
Abstract
Objective:
The research aim was to analyze the function of focused cardiac ultrasonography (FoCUS) in diagnosing a pulmonary embolism (PE) and contributing to the practice of emergency medicine and expediting the treatment of PE.
Materials and Methods:
In this prospective and observational study, Wells scores were calculated on those patients who presented to the emergency department over the last 2 years and were evaluated with a preliminary diagnosis of PE, as well as the biochemical values and imaging techniques. In all cases, FoCUS was used as the diagnostic tool.
Results:
A PE was detected in 38 (63.3%) of 60 patients. According to Wells score, it was determined that 5 (8.3%) patients had low-risk, 41 (68.3%) had medium-risk, and 14 (23.3%) had high-risk Wells score. There was a statistically significant correlation between the existence of PE and the findings of FoCUS in patients with right ventricular dilatation (P < .001). According to Wells score, moderate-risk individuals with PE were more likely to exhibit right ventricular dilatation (P = .003).
Conclusion:
The FoCUS results either alone or in conjunction with the Wells score, reviewed in the diagnosis of PE, effectively indicated and directed the diagnosis and treatment of patients admitted to this particular emergency department.
Patients admitted to a hospital emergency department (ED), with symptoms that include shortness of breath, tachypnea, chest pain, and syncope, should be evaluated and confirmed for the presence of a pulmonary embolism (PE). When a PE is misdiagnosed, it is a life-threatening condition that is one of the reversible causes of mortality, lacks a distinct clinical picture, and is therefore frequently ignored. Patients who do not receive the correct diagnosis and therapy have a mortality rate between 25% and 30%, although this rate drops to 2% after treatment. 1
Diagnostic imaging techniques are crucial in identifying and treating patients with acute respiratory failure. Chest radiographs and a computed tomogram (CT) are the most popular diagnostic tools used for this purpose. Even though portable radiography systems also allow patients to be evaluated, where they are being observed, this is not an option for CT. In the case of conducting a CT, patients must be transferred to the radiology department, which may be dangerous for emergency patients, with hemodynamic abnormalities. Computed tomographic pulmonary angiography (CTPA) is one of the other diagnostic tests performed in the ED, which is a popular and reliable method for imaging vascular structures, particularly for pulmonary vessels. However, diagnostic monitors at the bedside are required for a patient with hemodynamic instability. 2 In EDs, bedside ultrasonography (USG) is helpful in identifying or determining various causes of right ventricular dilatation, heart failure, shock, and volume measurement. The sensitivity and specificity of transthoracic echocardiogram (TTE) in diagnosing PE are 50% to 60% and 80% to 90%, respectively. 3 The diagnosis is strengthened by the presence of mobile and convoluted thrombi trapped in the right ventricular regions. Transthoracic echocardiogram features such as right ventricular dilatation, right/left ventricular asynchrony, McConnell’s sign, D-shaped septum, thrombus, and early systolic notch may guide emergency physicians to the diagnosis of PE.4,5 For the emergency diagnosis of patients with suspected hemodynamically unstable PE, current guidelines recommend that focused cardiac ultrasonography (FoCUS) be performed at the bedside, for the patient who has right ventricular dysfunction, thrombus, right ventricular dilatation and accept this as significant for the diagnosis of PE. 6 It is also recommended that an immediate CTPA examination be done, and if not, then they consider it as a PE and initiate the treatment accordingly. 6
Patients need to be assessed for the likelihood of PE based on specific risk factors. Diagnostic confirmations or risk calculations are made using criteria such as Wells (See Table 1), Geneva scores, or Pulmonary Embolism Rule Out Criteria (PERC). Current guidelines recommend that CTPA, be accessible in global EDs, as the most definitive method for diagnosing PE in hemodynamically stable patients with a high-risk score and a suspicion of PE. However, the D-dimer test should primarily be conducted on patients with low and moderate risk scores, and if the test is positive, additional investigation is recommended. Nonetheless, 40% of all PE patients have no risk indicators, and PE is diagnosed in roughly 10% of people deemed to be at low risk based on these scores. 6 Plasma D-dimer levels have a strong negative predictive value. However, as they may arise in numerous situations, such as aging, cancer, and infection, the trust of doctors in this test is debated, and most physicians require additional research to strengthen their diagnosis. 7
The Wells Scoring System.
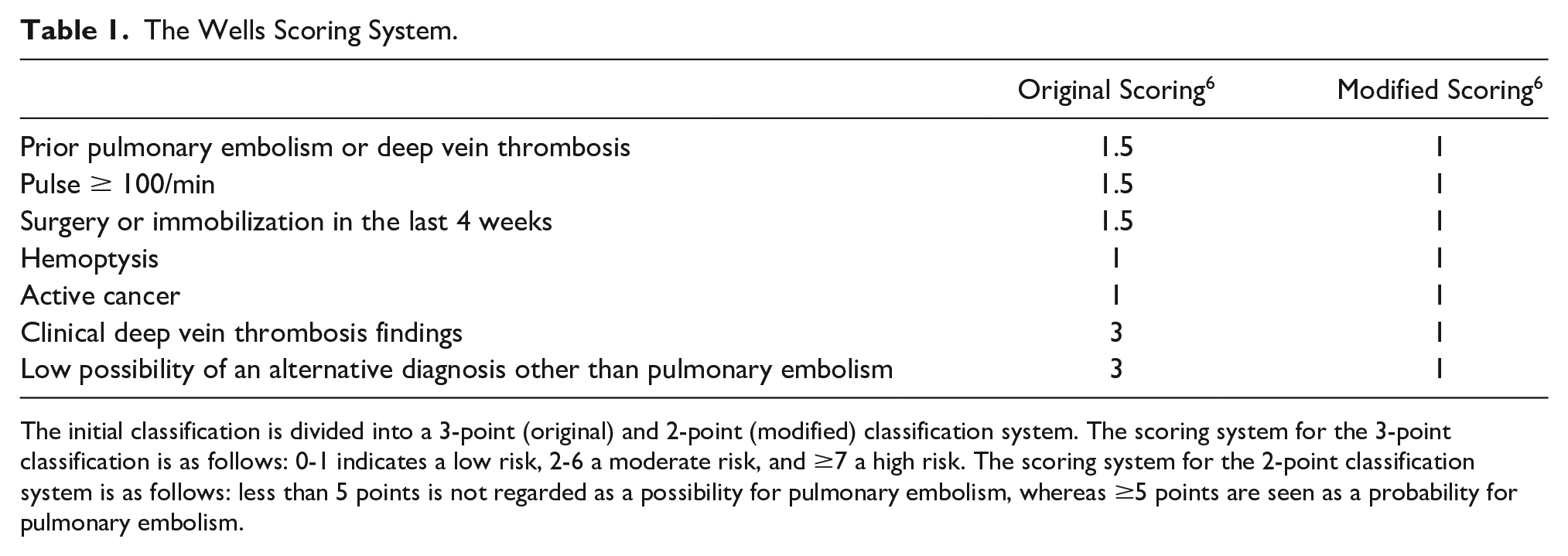
The initial classification is divided into a 3-point (original) and 2-point (modified) classification system. The scoring system for the 3-point classification is as follows: 0-1 indicates a low risk, 2-6 a moderate risk, and ≥7 a high risk. The scoring system for the 2-point classification system is as follows: less than 5 points is not regarded as a possibility for pulmonary embolism, whereas ≥5 points are seen as a probability for pulmonary embolism.
