
Abstract
Objective:
Non-ST-elevation acute coronary syndrome (NSTE-ACS) is a heterogeneous disorder including subgroups with a low or high risk for myocardial ischemia. The presence of postsystolic index (PSI) is associated with myocardial ischemia. The focus of this study was to find probable association between PSI and severity of coronary artery disease (CAD) in a cohort of patients.
Materials and Methods:
This was a cross-sectional study that consisted of 83 patients with unstable angina, non-ST-segment myocardial infarction (UA/NSTEMI), and a left ventricular ejection fraction ≥50%, without visible regional wall motion abnormalities. All patients underwent echocardiography, and global longitudinal strain (GLS), PSI, and mitral annular peak systolic (s′) and early diastolic (e′) velocities were measured. Coronary angiography was then performed, and a SYNTAX score was calculated.
Results:
The patient cohort was divided into two groups based on their high and low SYNTAX scores. PSI and GLS were higher in those patients with a higher SYNTAX score than in individuals with a lower score (85.04% ± 67.02% vs 46.67 ± 39.03, P = .001 and −16.09 ± 3.70 vs −17.99 ± 2.87, P = .012, respectively). Among the different variables assessed, only PSI was an independent predictor of a high SYNTAX score (B = 1.014, 95% confidence interval [CI]: 1.001–1.027, P = .034).
Conclusion:
This cohort study demonstrated that a cumulative PSI may be predictive of much more complex and extensive CAD, especially in patients with UA/NSTEMI.
Non-ST-elevation acute coronary syndrome (NSTE-ACS) is a heterogeneous disorder including different patient subgroups, with a low or high risk of disease severity or mortality. Identifying patients at high risk for poor outcome and mortality is critical. It is due to this fact that these patients should be considered for an invasive strategy to reduce the risk of complications. 1 Speckle-tracking echocardiography (STE) is an inexpensive and easily accessible noninvasive tool that can be used to detect small myocardial injury and determine territories of ischemic myocardium. 2 Longitudinal strain (LS) analysis can provide information on postsystolic strain (PSS), which is characterized as a delayed myocardial shortening that occurs following aortic valve closure. PSS is calculated as the absolute difference between peak global LS and peak systolic LS. 3 The presence of PSS has been reported as an important sign of regional myocardial ischemia, which is more accurate than other advanced echocardiographic variables, such as peak systolic longitudinal strain. 4 Postsystolic index (PSI) is a grading index for determining the severity of myocardial PSS and is defined as: 100 × [(peak global longitudinal strain − peak systolic longitudinal strain)/(peak global longitudinal strain)]. 5 Some studies have shown that a PSI of more than 0% is presented in nearly 80% of healthy individuals. Also, the normal values of measures of PSS are reported as follows: the median averaged PSI (defined as the average value of 17 myocardial segments) of 2.0% (interquartile range: 0.7–4.8) and the median PSS of 0.4% (interquartile range: 0.2–0.8). 3
Conversely, the SYNTAX score is an angiographic scoring system that evaluates the extent, complexity, and severity of coronary artery disease (CAD). Previous studies have been shown that a higher score is associated with a more complex lesion and an adverse prognosis. 6 The aim of this study was to determine whether there is any correlation between PSI and SYNTAX score in patients with unstable angina and non-ST-segment myocardial infarction (UA/NSTEMI).
Materials and Methods
This cross-sectional cohort study was performed on 83 consecutive patients with UA/NSTEMI and a left ventricular ejection fraction (LVEF) ≥50% who were admitted to the emergency department of the hospital between 2020 and 2021. This study was conducted based on the guidelines of the Declaration of Helsinki and was approved by the ethics committee of the host institution. All patients participating in this study signed an informed consent. Acute coronary syndrome (ACS) was diagnosed according to the 2014 American Heart Association (AHA)/American College of Cardiology (ACC) Guidelines for NSTE-ACS. 7 Those patients who presented with symptoms suggestive of ACS, including transient ST changes (≥0.5 mm) or marked T-wave inversion during angina symptoms, consented to the study. Also, patients with symptoms suggestive of ischemia but without ST-T changes were included. The diagnosis of NSTEMI was based on the presence of angina pain and a transient rise in cardiac troponin I (TnI) levels, above the upper normal limits (0.04 ng/mL). Blood samples for determining cardiac enzyme levels were taken within 10 minutes of presentation and measurements were repeated every 4 to 6 hours, during the first 2 days. Unstable angina was defined as new or aggravating angina or angina occurring at rest with no elevation in cardiac troponin. 8 Those patients excluded from the study demonstrated persistent ST-segment elevation of 0.1 mV or more in leads other than aVR or V1, left bundle branch block (LBBB), or anterior ST depression representing posterior ST-segment elevation myocardial infarction.
