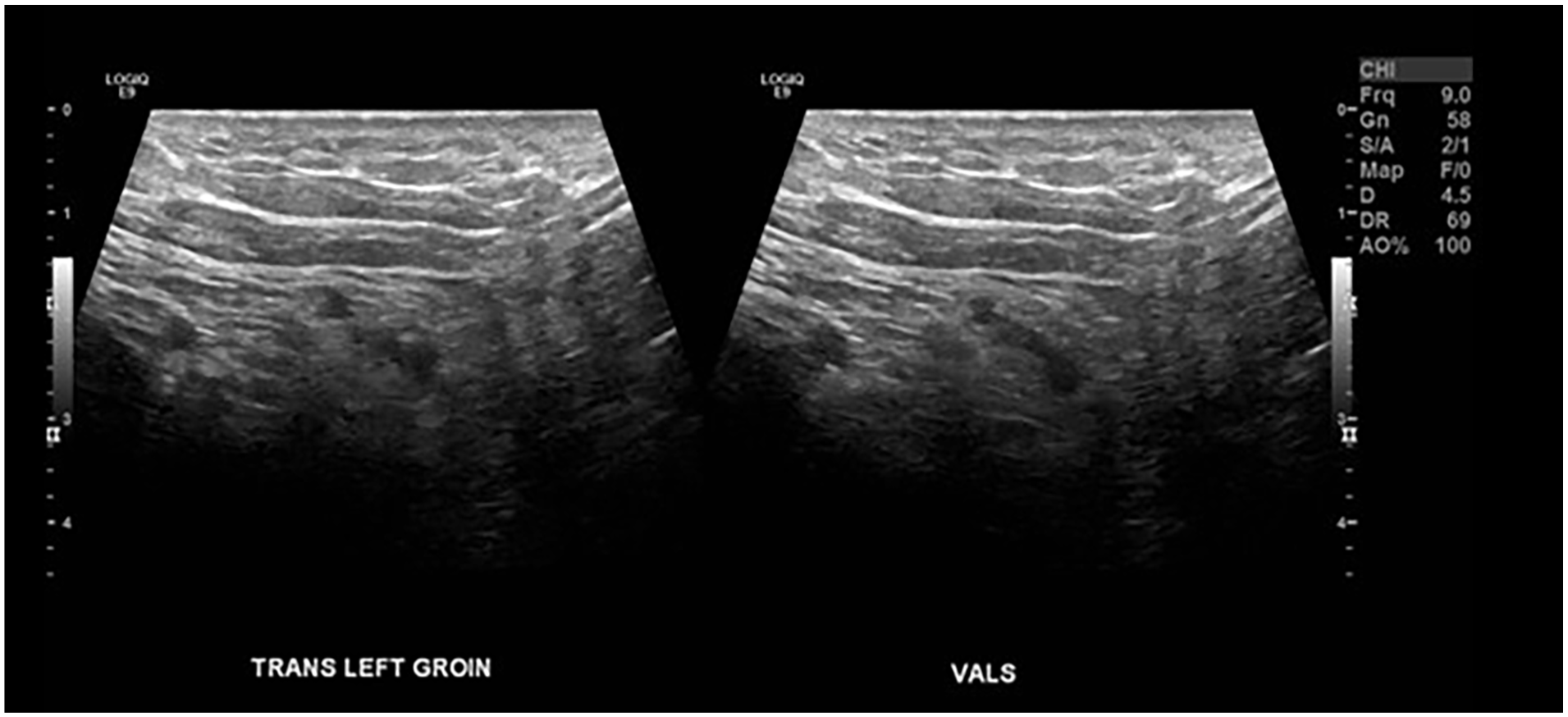
A transverse image of normal left groin during the patient performing a Valsalva maneuver.
Discussion
Amyand’s hernia is most often seen in male pediatric patients; however, there are cases reported at all ages, and when diagnosed in females, it is found at a higher incidence during the postmenopausal period.4,5 The normal appendix is found on the right side; therefore, Amyand’s hernia is most often found in the right lower quadrant; however, it has rarely been discovered in the left lower quadrant. 12 Intestinal rotation is one cause it may originate on the left side, and it may also be identified in infants with low birth weight, as their colon is not adequately fixed. 10
Management of Amyand’s hernia is debatable, with advantages and disadvantages for each treatment choice. 12 However, with mortality rates near 30%, it is essential to understand this rare condition as to not delay diagnosis and treatment.4,12,13 In 2007, Losanoff and Basson 14 recommended a four-part classification method to describe Amyand’s hernia along with recommended treatments.5,14 Each hernia was classified according to the state of the appendix (normal vs. inflamed), patient’s age, septic state, and if there was peritoneal involvement. In type 1, patients present with a normal appendix, and if they are a child or a young adult, appendectomy is to be performed along with a mesh hernioplasty. If it presents as an adult, then a reduction of the hernia and mesh hernioplasty is recommended. The criteria for a type 2 classification are documented when patients present with acute appendicitis and limited inflammation within a hernia. The plan of care for these patients is appendectomy through the hernia with a hernioplasty. Type 3 patients present with acute appendicitis and peritonitis, and it is recommended these patients have appendectomy through laparotomy and hernioplasty. Finally, patients classified as type 4 will have acute appendicitis and other related or unrelated abdominal pathology. These patients are recommended to have an appendectomy though hernia or laparotomy and appropriate diagnostic workup depending on abdominal pathology.5,14,15 See Table 1 as a reference for each typology.
