
Abstract
Intracranial hypertension (IH) is an important cause of secondary brain injury, and it is often associated with poor outcomes; due to that monitoring of intracranial pressure (ICP) is essential for the management of neurocritical patients. Although invasive methods have been the gold standard for ICP monitoring, recent non-invasive ultrasonography techniques have been used to estimate ICP. Among the most used methods are the measurement of the diameter of the optic nerve sheath and transorbital ultrasonography to evaluate papilledema. This presented case is of a patient with refractory IH due to subarachnoid hemorrhage, measured through an intraventricular catheter. A transorbital sonogram was performed and showed the presence of papilledema.
Intracranial hypertension (IH) is an important cause of secondary brain injury, and it is associated with poor outcomes; therefore, its monitoring is essential for the management of neurocritical patients. The gold standard for monitoring intracranial pressure (ICP) are intraventricular catheters. However, some non-invasive methods such as those based on ultrasonography have been developed. Among those are the measurement of the diameter of the optic nerve sheath and varied diagnostic methods, based on transcranial Doppler. 1 Another diagnostic technique used to evaluate the presence of IH is the interrogation of the optic disc, with transorbital ultrasonography (TOUS). Under normal conditions, there is no evidence of any alteration at the junction of the retrobulbar optic nerve and the globe (see Figure 1). When IH develops, papilledema can be seen as an elevation of the optic disc. 2 This case is provided of a patient with IH and associated papilledema.
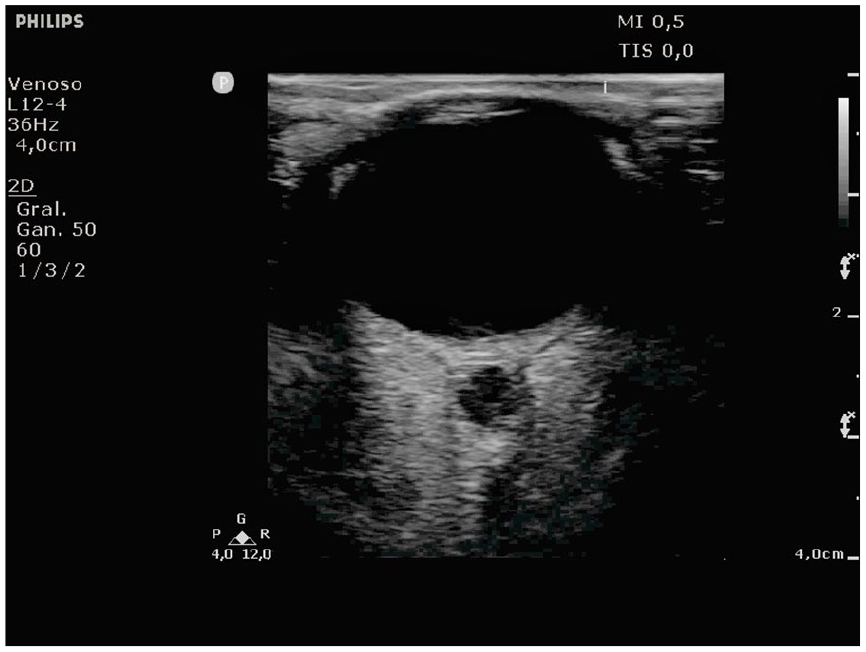
A grayscale transorbital ultrasonogram that demonstrates normal eye anatomy without the presence of papilledema.