Coronary angiography (CAG) was performed on all the participating patients with a Siemens AG fluoroscopy equipment system (Medical Solutions; Erlangen, Germany). A single experienced cardiologist interpreted the angiograms but only had anonymized patient data. A SYNTAX score was used to evaluate the extent, complexity, and severity of CAD. The patient’s overall SYNTAX score was calculated from summation of these individual scorings for every lesion using an algorithm of SYNTAX score, which is available on the SYNTAX webpage. 9 Based on this data, the patients were divided into two groups, based on either a high (≥22) or low (<22) SYNTAX score. 10
Patients with prior history of CAD, significant valvular heart disease, an LVEF <50%, atrial fibrillation, LBBB, neoplasms, cardiomyopathies, fever, and any systemic illnesses were excluded from the study. In addition, those patients who had regional wall motion abnormality or prior history of coronary revascularization were also excluded. Additional variables considered for this study were hypertension (HTN), which was characterized as a systolic blood pressure ≥140 mmHg and/or a diastolic blood pressure ≥90 mmHg or taking antihypertensive drugs. 11 In addition, diabetes mellitus (DM) was identified in this cohort based on the American Diabetes Association guidelines and also patients who need to take insulin or oral hypoglycemic medications. 12 Hyperlipidemia (HLP) was considered when there was a total cholesterol level >200 mg/dL and high-density lipoprotein cholesterol level <40 mg/dL in males or <50 mg/dL in females. 13 To calculate body mass index (BMI) in this cohort, an individual’s weight in kilograms was divided by their square of height in meters. Glomerular filtration rate (GFR) was determined by this formula (15% less in females): GFR = (140 − age) × (weight in kg)/72 × serum Cr (mg/dL) × 0.85 if female. 14
Echocardiography
All patients underwent a transthoracic echocardiography using an ACUSON SC2000 ultrasound equipment system equipped with a 4V1c transducer (Siemens Medical Solutions USA Inc., Mountain View, CA), 48 hours after hospitalization. The two-dimensional (2D) grayscale cine clips were obtained in three standard apical views. These included the apical four-chamber, two-chamber, and three-chamber views. In this cohort, the peak LS values from the basal, mid, and apical segments of the inferoseptal, anterolateral, inferior, anterior, inferolateral, and anteroseptal myocardial segments were obtained by the tracing of the endocardial and epicardial borders (eSie VVI software). The measurements were performed using a software dedicated for semi-automated analysis. The average value of all 18 myocardial segments was considered as the peak global longitudinal strain (GLS). 15 PSS was considered as the myocardial shortening which occurs after the end of systole. PSI was obtained from 18 myocardial segments and was calculated as (maximum strain − peak systolic strain/maximum strain) × 100 (%) (see Figure 1). If the time to maximum strain of a segment curve was before the end systole, it was considered PSI of this segment to be zero. 5 Sum of the PSI value obtained from 18 myocardial segments was considered as the total PSI value (the values were added together). The left atrial (LA) diameter was described as the vertical end-systolic distance between the posterior LA wall and the posterior aortic root in the parasternal long-axis view. 16 The apical four-chamber view was used to determine the transmitral Doppler early diastolic velocity (E-wave) and the E-wave deceleration time (DT) by placing cursor at the mitral valve leaflet tip. Average tissue Doppler mitral annulus septal and lateral early diastolic velocities (e′) were acquired by placing the cursor at the level of the mitral annulus. M-mode echocardiography was used to determine end-systolic and end-diastolic left ventricular (LV) internal dimensions and end-diastolic interventricular septal (IVS) and posterior wall thicknesses which were obtained at the level of LV minor axis by inserting the cursor at the mitral valve leaflet tip in parasternal long-axis view. The LV mass was calculated as follows: 0.8 (1.05 [(LVIDD + posterior wall thickness diameter (PWTD) + interventricular septal wall thickness diameter (IVSTD) 3 − (LVIDD) 3 ]) + 0.6 which end-diastolic LV internal diameter (LVIDD), posterior wall thickness (PWT), and interventricular septal wall thickness (SWT), are representative of the end-diastolic LV internal diameter and posterior and IVS wall thickness diameters, respectively. 15 M-mode echocardiography, in the parasternal long-axis view, was used to determine the diameter of the ascending aorta by placing the cursor 3–4 cm above the aortic valve. 17 The maximum opposing wall dyssynchrony was described as the maximum difference in time-to-peak strain in the opposing myocardial walls of three apical views including four-chamber, two-chamber, and three-chamber views. 18 The time-to-peak longitudinal strain was considered as the overall time-to-peak strain of these aforementioned three apical views.