Focused cardiac ultrasonography is essential for differential diagnosis and identification of PE in patients presenting to the ED with respiratory distress, syncope, chest discomfort related to acute respiratory failure, and altered hemodynamics. Focused cardiac ultrasonography is beneficial for assessing the presence of pericardial effusion, thrombus, valve movements, relative chamber width, cardiac function, and volume status. There are insufficient data in the published literature about the clinical correlation between FoCUS and the diagnosis of PE, in the ED. The aim of this study was to determine the effectiveness of FoCUS findings in the diagnosis of PE. In addition, it was important to compare these findings with the Wells score and other methods (clinical findings, biochemical data) for diagnosing a PE.
Materials and Methods
The host university’s Faculty of Medicine Noninvasive Clinical Studies Ethical Committee, granted approval for this prospective, observational study. The researcher conducting the study was qualified in basic and advanced USG and has sufficient knowledge and experience on cardiac sonography. The entire study was conducted by the same investigator, who also performed bedside FoCUS, on all patients enrolled in the study.
Patients aged over 18 years old who were presented to the ED with complaints such as respiratory distress, chest pain, fainting, and followed up with the differential diagnosis of PE due to medical history, examination, Wells score, and had CTPA as a diagnostic follow-up, between the dates February 1, 2019, and February 27, 2021. The lead investigator performed FoCUS and venous compression ultrasonography (VCU) using the ultrasound equipment system’s cardiac and linear transducers, before the patients had been transported to CTPA. The patients’ demographic information, medical history, examination findings, Wells scores, laboratory results, and CTPA results were recorded.
Patients under 18 years of age, without written consent to participate, patients who were not deemed suitable or had contraindications for radiocontrast material (kidney diseases or allergic to radiocontrast material etc.) and who could not undergo CTPA because the CT unit in the host hospital was not suitable for morbid obesity patients, were all excluded from the study.
Focused Cardiac Ultrasonography
The patient was turned slightly to the left, in their bed. The transducer cursor was placed in the left, third, and fourth intercostal spaces and pointed toward the patient’s right shoulder. The heart was reviewed in the parasternal long-axis (PLAX) view; after that view, the transducer was rotated at a 90° angle. The transducer was held so that the cursor was pointed toward the patient’s left shoulder and then moved into the parasternal short axis (PSAX). The heart was evaluated through the subxiphoid window by placing the transducer under the left nipple where the best heartbeat was acquired, through the apical four chambers with the cursor on the patient’s left and putting the transducer under the xiphoid, over the left lobe of the liver. The ejection fraction (EF) of patients with asymmetrical or irregular left ventricular contractions and inadequate valve movement was determined to be reduced, whereas the EF of individuals without these symptoms was deemed sufficient. In addition, the vena cava inferior (VCI) diameter and collapse rates were assessed by positioning the transducer perpendicular to the left lobe of the liver, under the xiphoid, with the cursor pointing toward the patient’s head (See Table 2). Patients with right ventricular/left ventricular end-diastolic transverse diameter measurements >1.0 in apical four chambers, were deemed to have right ventricular dilatation. In these scanning windows, the D-shaped septum, the right ventricle’s contractile activity, and intracardiac thrombus were also assessed. The results were evaluated statistically. For VCU examination, the inguinal and popliteal regions of all patients were investigated using a compression ultrasonographic approach centered on two points: the inguinal and popliteal regions (See Figure 1).
The Volume Evaluation of Patients Using a FoCUS, According to the Measurement of the Vena Cava’s Inferior Diameter and Amount of Venous Collapse.
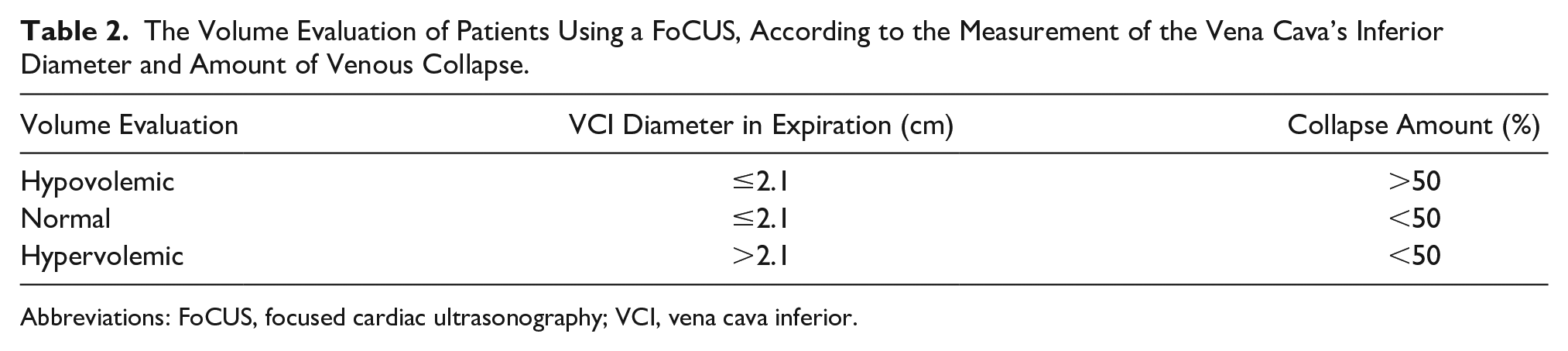
Abbreviations: FoCUS, focused cardiac ultrasonography; VCI, vena cava inferior.