Case Report
A 36-year-old female patient with no relevant medical history presented to the emergency department, with a severe headache and ultimate coma. Orotracheal intubation was done at her arrival, and she was connected to a mechanical ventilator. A computed tomography (CT) was completed and showed a subarachnoid hemorrhage; therefore, a digital angiography was performed. This examination discovered a basilar artery aneurysm that was managed with the placement of several platinum coils. The patient was admitted to the neurocritical care unit. During her stay, she developed basilar artery vasospasm with severe brain damage and hydrocephalus that required placement of an intraventricular catheter. The patient presented with an increased ICP of up to 67 mmHg, despite the treatment. She was evaluated by the neurosurgery service with no criteria for surgical treatment. TOUS was performed using a linear transducer with a frequency of 7.5 to 12 MHz that was placed gently on the upper eyelid using a thick layer of ultrasound gel. The ultrasound equipment system was adjusted using the preset for venous vascular studies, as it gave better image definition. The examination time and gain of the equipment were adjusted according to the “as low as reasonably applicable (ALARA)” principle to protect the eye. The transducer was adjusted to display the optic nerve. The optic nerve sheath diameter (ONSD) was measured a 3.0 mm behind the eye globe, since it is the site of maximum pressure change within the nerve. Electronic cursors were placed at the transition from the dark to the hyperechoic regions. A value less than 5.8 mm was deemed normal according to previously published studies. 3 The optic disc height was measured as the distance between the peak of the disc and its junction with the posterior surface of the globe. An ONSD diameter of 5.8 mm (see Figure 2) and an optic disc height of 3.0 mm (see Figure 3) was seen in both the eyes of the patient. The patient presented with clinical and sonographic features that were compatible with cerebral circulatory arrest. She was declared brain-dead under the Argentinian guidelines, adopted by the host hospital.
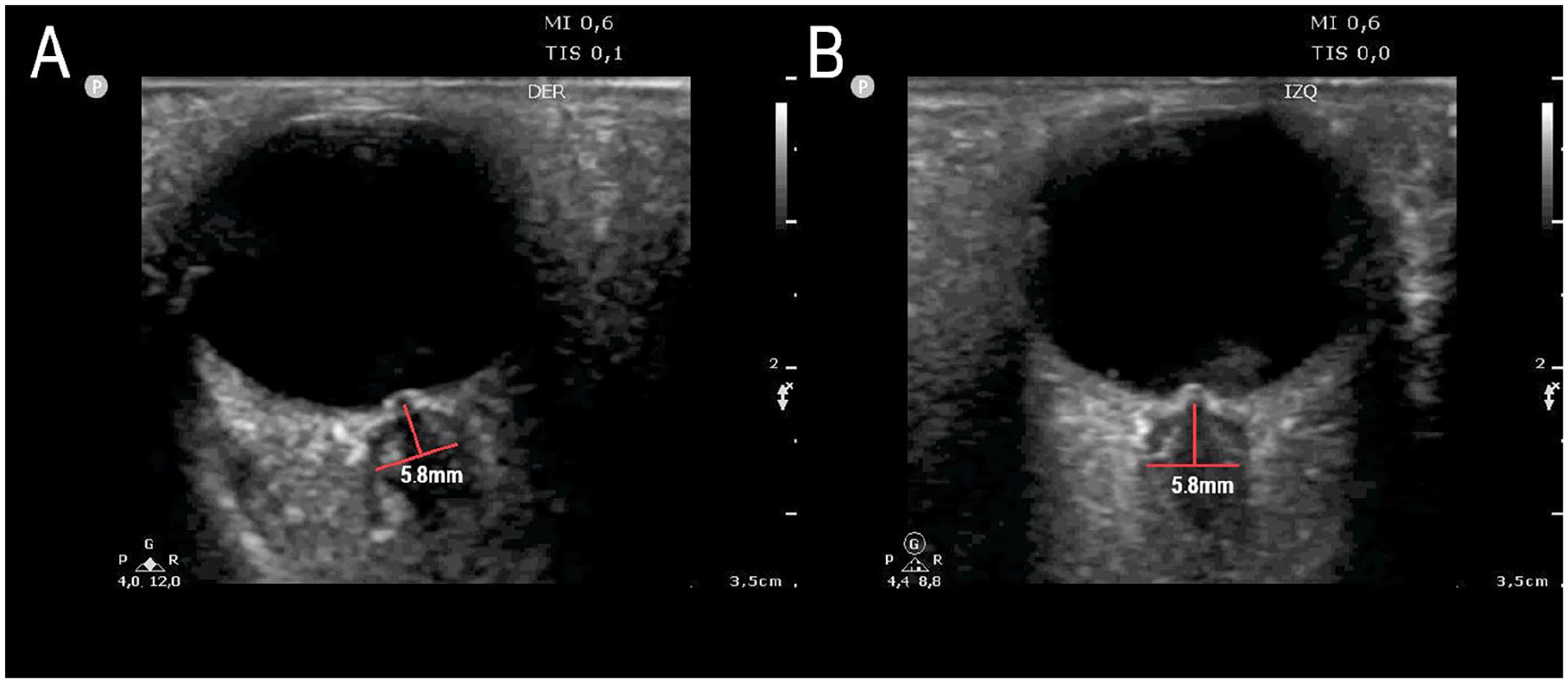
A grayscale transorbital ultrasonogram showing an optic nerve sheath that measures 5.8 mm and an optic disc elevation which is compatible with papilledema, on both the patient’s right (A) and left (B) sides.