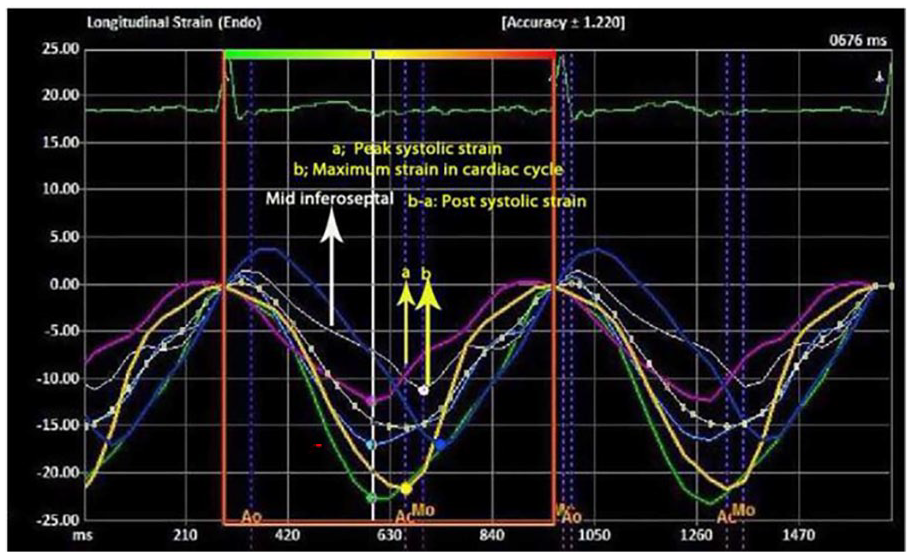
Longitudinal speckle-tracking echocardiography in apical four-chamber view shows strain curves in inferoseptal and anterolateral LV myocardial walls which are divided into three segments including basal, mid, and apical segments. Strain curves demonstrating PSS are displayed on each wall segment. The PSI is computed as (maximum negative strain in cardiac cycle − peak negative systolic strain)/(maximum negative strain in cardiac cycle) × 100. The yellow vertical arrows indicate a peak negative systolic strain and maximum negative strain in cardiac cycle and in mid inferoseptal myocardial segment. LV, left ventricular; PSI, postsystolic index; PSS, postsystolic strain.
Statistical Analysis
The continuous variables were described with means and standard deviation, while categorical variables were presented as frequency and percentage. The normality for quantitative variables was determined using the Shapiro–Wilk test and demonstrated a normal distribution for all variables. Therefore, all continuous variables were compared using an independent t test. Conversely, the categorical variables were compared using the chi-square and Fisher’s exact tests. Finally, a logistic regression analysis was conducted to determine the confounding effects of different variables on the SYNTAX score. A P-value of less than .05 was considered to be significant. SPSS/PASW (Predictive Analytics Software) (SPSS, Chicago, IL, USA), version 18, was used to conduct the statistical analysis.
Results
This cohort study included 83 patients and of those, 53 were male and 30 females, with unstable angina or NSTEMI. These patients were admitted to the emergency department of the host hospital. This patient cohort had a mean age of 62.24 ± 9.36 years and a mean BMI of 27.06 ± 4.33 kg/m2. Cardiac troponin levels were elevated in 27 of these patients (32.5%). HTN was the most frequent CAD risk factor (44 patients, 53%) that was followed by DM (36 patients, 43.4%) and HLP (27 patients, 32.5%), in decreasing order of frequency. Table 1 demonstrates the demographic and laboratory features of the two study subgroups. This patient cohort was divided into two groups with high (≥22) and low (<22) SYNTAX scores. The mean age, BMI, serum Cr, GFR, prevalence of DM, and HTN were not statistically significant between the two groups. However, male gender, HLP, and a positive troponin result were more prevalent in patients with a higher SYNTAX score than in those with a lower score.
The Descriptive Information That Was Used to Describe and Compare Demographic and Paraclinical Variables Within the Two Study Subgroups is Characterized by High (≥22) and Low (<22) SYNTAX Scores.