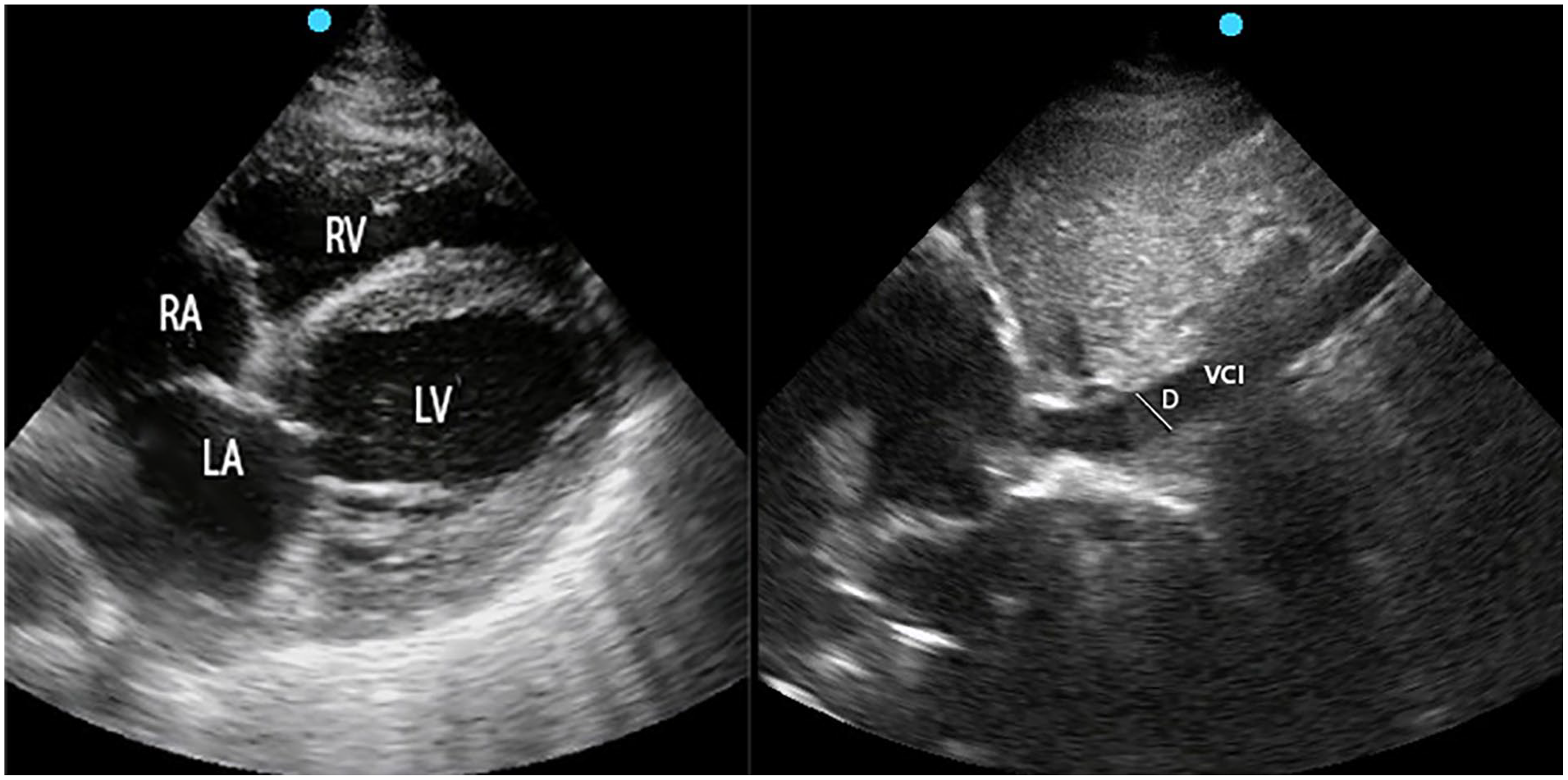
A sonographic apical 4 chamber view and a view of the inferior vena cava, which is measured based on the image at the xiphoid scanning window. D, Diameter; LA, Left atrium; LV, Left ventricle; RA, Right atrium; RV, Right ventricle; VCI, Vena cava inferior.
Statistical Analysis
The data were statistically analyzed using IMB SPSS software, version 23.0. Continuous measurements were summarized as mean, standard deviations, and minimum-maximum values, while categorical measurements were summarized with values and percentages. In order to compare categorical variables, the chi-square or Fisher’s exact tests were employed. The Student’s T-test was used for variables with a parametric distribution, whereas Mann–Whitney U-test was employed for variables without a parametric distribution. In all tests, the statistical significance level was set a priori at P < .05.
Results
Sixty participants were consented and took part in the study. The descriptive information of this cohort was that 32 participants (53.3%) were male, while 28 (46.7%) were female. The average age of the male participants was 56.9 ± 18.1, while the average age of female participants was 63.0 ± 18.3. The history of long-term disease was present in 54 participants (90%). When evaluating the long-term disorders of the patient cases, cardiovascular system diseases (46.7%) were the most prevalent, followed by cancer (36.7%) and respiratory system diseases (25%). There was no significant difference between the presence of long-term disease (P = .284), cardiovascular system (P = .142), or malignancy (P = .281), and the presence of PE (P > .05); the incidence of respiratory system diseases such as asthma, chronic obstructive pulmonary disease (COPD), and interstitial lung disease was lower in those diagnosed with PE (P = .011). When the risk scores of all patients according to Wells scoring was taken into consideration, it was observed that 5 (8.3%) patients had a low-risk score, 41 (68.3%) had a medium-risk score, and 14 (23.3%) had a high-risk score. The patients’ mean Wells scores were found to be 4.53 ± 2.5.
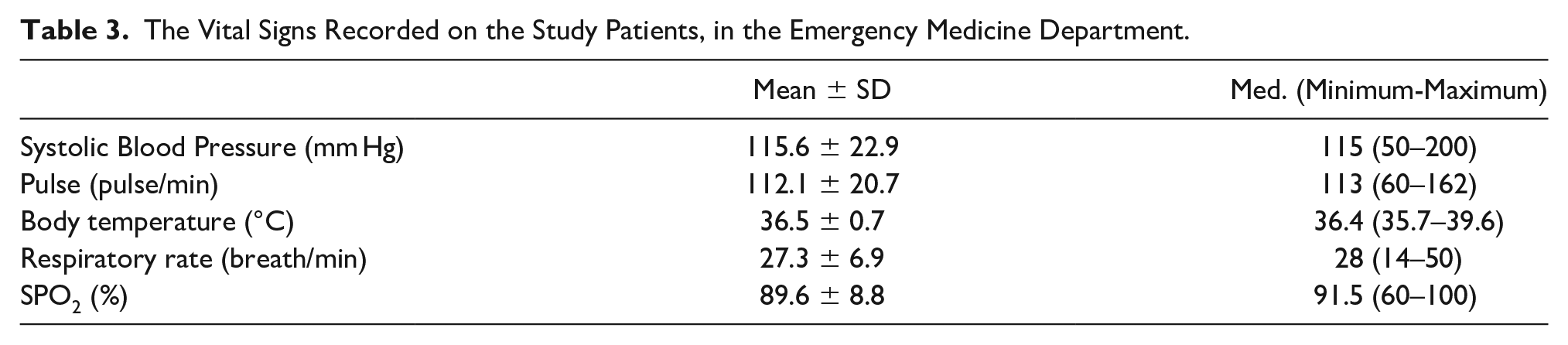
When the mean values of all patients’ vital signs were evaluated, it was discovered that the study participants were hypoxic, tachypneic, and tachycardic (See Table 3).
The Vital Signs Recorded on the Study Patients, in the Emergency Medicine Department.
In the FoCUS evaluation of all patients, 56 patients were found to have sufficient EF, 26 patients were found to have right ventricular dilatation, and 32 patients were found to have normal VCI (See Table 4).
A Bar Chart That Displays the FoCUS Diagnostic Results of the Study Patients.
