
Abstract
Tissue Doppler imaging, left ventricular color M-mode velocity propagation, and deformation imaging techniques from the medical literature were critically reviewed. The review was undertaken to evaluate the accuracy, reproducibility, and clinical efficiency of echocardiographic technologies for image acquisition and data analysis in assessing pediatric diastolic function. Tissue Doppler imaging, velocity propagation, and deformation imaging all show low variability and high reproducibility and specificity. Age, growth, heart rate, morphology, and sonographic technique affect some pediatric echocardiographic indices more than others; therefore, each should not be solely relied on. Their complementary diagnostic information should be evaluated collectively as a complete echocardiographic examination by expertly trained medical professionals.
Keywords
Diastology is a multifaceted approach for evaluating myocardial relaxation of the ventricles and an important component of a complete echocardiographic examination. As individuals age, ventricular relaxation declines, resulting in myocardial stiffness, elevated pressures, and eventual heart failure. In very young children and adolescents, diastolic abnormalities can indicate subclinical cardiovascular degeneration in patients without congenital heart disease. The degree of diastolic dysfunction determines future prognosis, with choices ranging from therapeutic approaches to surgical intervention and palliation.
A complete assessment of diastolic function includes pulsed wave Doppler evaluation of isovolumic relaxation, early ventricular filling, diastasis, late ventricular filling, and left atrial size calculations. Currently, the standard for performing pediatric echocardiograms include the aforementioned diastolic parameters, which are obtained primarily from mitral valve and pulmonary vein inflow. As diastolic function is further studied and better understood, newer modalities are more routinely employed clinically for assessing diastolic dysfunction, three of which are the focus in this literature review: tissue Doppler imaging (TDI), color M-mode left ventricle velocity propagation (Vp), and deformation imaging.1-19 Collectively, these quantify ventricular compliance and filling patterns. Sonographers and practitioners must exhibit the expert knowledge and skills necessary to perform the proper image acquisition, properly utilize correlating data analysis software, and understand how to interpret the data with the given limitations to accurately assess and differentiate diastolic dysfunction in children.
Transmitral and Pulmonary Inflow
While not the topic of comparison in this literature review, the role of mitral valve and pulmonary vein inflow properties is included at this point because of their relevance to diastolic mechanics and recognition of dysfunction.20-28 From an apical four-chamber view, a pulsed wave Doppler sample volume is placed at the level of the mitral valve leaflet tips, and a spectral Doppler tracing is obtained whereby early (E wave) and late (A wave) diastolic peak velocities are measured and recorded. From this spectral tracing, the deceleration time is calculated from peak E to baseline, and the A wave duration is measured. Angling the transducer slightly anterior produces the apical five-chamber view, from which a continuous wave Doppler cursor can be aligned between the left ventricular outflow tract and the anterior mitral leaflet, obtaining a tracing that allows the isovolumic relaxation time to be measured and recorded.
While in the apical four-chamber view, a pulsed wave Doppler sample volume is placed approximately 1 cm proximal to the right upper pulmonary vein orifice as it enters the left atrium, and a spectral tracing is obtained such that peak systolic and diastolic velocities are measured, as well as peak A wave reversal velocity. These parameters provide data that are simple and useful in quickly assessing the status of ventricular diastolic dysfunction, but they can be limited in their clinical value because of valvular regurgitation severity, the age and size of the patient, as well as other confounding factors mentioned in the Discussion section.