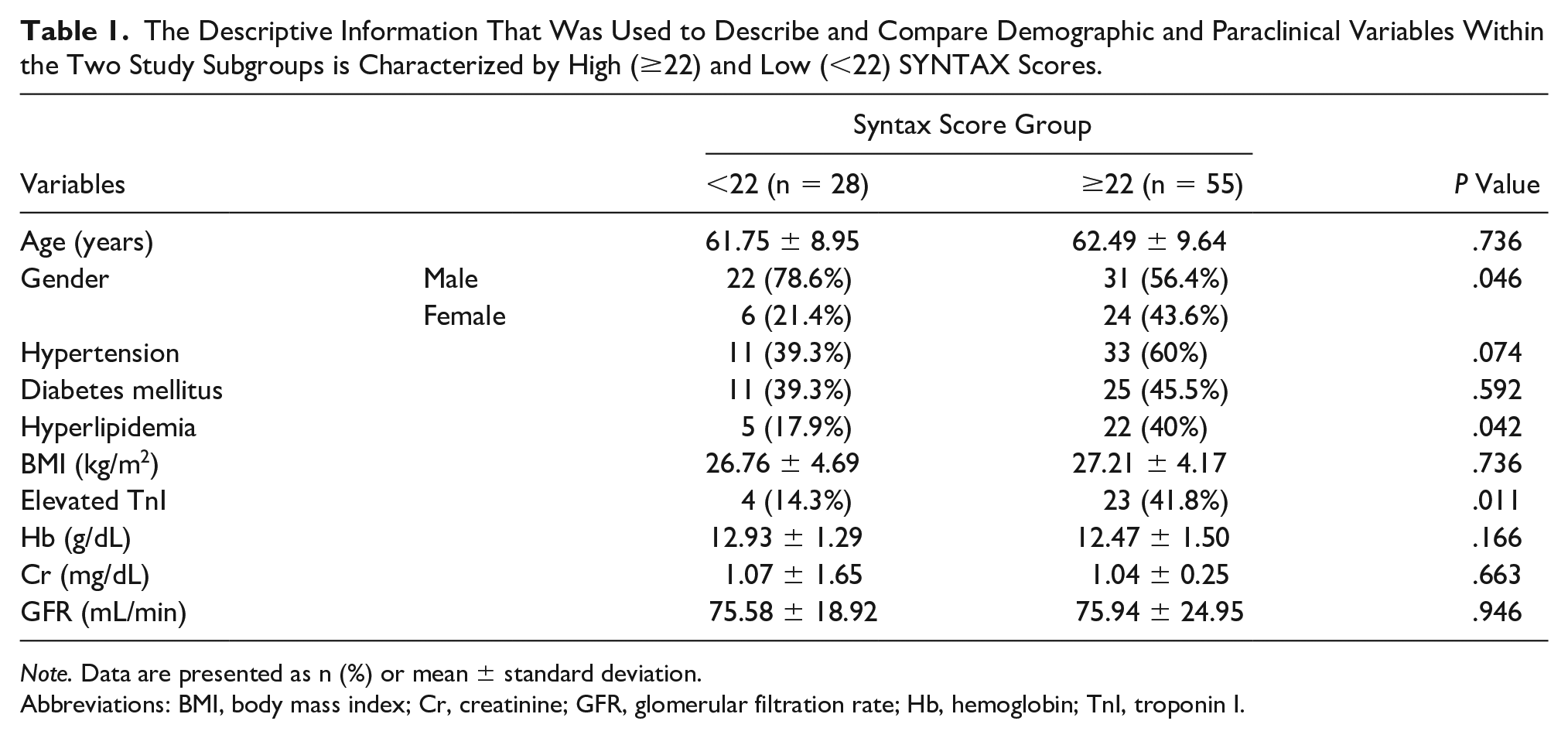
Note. Data are presented as n (%) or mean ± standard deviation.
Abbreviations: BMI, body mass index; Cr, creatinine; GFR, glomerular filtration rate; Hb, hemoglobin; TnI, troponin I.
Among the different echocardiographic variables, PSI and GLS were higher (P = .001 and .012, respectively) in patients with a higher score than in those with a lower SYNTAX score (see Tables 2 and 3, and Figure 2). A logistic regression analysis was performed to determine the independent effects of different demographic and echocardiographic variables, in predicting a SYNTAX score (see Table 4). This analysis revealed that among different demographic and echocardiographic variables, only PSI was an independent predictor of a high SYNTAX score (B = 1.014, 95% confidence interval [CI]: 1.001–1.027, P value = .034). This would mean that for every unit increase in PSI, a probability of having a SYNTAX score ≥22 increased by 1.4%.
The Comparison of Conventional Echocardiographic Variables Based on the Two Study Subgroups is Characterized by High (≥22) and Low (<22) SYNTAX Scores.