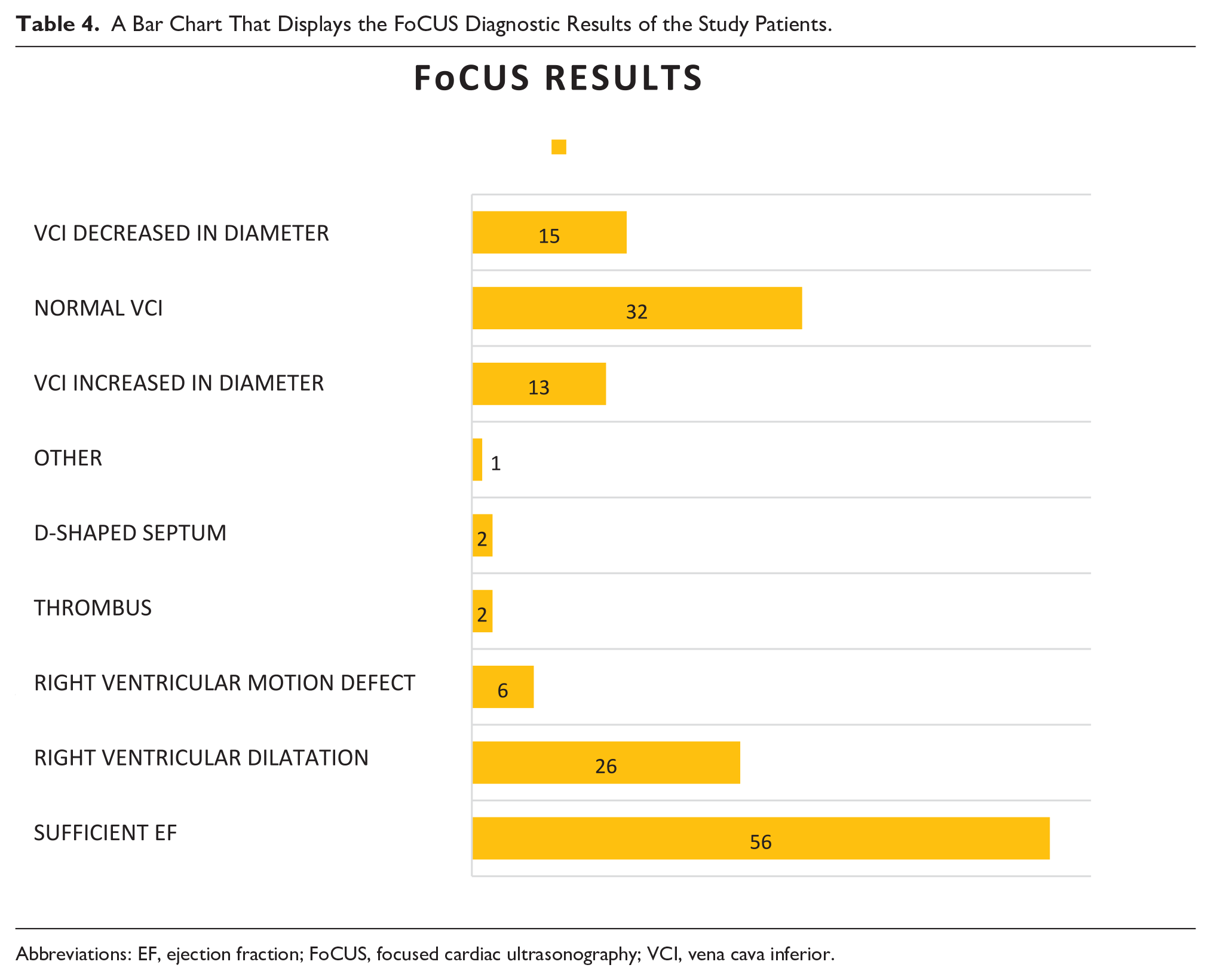
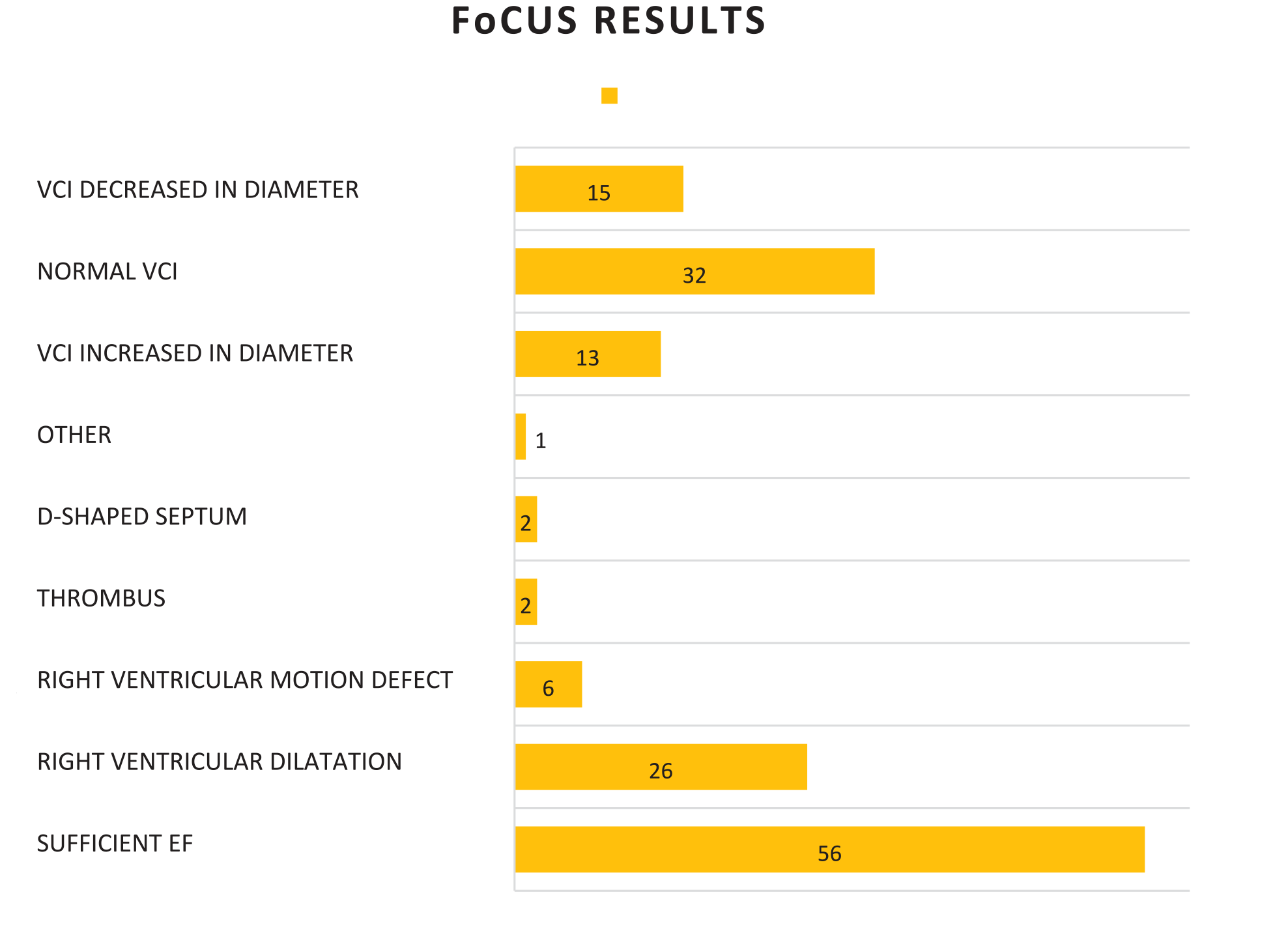
Abbreviations: EF, ejection fraction; FoCUS, focused cardiac ultrasonography; VCI, vena cava inferior.
