
Abstract
Pulmonary embolism, a serious complication after trauma, may cause sudden death. We discuss an unusual case of 65-year-old woman who had traffic accident with liver injury and open fracture of both tibia and fibula on the right side. She was diagnosed with massive pulmonary embolism on the second day after accident and successfully underwent emergency surgical embolectomy from bilateral pulmonary arteries. There were no postoperative complications. The patient’s good state of health was recorded after 13 months of surgery. Surgical pulmonary embolectomy for such a multi-trauma patient provides valuable experience not only for our institution but also for the countries having similar resource-limited conditions.
Introduction
Pulmonary embolism (PE) is one of potentially life-threatening complications in the post-traumatic patients with an incidence of 5%–63%. 1 The in-hospital mortality rate was 8.1% for hemodynamically stable patients, 25% for those presenting with cardiogenic shock, and 65% for those requiring cardiopulmonary resuscitation. 2 From the analysis of previous medical literature, the patient had clinical symptoms when pulmonary arteries (PA) were blocked more than 30%–50%. 3 The resistance of the pulmonary artery increases in the patient with PE, causing right ventricle failure. The mechanism of sudden death is mainly due to the electromechanical dissociation. In the milder cases, the patients often experience symptoms including syncope, hypotension, and shock. For the patients who survive an acute PE, the sympathetic nervous system is activated, the endogenous and exogenous mechanisms are stimulated, and the Frank–Starling mechanism working to increase pulmonary arterial pressure and to increase blood flow through the lungs, along with vasospasm mechanism, which may maintain a stable blood pressure for these cases.
The second hemodynamic instability usually occurs after 24–48 h due to the recurrent PE and/or right ventricle failure, which is often because of not found or ineffective treatment for PE, pulmonary re-embolism, and the reduction of compensatory mechanisms. 4 Here, we discuss an unusual case of 65-year-old woman with multi-trauma who had submassive PE and underwent successful emergency surgical embolectomy from bilateral PA.
Case
A 65-year-old woman had traffic accident with liver trauma and open fracture of both tibia and fibula on the right side (Figure 1(a)). She had no problem with the health before. After the immobilization of lower extremity, the patient was admitted to the Department of Emergency Abdominal Surgery for liver conservative therapy. The liver sonography and computed tomography (CT) saw laceration with 11 cm in length, 4 cm parenchymal depth, and parenchymal contusion in IV, V, VI lower lobes without active bleeding (Figure 1(b)). She was diagnosed with third degree of liver trauma according to the American Association for Surgery of Trauma, 5 therefore anticoagulation was delayed for 72 h after admission due to the liver injury.
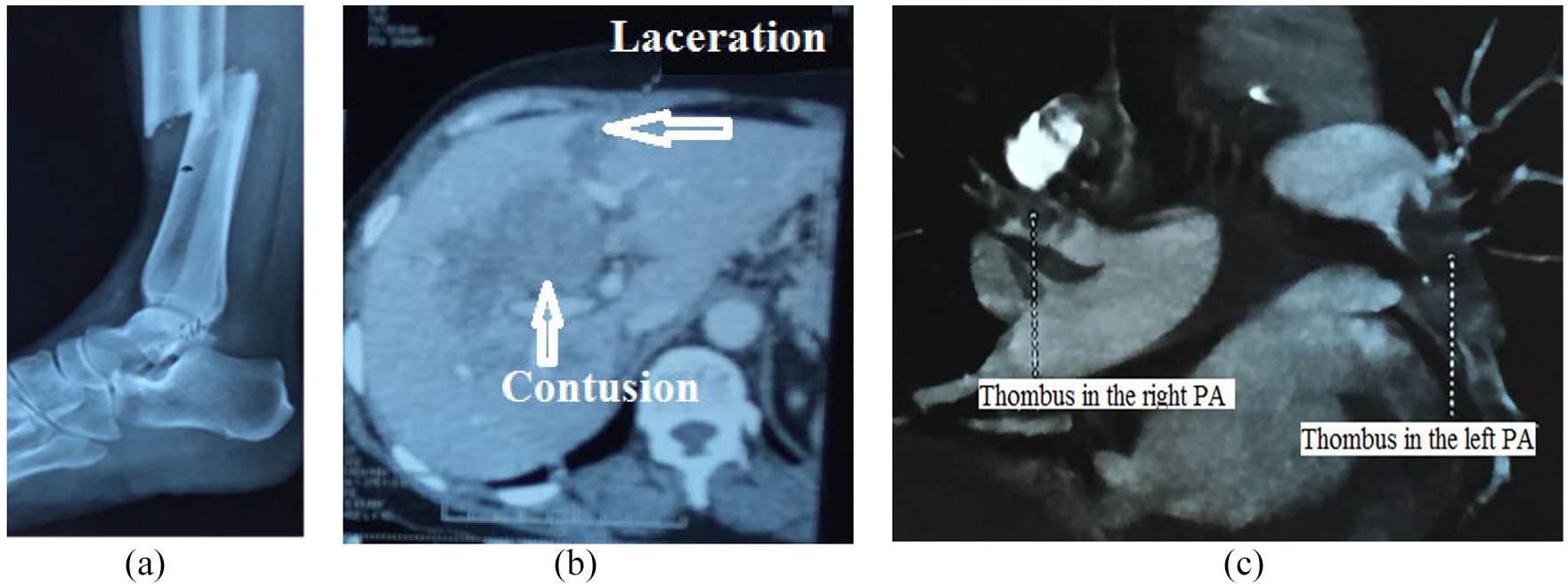
(a) X-ray: the rupture of tibia and fibula. (b) Abdominal CT: liver trauma. (c) Chest CT pulmonary angiography: thrombus in PA.