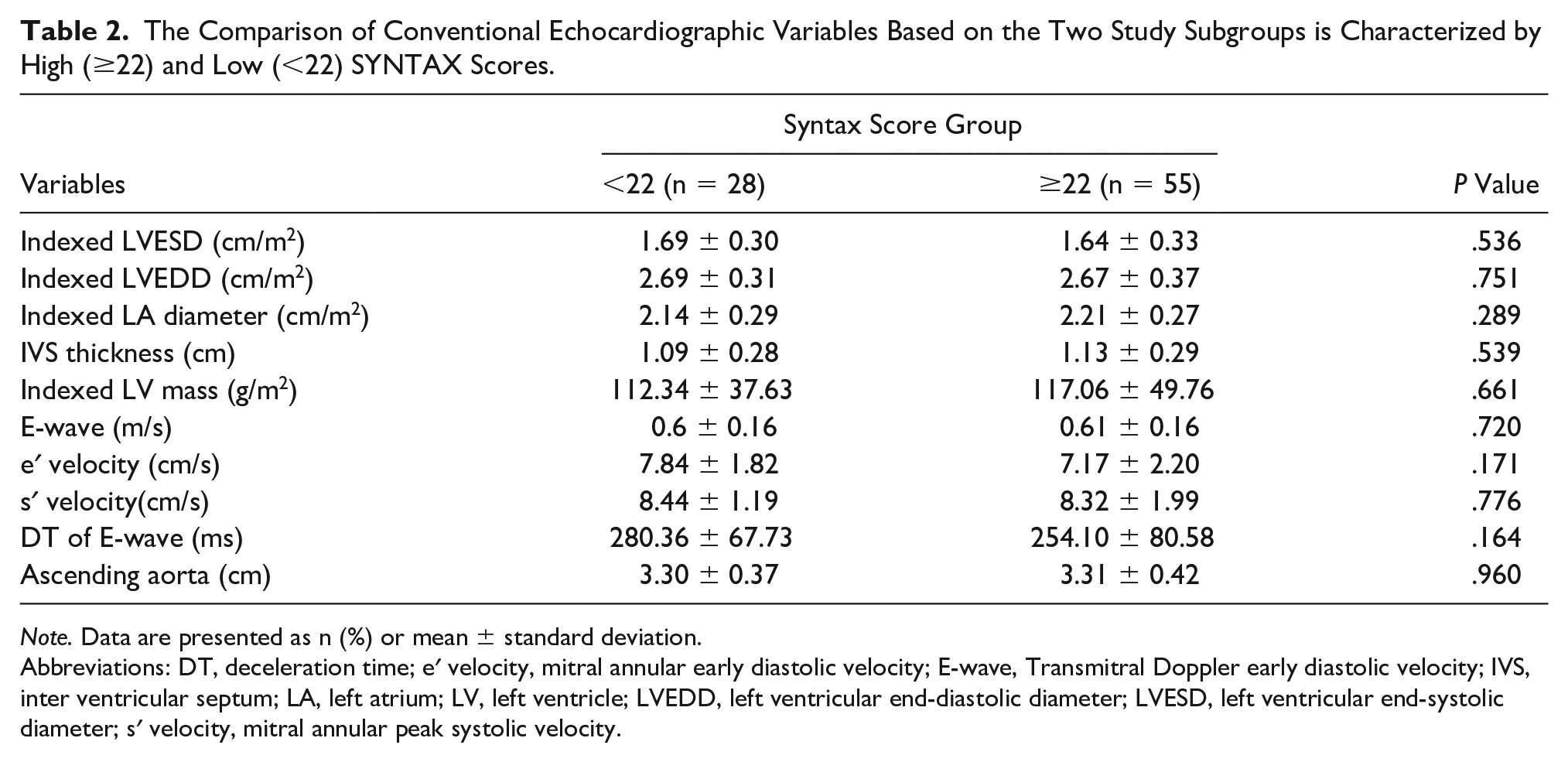
Note. Data are presented as n (%) or mean ± standard deviation.
Abbreviations: DT, deceleration time; e′ velocity, mitral annular early diastolic velocity; E-wave, Transmitral Doppler early diastolic velocity; IVS, inter ventricular septum; LA, left atrium; LV, left ventricle; LVEDD, left ventricular end-diastolic diameter; LVESD, left ventricular end-systolic diameter; s′ velocity, mitral annular peak systolic velocity.
The Comparison of Speckle-Tracking Echocardiographic Variables Based on the Two Study Subgroups Characterized by High (≥22) and Low (<22) SYNTAX Scores.