According to the results of CTPA, PE was diagnosed for the first time in the ED in 38 (63.3%) patients. The identification of PE in the CTPA examination was statistically substantially greater (P = .003) in patients with a Wells score of moderate-risk and right ventricular dilatation in FoCUS results (See Table 5 and Figure 2).
The Wells Score and the Examination for the Presence of a Pulmonary Embolism.
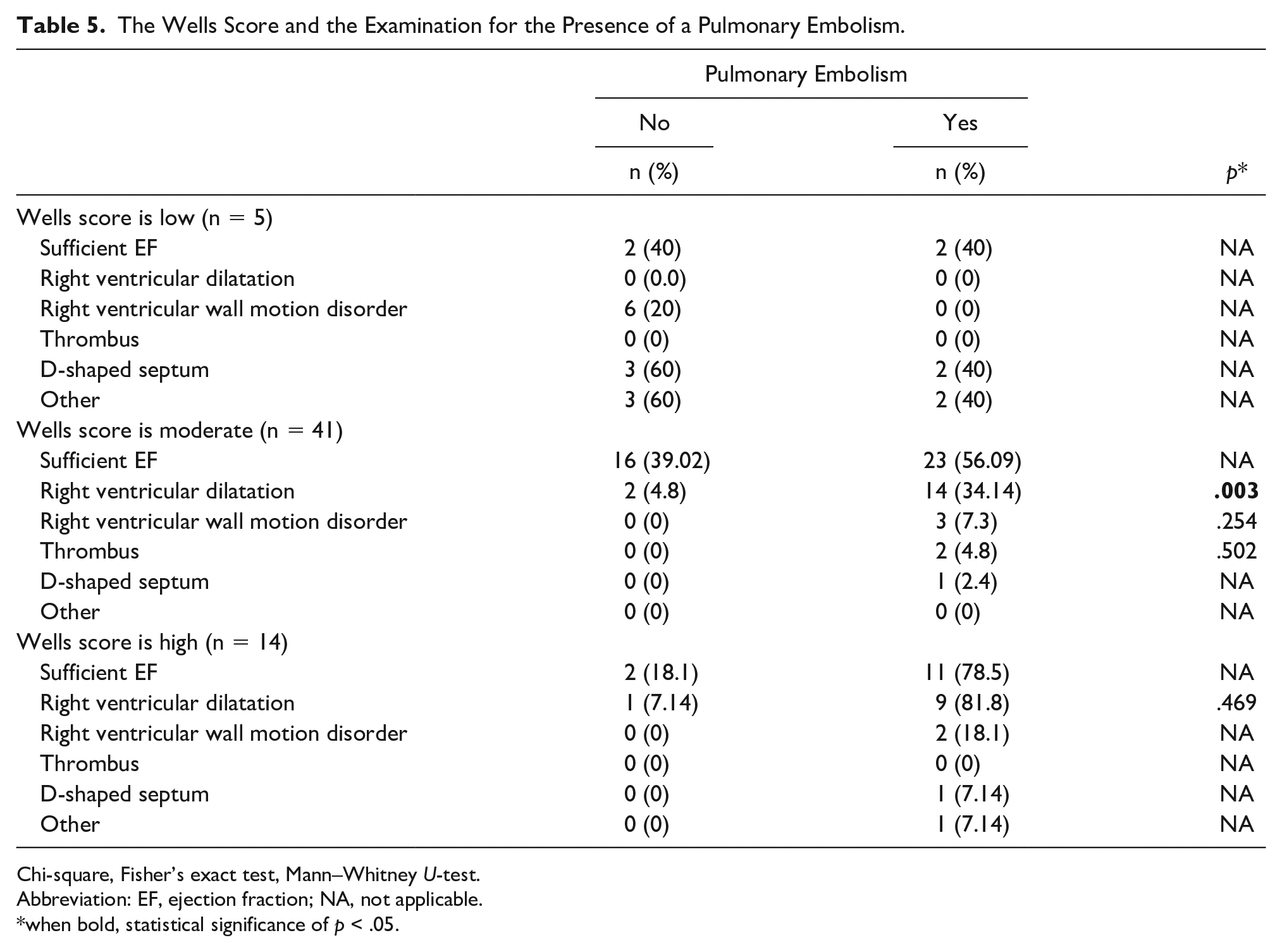
Chi-square, Fisher’s exact test, Mann–Whitney U-test.
Abbreviation: EF, ejection fraction; NA, not applicable.
when bold, statistical significance of p < .05.
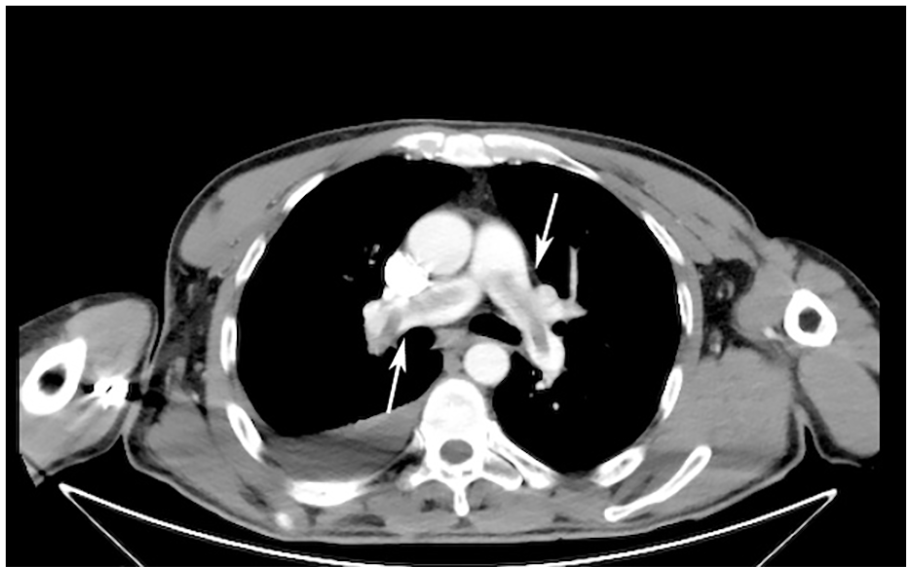
A computed tomographic pulwmonary angiography image that demonstrates a saddle-type pulmonary embolism.
When the PE diagnosis was examined according to the FoCUS findings, it was found that the observation of right ventricular dilatation was statistically significant in PE diagnosis (P < .001) (See Tables 6 & 7; Figure 3).
The FoCUS Diagnostic Findings and the Examination for the Presence of a Pulmonary Embolism.