On her second hospital day, the patient had shortness of breath, chest pain, sinus tachycardia more than 140 per minute, blood pressure 90/60 mmHg and hypoxemic, and oxygen saturation about 90% with high-flow oxygen face mask. An urgent chest CT pulmonary angiography revealed massive PE and pleural effusion (Figure 1(c)).
The patient was immediately sent to the intensive care unit (ICU). An urgent bedside transthoracic echocardiography showed severe right ventricular (RV) dilation, moderate-to-severe pulmonary hypertension, and moderate tricuspid valve regurgitation. Doppler echography showed thrombus of right popliteal and tibial veins. D-dimer analysis was 36940. A team including cardiologists, cardiac surgeons, and reanimatologist consulted together for the consideration of therapies. Because the patient had liver injury, the fibrinolytic therapy was contraindicated; hence, the surgical pulmonary embolectomy was recommended.
The urgency operation was indicated for our patient. In the operation, we used median sternotomy, heparinization by 200 UI/kg, activated clotting time (ACT) about 300–400 s, and aortic and bicaval cannulation. Cardiopulmonary bypass (CPB) went on with full flow and on beating heart the pulmonary trunk was opened longitudinally, extended to left pulmonary artery. Under direct vision, blood clots in left pulmonary artery were taken out by Miniry (special instrument for bile-stone removal) (Figure 2(a)) and left PA purified by warm solution of NaCl 0.9%. In the right side, PA was longitudinally opened next to the superior vena cava, and blood clots were removed using the same method. Mini-incision in right atrium was made to control the absence of thrombus. All incisions were closed by continuous Prolene 5–0 suture. The CPB was stopped and the operation was ended. Bypass time was 30 min.

(a) Pathological specimen from surgical pulmonary embolectomy. (b) CT pulmonary angiography of pulmonary artery after surgery.
The patient was transferred to ICU with low dopamine dose in the stable hemodynamic parameters. Bedside echography of liver showed the same lesion of liver as before, and no change of abdominal effusion. Chest X-ray demonstrated pulmonary interstitial edema. Both her legs were dressed with compression stockings, and heparin was indicated after 6 h of surgery. The patient was extubated successfully within 72 h, and then osteosynthesis was performed after 10 days. After the 7-day osteosynthesis, she was discharged from the hospital with oral Xarelto 20 mg per day. Post-operative CT pulmonary angiography revealed good result, PA without thrombus, and good deflated lungs (Figure 2(b)). A transthoracic echocardiogram showed normal pulmonary pressure and low tricuspid valve regurgitation.
Discussion
The risk factors for the formation of deep venous thrombosis and the cause of pulmonary artery embolism were described in the European Guideline for the Diagnosis and Management of Acute Pulmonary Embolism 6 and the Guideline of American College of Cardiology for Acute Management of Pulmonary Embolism. 7 Our patient had leg fracture and liver trauma, which were considered as two main risk factors in this case. Liver contusion in hemodynamically stable patients was mostly treated conservatively,8,9 and, because of the risk of bleeding, the patient had delayed chemical anticoagulation for 72 h and waited control abdominal CT scan. Mechanical methods for venous thromboprophylaxis are highly recommended (Grade 1A) for patients at high risk for bleeding. 10 In our patient, a graduated compression stocking was used on the non-injured leg only. Pain and edema precluded its use on the fractured side. These two main causes generated deep venous thrombosis, affirmed by Doppler ultrasound.
The diagnosis of PE in this patient was confirmed in the immediate CT-PA. The outcome of PE treatment greatly depends on the patient’s clinical condition. To help choose the appropriate treatment strategy, PE was classified into three groups according to the American Heart Association: massive PE, submassive PE, and less PE. 11 Based on this guide, our patient classified as massive PE.
Treatments of massive PE through recommendation are thrombolysis, catheter embolectomy, and surgical embolectomy.6,7,12 Thrombolysis was contraindicated for this patient because of liver trauma and high risk of bleeding. 13 Catheter embolectomy was not available in our center at this time and the method was chosen to be surgical embolectomy.7,12,14,15
Surgical thrombectomy using CPB is a chosen method when the patient is contraindicated with thrombolytic agents, especially for the patients with right atrial thromboembolism or opposing embolism. Previous studies showed a mortality rate of 20%–30% after surgical thrombectomy; 16 however, to date, with the advancement of cardiac surgery, this figure significantly decreased (4.0%). 17
Our patient was indicated for the surgical embolectomy with CPB. From the analysis of previous medical literature, we found that many techniques were reported for pulmonary artery embolectomy, but the latest announcements were more about pulmonary artery embolectomy on beating heart under CPB. This technique, with low complication and mortality rate, was applied to our patient.1,14,18–20 She had liver injury, so the usage of heparin high doses in surgery was considered with high risk of bleeding. We used the dose of 200 UI/kg of body weight 21 and then tried ACT to maintain an ACT of >480 s during CPB, 22 and probed instead of using the dose of 300 UI/kg of body weight like regular open heart surgery to prevent high ACT and high risk of bleeding from liver contusion.
Implantation of the inferior vena cava filter was also discussed. Ultrasound after surgery showed only thrombus in popliteal vein or lower, and liver injury was stable. The patient could be treated with low-molecular-weight heparin and then with Xarelto. Compression stockings were used as the treatment of deep vein thrombosis, so inferior vena cava filter placement was kept.
Conclusion
In conclusion, PE was a life-threatening disease with high death rates. For massive and submassive PE, urgent surgical pulmonary embolectomy on beating heart with CPB should be proposed as a safe method with good results, especially in cases where thrombolytic therapy is contraindicated and catheter embolectomy is not available.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for her anonymized information to be published in this article.