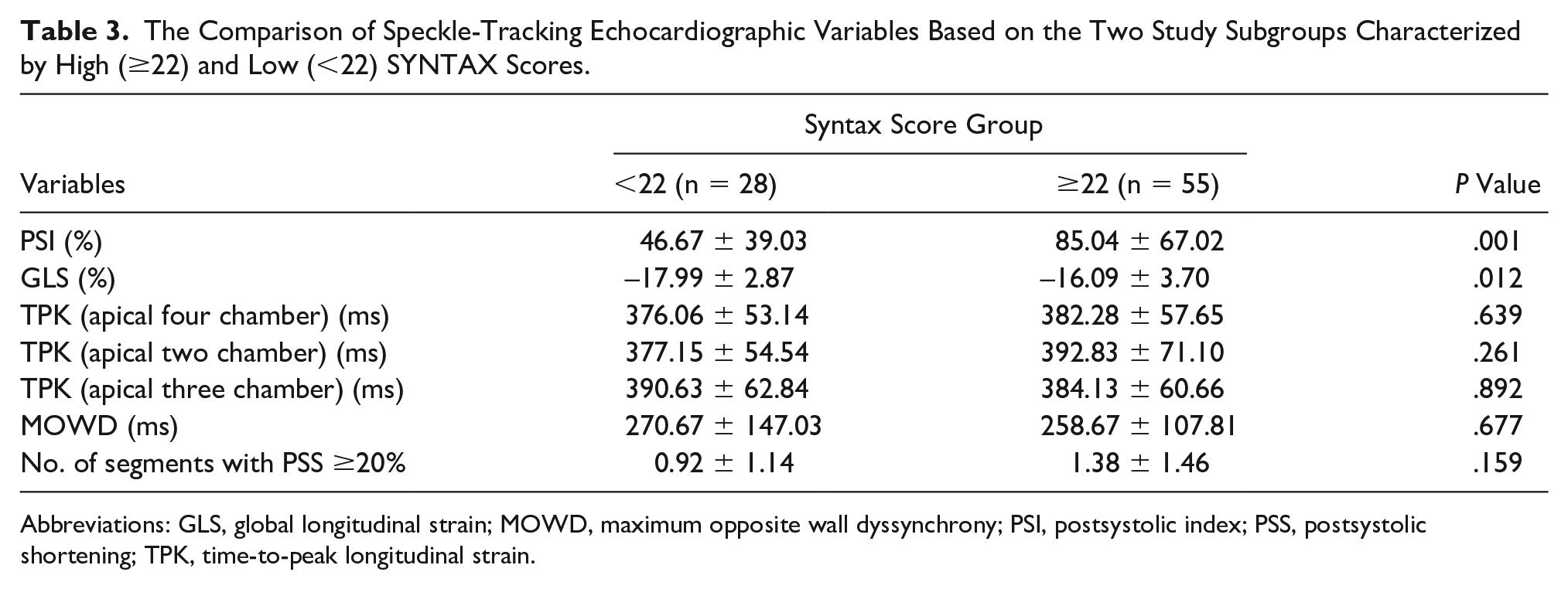
Abbreviations: GLS, global longitudinal strain; MOWD, maximum opposite wall dyssynchrony; PSI, postsystolic index; PSS, postsystolic shortening; TPK, time-to-peak longitudinal strain.
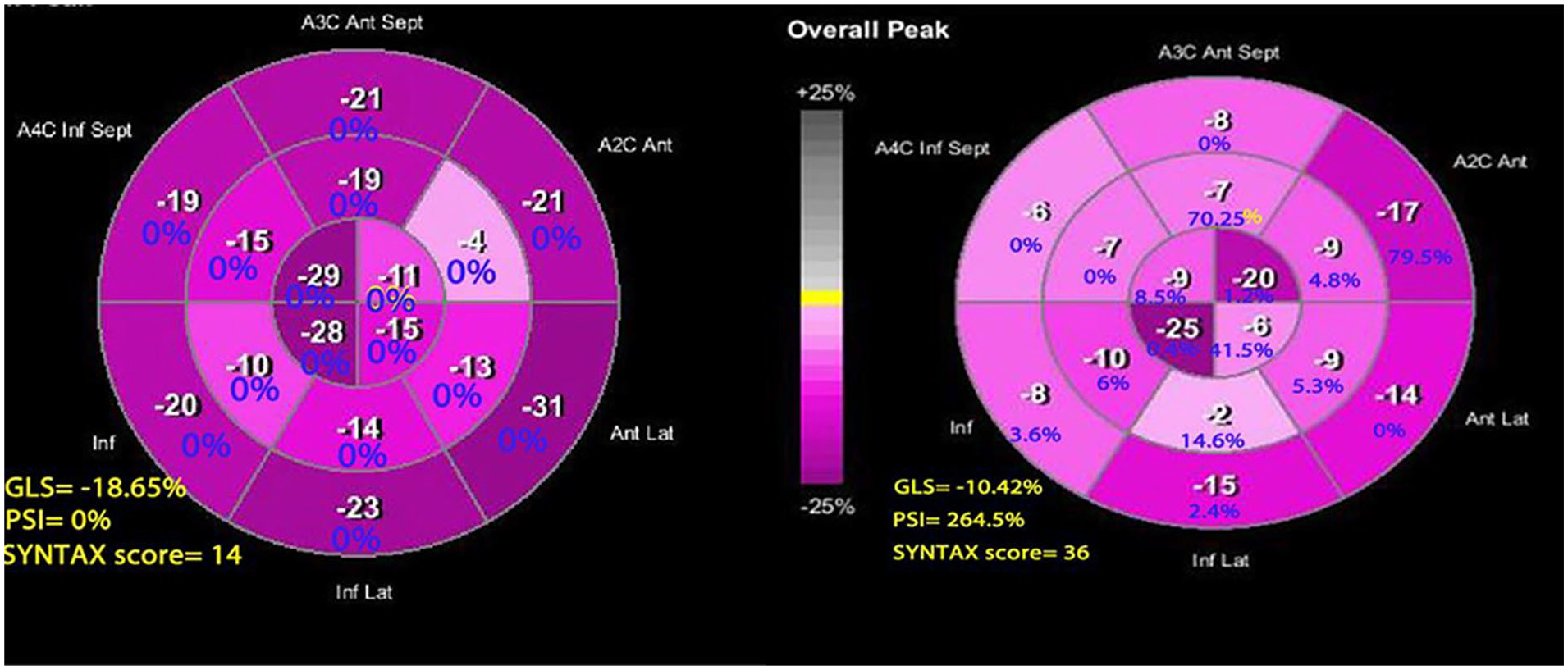
The peak systolic strain (white) and postsystolic shortening (blue) values in the 17 segments of the left ventricle are shown in the bulls-eye plots. A2C, apical two-chamber; A3C, apical three-chamber; A4C, apical four-chamber; Ant, anterior; Ant lat, anterolateral; GLPS, global lateral pulse strain; Inf, inferior; Inf Lat, inferolateral; Inf Sept, inferoseptal; PSI, postsystolic index.