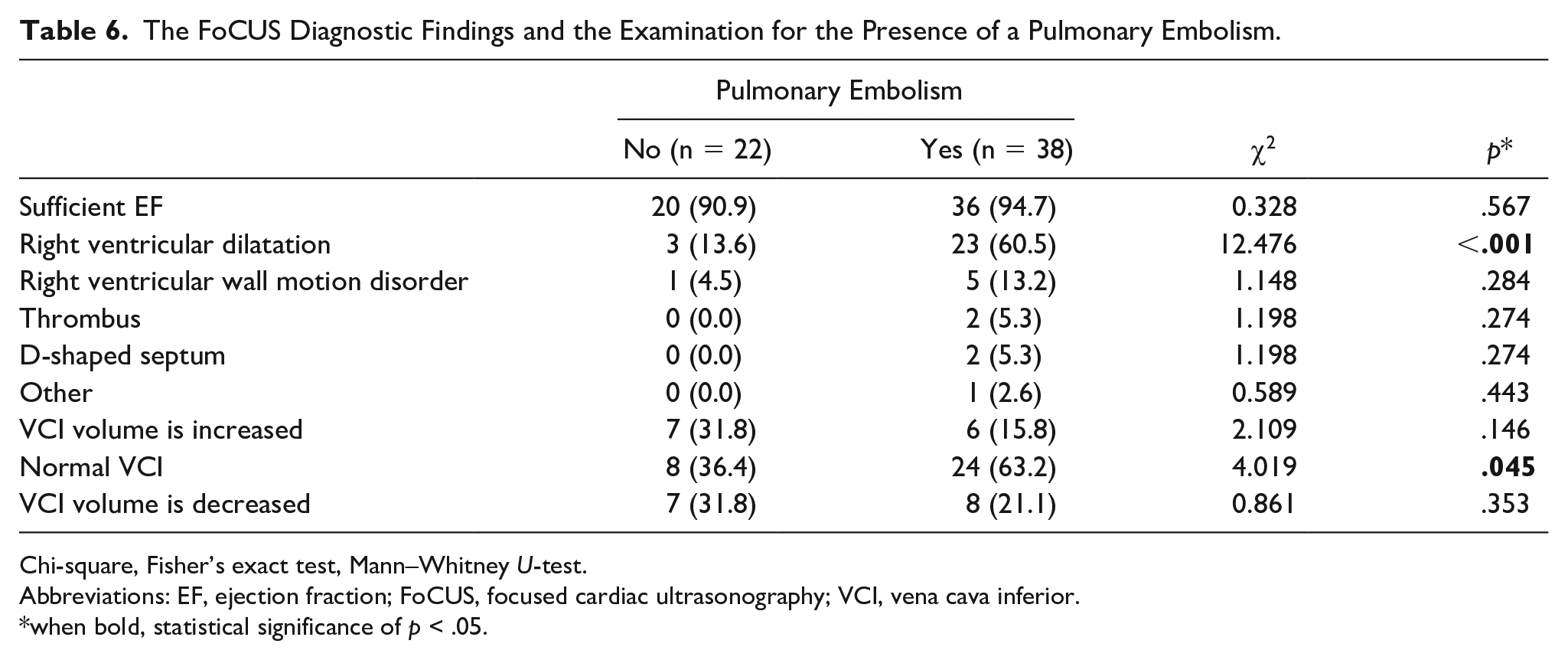
Chi-square, Fisher’s exact test, Mann–Whitney U-test.
Abbreviations: EF, ejection fraction; FoCUS, focused cardiac ultrasonography; VCI, vena cava inferior.
when bold, statistical significance of p < .05.
The Vascular Compression Ultrasonography (VCU) Findings and the Differences Between Embolism Groups While a DVT was Detected in 8 Patients as One-Sided in the Inguinal Area (13.3%) and Seven Patients as One-Sided in the Popliteal Region. Thus in a Total of 15 Patients (25%), Double-Sided DVT was Not Detected in Any of the Patients.
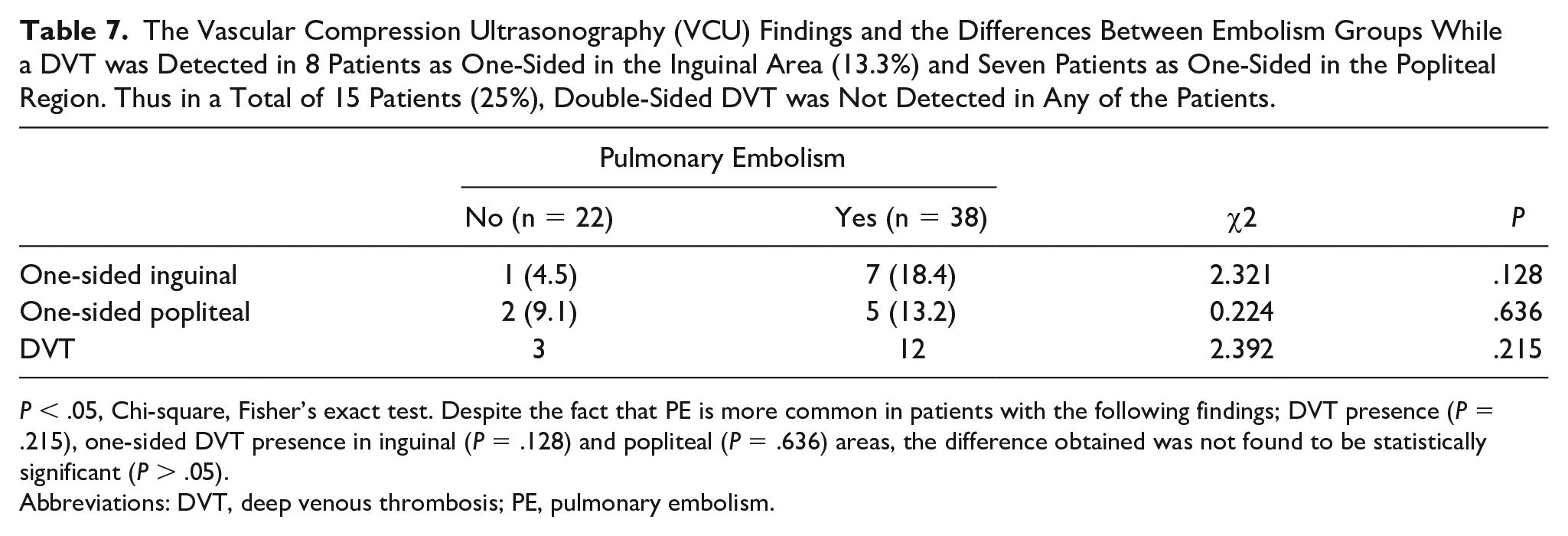
P < .05, Chi-square, Fisher’s exact test. Despite the fact that PE is more common in patients with the following findings; DVT presence (P = .215), one-sided DVT presence in inguinal (P = .128) and popliteal (P = .636) areas, the difference obtained was not found to be statistically significant (P > .05).
Abbreviations: DVT, deep venous thrombosis; PE, pulmonary embolism.