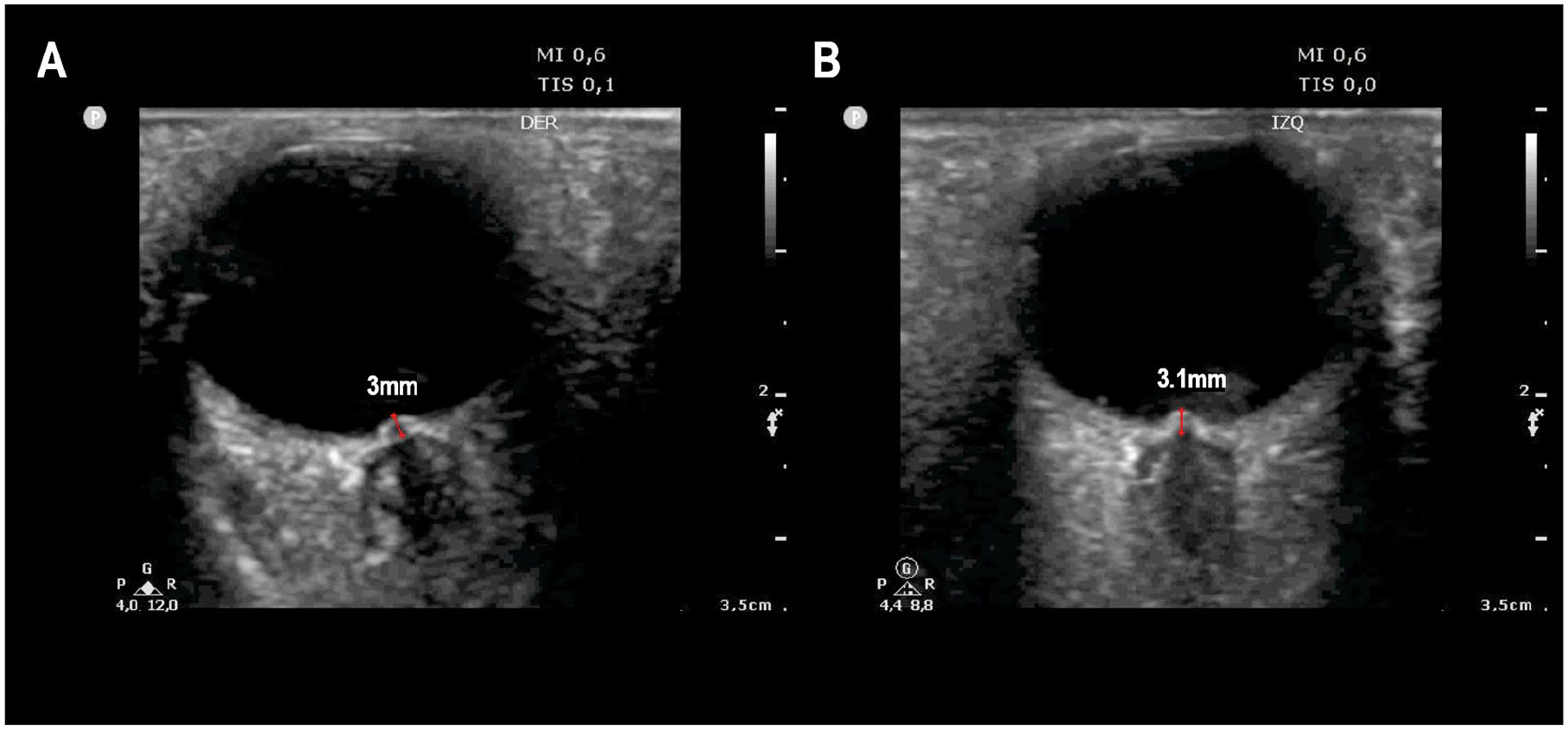
A grayscale transorbital ultrasonogram that measured the optic disc elevation of 3.0 mm and 3.1mm on the patient’s right (A) and left (B) sides, respectively.