The Results of the Logistic Regression Analysis That Determined a Relationship Between Different Demographic and Echocardiographic Variables Compared to the Angiographic SYNTAX Scores ≥22.
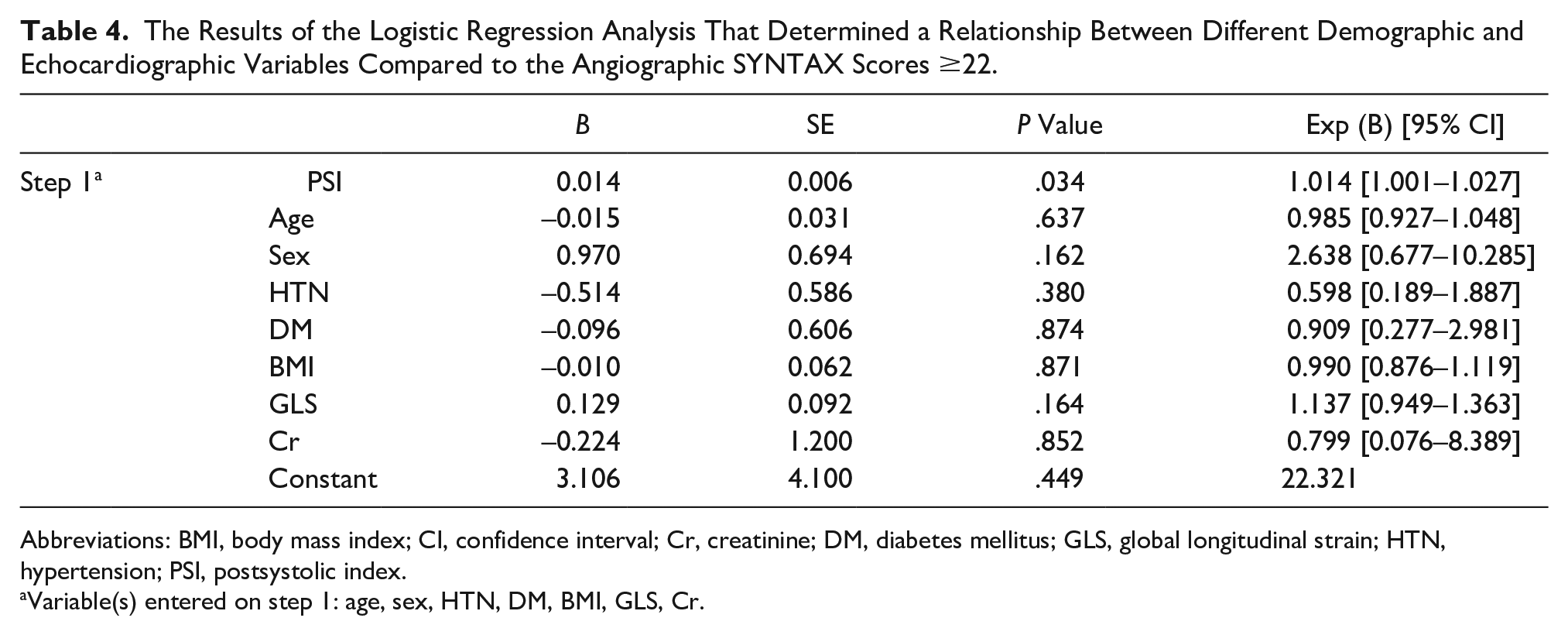
Abbreviations: BMI, body mass index; CI, confidence interval; Cr, creatinine; DM, diabetes mellitus; GLS, global longitudinal strain; HTN, hypertension; PSI, postsystolic index.
Variable(s) entered on step 1: age, sex, HTN, DM, BMI, GLS, Cr.
Discussion
This cohort study showed that UA/NSTEMI patients with a SYNTAX score ≥22 had higher GLS and PSI than those with a score of less than 22. Among different echocardiographic and demographic variables, only PSI was an independent predictor of a high SYNTAX score.