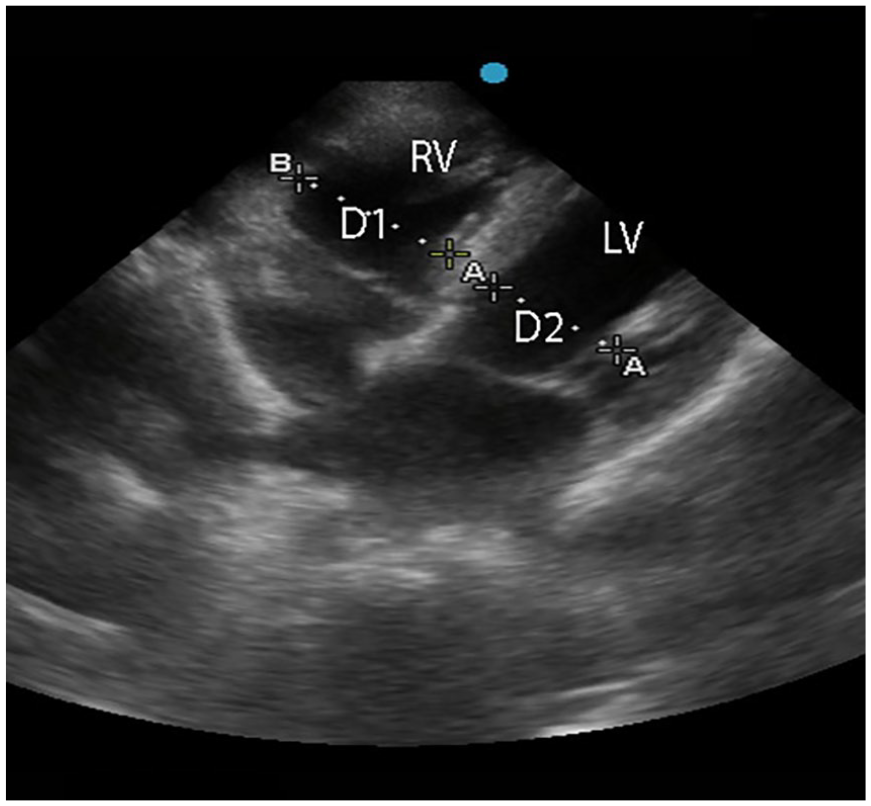
A sonographic apical 4 chamber view of a patient with right ventricular dilatation (D1/D2>1). D, diameter; LV, left ventricle; RV, right ventricle; VCI, vena cava inferior.
In laboratory results, it was found that the higher levels of white blood cells (WBCs), hemoglobin (Hb), hematocrit (Hct), D-dimer, and lower levels of blood urea nitrogen, when compared with patients without embolism were statistically significant (See Table 8).
The Laboratory Diagnostic Findings and the Examination for a Pulmonary Embolism.
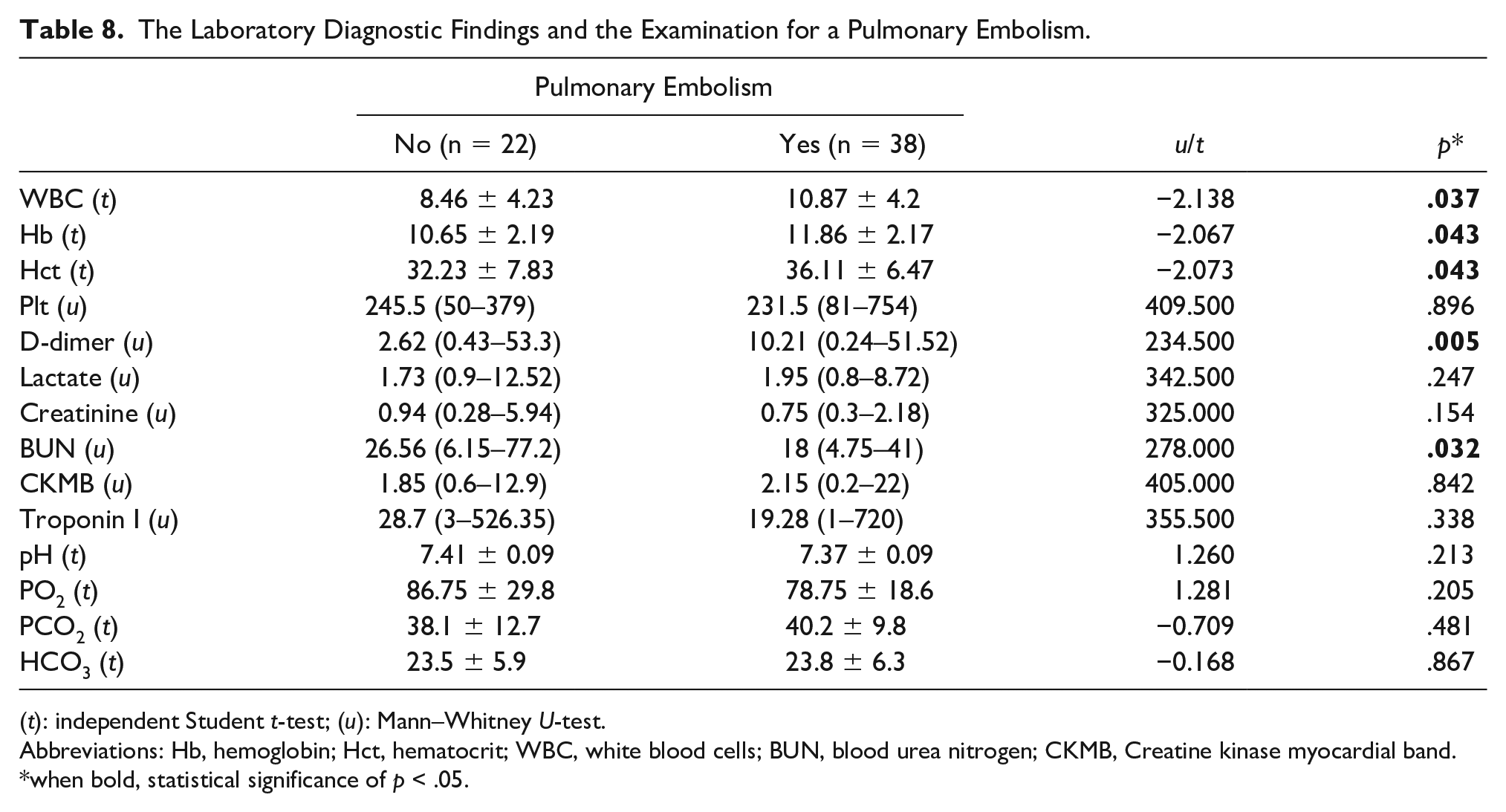
(t): independent Student t-test; (u): Mann–Whitney U-test.
Abbreviations: Hb, hemoglobin; Hct, hematocrit; WBC, white blood cells; BUN, blood urea nitrogen; CKMB, Creatine kinase myocardial band.
when bold, statistical significance of p < .05.