Discussion
Although invasive diagnostic methods are the gold standard for ICP measurement, several non-invasive alternatives have been developed, and sonography can be used to estimate it. One of those diagnostic techniques is the TOUS evaluation of the optic disc.
Usually, the meningeal covering of the brain extends into the orbit and encircles the optic nerve, which is why changes in ICP are transmitted to the optic disc, through the subarachnoid space. 4 The development of papilledema is nothing but the optic nerve edema caused by increased ICP that was transmitted to the subarachnoid space, surrounding the optic nerve.4,5
Clinical evaluation of papilledema involves fundoscopy and visual examination of the optic nerve. The severity of papilledema is determined by the appearance of the disc margin, its height, and vascular pattern. The Frisen scale was created to standardize the grading of papilledema, but its clinical evaluation is subjective and frequently varies between observers. 5 The usefulness of orbital CT for the diagnosis of papilledema has also been reported. It is evidenced as a “bulging” of the terminal optic sheath into the posterior side of the eye. 6 A CT examination has the advantage of being able to assess the cause of IH. However, papilledema can be difficult to objectify due to low imaging resolution.
The potential of a magnetic resonance imaging (MRI) examination to offer gross visualization of the eye and optic nerve has drawn attention and become an additional diagnostic choice. MRI has stronger soft tissue contrast when compared with a CT image of the same area. However, papilledema has been technically difficult to assess because of its small size. 7 It must be taken into account that transferring critical patients to make these kinds of studies is complex and can be dangerous. After more than 20 years, TOUS is still widely and safely used for an ophthalmic examination. 8 It is considered the first-line diagnostic tool to detect papilledema because it is safe and can be performed several times with no need to move a patient to the imaging department. It visualizes papilledema as an elevation of the optic disc, using a linear transducer. 9 In the study of Teismann et al., 10 an optic disc elevation greater than 1.0 mm predicted optic disc edema, with a sensitivity of 73% and a specificity of 100%. Mohson et al. 11 showed that the presence of optic disc bulging, without measuring its elevation, has a sensitivity of 61.1% and specificity of 100% for the detection of IH. It is important to take into account that the presence of papilledema may be due to other causes such as inflammatory diseases, infection, infiltrative conditions, and microvascular infarction. Also, it should be noted that ICP elevation does not cause disc swelling in the acute setting; therefore, in this situation, significant ICP elevation may not manifest yet as papilledema. 10 Therefore, the diagnostic findings should always be interpreted in the clinical context of the patient. Also, as mentioned when performing TOUS, it is important to take into account the ALARA principle due to the mechanical and biological risks of exposing the eye to high-frequency transducer output. 12
In the present case, ultrasonography allowed for visualization of papilledema in a patient with severe refractory IH and could not be moved to the imaging department. Based on a limited literature review, this may be the first case of papilledema demonstrated using TOUS, as a sign of IH, in a patient with subarachnoid hemorrhage and a poor outcome.
Conclusion
This patient case study helps to illustrate that TOUS can be used to evaluate the presence of papilledema in a simple and non-invasive diagnostic manner. It also can complement the diagnostic information obtained by other diagnostic imaging techniques.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Approval for this case study was waived in accordance with the local regulations because this study is a case of a single patient and did not include protected health information, data analysis, or testing of a hypothesis, and was de-identified.
Informed Consent
Written consent was obtained from the patient before the publication of this case study.