Patients with severe CAD may have a normal left ventricular wall motion at rest. Therefore, finding another resting parameter with an ability to distinguish patients with severe CAD from those with a less severe or no CAD would be helpful. 19 STE is highly valuable for detecting ischemia in patients with suspicion of ischemia in the absence of visual wall motion abnormalities. Indeed, an LV GLS >−18.8% has been reported to have a high sensitivity and specificity in determining coronary artery stenosis in patients with chest pain and non-diagnostic electrocardiogram and blood biomarkers. 2 Also, patients with stable angina have shown concurrent decrease in GLS and increased number of involved coronary vessels and a significant correlation between GLS and LVEF. 20 In the present study, all patients had an LVEF ≥50% without any regional wall motion abnormalities. A high SYNTAX score may be predictive of a more complex and extensive CAD. The current study cohort was divided into two groups based on their SYNTAX score, with the cut-offs utilized in the US/European guidelines, including patients with a low score ≤22, as well as those with intermediate to high scores (>22). 21 In this cohort, a higher value of GLS was found in patients with SYNTAX score ≥22 than those with a score of less than 22. In a study on 216 patients who underwent CAG with a suspicion of CAD, segmental LV LS could localize coronary lesions and was inversely correlated with SYNTAX score. 22 PSS is characterized as myocardial contraction that happens after the end-systole and is detected mostly during isovolumic relaxation. Determination of PSS is important in the diagnosis of acute ischemia. It is due to this fact that this delayed contraction is observed in the setting of regional contractile dysfunction. 23 In 2003, Voigt et al. conducted a study on 20 young control students, 10 older control individuals, 30 patients with acute myocardial infarction, and 10 patients with post myocardial infarction scar. Longitudinal myocardial deformation was determined by Doppler tissue strain rate imaging. They reported that PSS was normally seen in almost one-third of myocardial segments of healthy individuals. However, PSS occurred more frequently in acutely ischemic and scarred myocardium (78% and 79%, respectively). Their findings indicated that pathologic PSS is usually associated with decreased systolic strain. 24 In 2018, Brainin et al. performed a cohort study on 293 patients with suspected stable angina pectoris who underwent STE and CAG. The pathological PSS was defined as PSI ≥20% in each myocardial wall. They described significant CAD as ≥70% stenosis in one or more epicardial coronary arteries. Patients with significant CAD had a higher prevalence of PSS, and the presence of PSS was strongly predictive of significant CAD. During the follow-up period of 3.5 years, the existence of PSS and PSI was independently predictive of the secondary end points including major adverse cardiovascular outcome and revascularization. 23 A SYNTAX score was not included in their study and only ambulatory patients with stable angina pectoris were entered. In the present study, an absolute value of PSI was higher in patients with a high SYNTAX score than individuals with a lower score. Also, the current study patients were admitted with UA/NSTEMI.
In 2020, Rumbinaite et al. performed a study on 83 patients with a moderate probability of having stable CAD and an LVEF ≥55%. CAD was defined as ≥50% diameter stenosis on CAG. The results of this study showed that regional PSI assessment during recovery phase of dobutamine stress echocardiography can improve the diagnostic accuracy of this modality for detecting significant CAD. However, PSS parameters did not differ significantly among CAD and non-CAD groups during the rest. 25 Contrary to the present study, their patients were ambulatory individuals without any evidence of acute ischemia. The mitral valve annular motion is representative of overall longitudinal LV contraction and relaxation, which is displayed by s′ and e′ velocities, respectively. Reduction of e′ velocity is a marker of impaired LV relaxation or increased LV filling pressure. Conversely, a decrease in s′ velocity is seen during episodes of myocardial ischemia that is indicative of regional contractile dysfunction. However, there are some significant limitations in the capability of s′ velocity in predicting abnormal regional function. 26 The SYNTAX score is an angiographic system for evaluation of the grade and complexity of coronary artery lesions. A higher SYNTAX score is representative of a more complex lesion and a poor prognosis in patients undergoing coronary revascularization. 6
Limitation
The major limitation of this study was the research design and a conveniently small sample size. Also, patients’ outcome and mortality were not included in the study. Because this research was a cross-sectional study, echocardiographic variables were compared between patients with low and high SYNTAX scores.
Conclusion
This cohort study showed that a cumulative PSI in 18 myocardial segments can be predictive of much more complex and extensive CAD in patients with UA/NSTEMI.
Footnotes
Acknowledgements
We would like to thank all patients and our hospital staff for their care and support that enabled us to perform this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by Mazandaran University of Medical Sciences ethical committee (IR.MAZUMS..REC.1398.5921).
Informed Consent
A written informed consent was obtained from all participants.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study.
Trial Registration
not applicable.