The Classification, Description, and Management of Amyand’s Hernia. 14
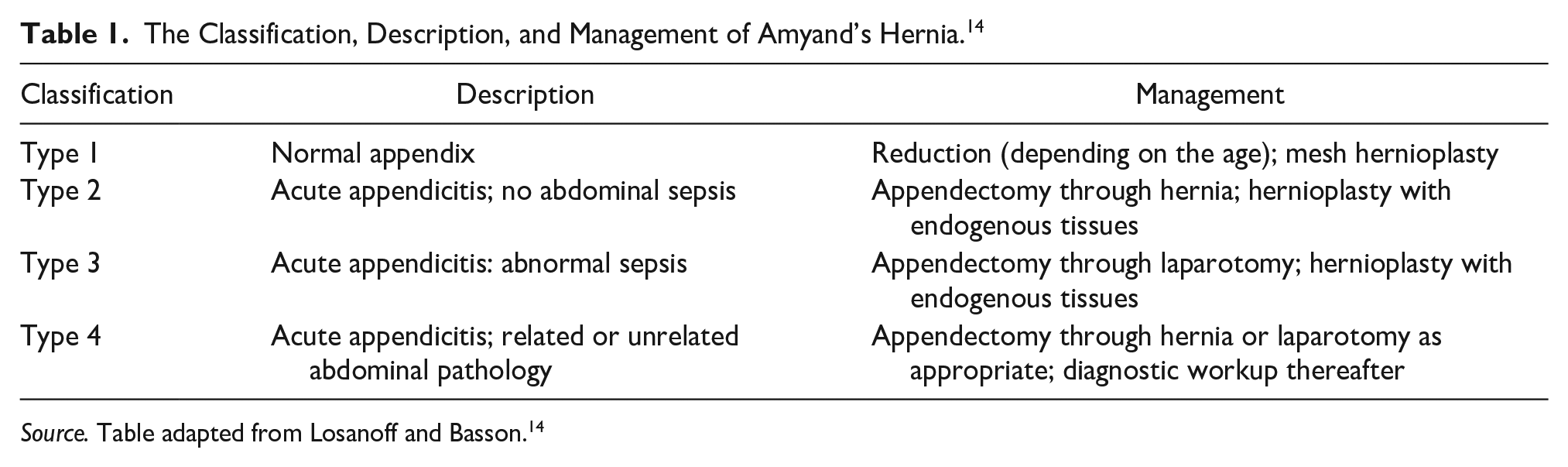
Source. Table adapted from Losanoff and Basson. 14
Clinical presentation of an inguinal hernia may present as a bulge or swelling in the groin area1,11 with right lower quadrant tenderness. 15 However, the diagnosis of Amyand’s hernia is often difficult due to nonspecific symptoms and its rare occurrence. 10 Frequently, Amyand’s hernia is an incidental finding. 5 According to the literature, only 1 in 60 cases have been diagnosed preoperatively and the majority of them are discovered intraoperatively.15,16
The imaging choices used to identify Amyand’s hernias are primarily sonography and computed tomography (CT). 1 However, some literature reports magnetic resonance imaging (MRI) can also used to diagnose Amyand’s hernia.1,17 These imaging techniques are most often used if clinical examination leaves doubt of proper diagnosis or where priority is early surgery. 5 Literature supports CT as the imaging modality of choice in evaluating Amyand’s hernia especially in complicated cases.4,5,12 Sonography is reported as a good imaging choice for examining lumps or bulges in the inguinal area 1 because it is of low cost, 5 it lacks ionizing radiation, 10 and it is portable. 1 In addition, sonography is the imaging modality of choice for pediatric patients to reduce radiation exposure. 10
Amyand’s appendix sonogram is positive if a noncompressible tubular structure inside the hernial sac is found. Sonography of the normal appendix is ≤6 mm long showing echogenic mucosa, hypoechoic muscularis mucosa, echogenic submucosa, hypoechoic muscularis propria, and echogenic serosa. 10 If wall thickening is seen with free fluid and hyperemia, this suggests an acute appendicitis. 5
Conclusion
This case study identified an incidental finding of Amyand’s hernia. Amyand’s hernia is difficult to diagnose because of nonspecific symptoms and its rarity. Sonographers must possess knowledge of normal anatomy of the groin area to identify a normal or inflamed appendix that has herniated in the inguinal region. If Amyand’s hernia is suspected, the sonographer should further access the inguinal canal with a high-frequency linear-array transducer, attempt to image any content identified in the hernia sac, and evaluate for a noncompressible tubular structure. Losanoff and Basson’s 14 four-part classification system is a great tool to help surgeons determine the appropriate treatment for Amyand’s hernia, and sonography and CT are essential imaging modalities to positively identify a herniated appendix.
Footnotes
Ethics Approval
Ethical approval was not sought for the present study because this information was researched and developed to be shared for medical or educational purposes.
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.