Discussion
A FoCUS performed in emergency medicine department can provide help in making a quick diagnosis or ruling out the following diagnoses: shortness of breath, an acute coronary syndrome, which can be fatal in the differential diagnosis of chest pain, high-risk PE, aortic dissection, and cardiac tamponade. Performing a FoCUS on patients with suspected PE may detect ventricular wall thickness or tricuspid regurgitation; therefore, long-term thromboembolic or pulmonary hypertension should be considered for these patients. 8
The FoCUS imaging protocol can be completed in emergency medicine department and the exam is a part of full echocardiography protocol, even though it is limited in detail. In a study by Dresden et al., 9 they evaluated the correct ventricular width of PE patients with bedside sonography and in 17 out of 146 patients assessed, the left ventricular/right ventricular ratio was found to be greater than 1.0, as well as 15 patients were diagnosed with PE. In that same study, 10 out of 11 patients diagnosed with right ventricular movement flaws were diagnosed with PE. 9 As a result of the study, in PE diagnosis, the sensitivity and specificity of left ventricular/right ventricular were found to be 50% and 98%, respectively. 9
In this study, when CTPA and FOCUS findings were evaluated together, it was detected that in PE patients, right ventricular dilatation, which was deemed the most valuable result, was higher (P < .001). This finding supported published studies conducted with a detail cardiac echogram and a FoCUS study of patients with PE, as well as related sonographic imaging protocols. In the detection of PE in the CTPA examination of patients with right ventricular dilatation, there is a statistically significant relationship. The finding of right ventricular dilatation, in the bedside USG applied to patients admitted to emergency medicine departments, with suspected PE, was statistically significant. In the patients with PE, the frequency of VCI volume, being within the normal interval, was higher than in other sources (P < .05). Pulmonary embolism was detected in 4 out of 5 patients with right ventricular wall motion disorder. Although the incidence of right ventricular wall motion disorder in a FoCUS examination is not common, it is an important finding for the diagnosis of PE.4,5 There are not many published studies, in which the results of a bedside FoCUS examination were performed in an emergency medicine department and with PE patients.
In a study conducted by Atalay et al., 10 in which they examined the value of FOCUS in PE diagnosis, it was detected that in 33 (55.0%) patients out of 60 patients with the final diagnosis of PE, the ratio of right ventricular to left ventricular was less than 0.9 and in 27 patients, the ratio of right ventricular to left ventricular was greater than 0.9. The difference between them was found to be statistically significant. The rise in the ratio of the right ventricle to the left ventricle, right ventricular dilatation, and septal flattening are used interchangeably in the works cited. In the same study, two patients with thrombus at the right ventricular or right atrium were detected. 10
About the Wells score, which is one of the most commonly used risk scoring systems, Bass et al. 11 stated that the sensitivity and specificity of Wells criteria are 72% and 62%, respectively, and reported that its sensitivity goes up to 99%, when used with the D-dimer test. Despite the fact that the Wells score alone or used with the D-dimer test is essential in diagnosis, Hsu and Soo Hoo 12 revealed that physicians’ clinical decision rules, for diagnosing a PE and the rate of using the D-dimer test in conjunction with these rules, varied between 8% and 11.9%, for unknown reasons. Right ventricular dilatation was shown to be statistically significant as a FOCUS finding in patients with intermediate risk according to Wells score and embolism in CTPA assessment (p = 0.003). Although in a 2021 meta-analysis, it was recommended that right ventricular strain, which is one of the findings of a FoCUS, should not be effective in leading clinicians to the diagnosis. 13 This is compared to this study where they considered that the detection of right ventricular dilatation, after the FOCUS, would be performed on the patients with a Wells score of moderate risk and would be efficient for the emergency diagnosis and treatment of PE. 13
Malignancy was determined to be a moderate risk factor in patients diagnosed with PE or deep venous thrombosis (DVT) based on the studies of Rogers et al. 14 and Williams and Goldstein 15 which analyzed more than 16 000 patients, and Anderson and Spencer 16 ; moreover, in the study by Stein et al. 17 patients with PE were shown to have a prevalence of 19% malignancy (excluding lung cancer) and 3% lung cancer. The data from this study support these rates. In addition, in patients with respiratory system diseases such as asthma and COPD who were monitored in this study, the incidence of PE was found to be lower and statistically significant (P = .011) compared to patients with systematic diseases. This finding might suggest that symptoms such as respiratory discomfort and palpitations in patients with long-term respiratory system disease may be predominantly caused by their existing disease and may be helpful for minimizing unnecessary examinations of patients for PE.
When the available data were reviewed, DVT was detected in 12 out of 38 patients (31.57%). In a study by Turksta et al., 18 they examined the DVT findings of 397 patients with suspected PE, using VCU. In that study, 29% of the patients had a DVT detected through VCU. In a more recent study conducted by Perrier et al., 19 this rate was found to be approximately 50%. Although the presence ratio of one-sided DVT in the inguinal (P = .128) and popliteal (P = .636) areas in the patients with PE was high, it was not considered to be statistically significant.
In the study by Çavuş et al., 20 the WBC value was shown to be significantly elevated, consistent with this study findings. In a retrospective research of 1612 patients conducted by Williams and Goldstein, 15 it was discovered that the Hb, Hct, and platelet counts of patients with PE identified in the ED were low. In this study, Hb and Hct increases (P = .043) were statistically significant in patients with PE when it is compared to patients without PE. However, platelet count was not statistically significant in the diagnosis of PE.
In this study, the D-dimer level was shown to be elevated in all, but one patient diagnosed with PE. Plus, it was found that the D-dimer level was statistically significant when compared to patients without a diagnosis of PE (P = .005). Owing to its high sensitivity but low specificity, the generally accepted vision test has been advised to rule out the diagnosis of PE in numerous studies, including the PE 2019 ESC Guide. 6 Nonetheless, it is recognized that the specificity of the D-dimer test increases with clinical scoring systems, and it is advised that the two be interpreted together.
Despite the fact that FoCUS findings in the emergency medicine department contributed significantly to the diagnosis of PE, research indicates that lung sonography findings applied, using the Basic Lung Ultrasound Examination (BLUE) protocol, in patients with acute respiratory failure can also provide supportive data. The posterolateral alveolar and/or pleural syndrome (PLAPS), which is indicative of lung base consolidation, should be further analyzed. If consolidation cannot be detected, veins in the lower extremities should be examined for PE as the only remaining meaningful diagnosis. According to reports, 70% of patients with PE have a DVT, and 30% of these patients are asymptomatic. 21 Patients with suspected PE should have a comprehensive cardiac assessment. It is possible to observe right ventricular dilatation as the McConnell sign or cardiac thrombus. This method may enhance the diagnostic precision of the Basic Lung Ultrasound Examination (BLUE) protocol for detecting a PE.
In recent years, the blood lactate level has been investigated as a biomarker of oxygen transport to tissues in the study of the progression of a variety of disorders. In this study, there was no statistically significant difference even though the serum lactate levels of patients with and without PE were high.
Limitations
This study has the limitations of the research design; therefore, the results cannot be generalized due to internal and external validity constraints. This cohort of participants also represents a convenient sample, which makes these results specific only to this group of participants.
Conclusion
In this study, the FoCUS results, which were gathered in the emergency medicine department, to effectively diagnose a PE, suggests that it was a guide in making the diagnosis. It was discovered that patients with right ventricular dilatation, which was a FoCUS finding, had a significant prevalence of PE. The diagnosis of PE was also shown to be greater in these patients with right ventricular dilatation, as part of the FOCUS result, in patients with intermediate risk, based on their Wells score. Therefore, this would suggest a result that could be replicated and possibly improve the connection between Wells score and the D-dimer test. In this cohort, a high WBC, Hb, and Hct levels were found to be significant in diagnosing PE. A FoCUS examination, which is to be performed by an emergency medicine physician trained in USG, could be very helpful in the diagnosis of PE.
Footnotes
Ethics Approval
This study was approved by the noninvasive Clinical Research Ethics Committee of Faculty of Medicine, Çukurova University (no: 68, meeting: 85).
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.