Diastolic Echocardiographic Modalities and Techniques
Tissue Doppler Imaging
TDI is a Doppler modality used to measure the myocardial velocity as the left ventricle relaxes during diastole. Gain and filter settings are adjusted to maximize detection and display of the low velocities of the myocardium, enabling their separation from the high signal velocities of mitral inflow during this phase. In an apical four-chamber view, peak myocardial velocities are measured with pulsed wave Doppler during early (E′) and late (A′) diastolic filling at the septal and lateral walls of the left ventricle near the mitral annulus, with an interception angle no greater than 20 degrees from the lateral wall 1 (Figure 1). Variations in sample gate placement have been noted, ranging from multiple myocardial segments throughout the left ventricle in initial studies to the medial and lateral mitral annulus, while other studies included annular velocities from the right ventricular free wall. Measurements were typically averaged over 3 to 6 cardiac cycles, depending on the study, and velocities were found to be angle and load dependent.2-7
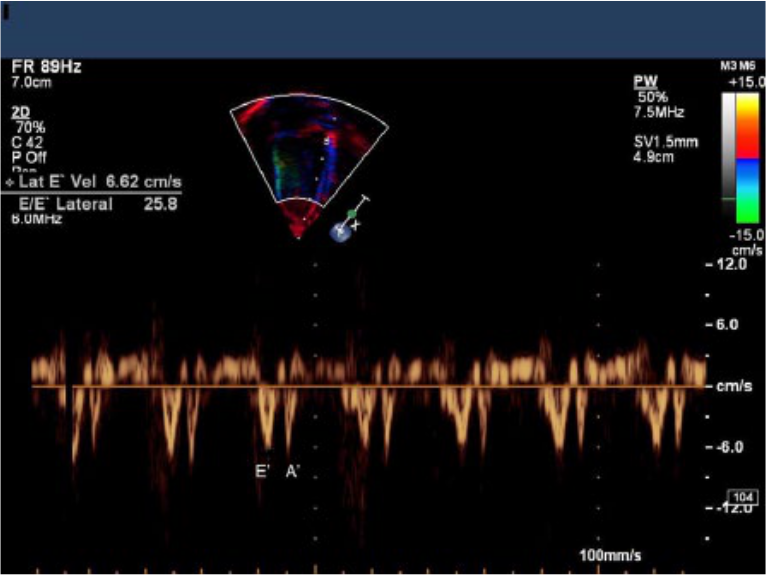
Pulsed wave Doppler waveform depicting myocardial tissue velocity at the mitral annulus during early (E’) and late (A’) diastolic filling. (Reprinted with permission from Border WL et al: Color M-mode and Doppler tissue evaluation of diastolic function in children: simultaneous correlation with invasive indices.
Several studies showed a higher variability of myocardial velocities in neonates and children <1 year, with heart rate having a slightly greater effect on late diastolic velocities and minimal to no effect on early diastolic velocities, while age and cardiac size exhibited the largest impact. This variability decreased substantially after the first year and was closely correlated with left ventricular end diastolic dimensions.3,4,6,8 TDI reproducibility remained relatively high; mean absolute variances of velocity measurements ranged from 2.2% for interobserver variability to 5.5% for intraobserver variability. 4 While TDI reproducibility is high, a study of 325 children (63 of which were neonates) published in 2004 by Eidem et al. determined that previous studies have significant shortcomings in terms of sample size and consistent methods of obtaining values. 4 The Eidem et al. study showed causality between age and increased TDI velocities and was the first to evaluate these relationships in children <1 year old. A smaller study in 2000 consisting of 48 children was performed by Harada et al. 6 and showed similar correlations, as did a study consisting of 131 children performed by Mori et al., also in 2000. 8 Roberson et al.—whose 2007 study consisted of 634 children, 276 of which were <1 year of age—concluded that TDI was a clinically effective and highly reproducible method to assess left ventricular diastolic function in children. 3 As reported by Berg and Greve in 2013, TDI produces reliable results 9 ; unlike endocardial tracings used to measure ejection fraction, TDI does not rely on cardiac geometry and thus is a useful technology for patients with cardiomyopathies.
Color M-mode Vp
Within the past two decades, color M-mode left ventricle Vp has been developed and used to assess ventricular relaxation by measuring the velocity of blood as it enters and fills the left ventricle throughout diastole. Originally described in 1992 by Brun et al., 10 from the apical four-chamber view, an M-mode scan line is placed through the left ventricle from the apex to the mitral valve, parallel with the direction of blood flow. The color scale is adjusted to alias during early diastolic filling (E). The aliasing slope of the E wave occurring at early diastolic filling is measured to determine Vp, which gives an accurate representation of the entire ventricle during relaxation (Figure 2). Unlike mitral valve inflow, which can pseudonormalize as diastolic dysfunction progresses, this modality does not exhibit any such changes. 2 Additionally, Vp assesses left ventricular spatiotemporal filling patterns simultaneously and is acquired in one image, as compared with multiple pulsed wave velocities, which are obtained separately at different depths along one scan line; it is also load independent.11,12 In 2003, Border et al. studied 20 patients and determined an interobserver variability rate of 11.4%, and although the variability was slightly higher than that found with TDI, it was comparable in its diagnostic utility. 2 Additionally, the study concluded that the ratio of E/Vp was 100% sensitive, with 77% specificity, in seven patients who had elevated end diastolic pressure (>15 mm Hg). Because this modality provides accuracy in velocity of relaxation patterns throughout the ventricle in one image, several studies concluded that it was an effective parameter and recommended that it be used in pediatric examination protocols.2,11,12
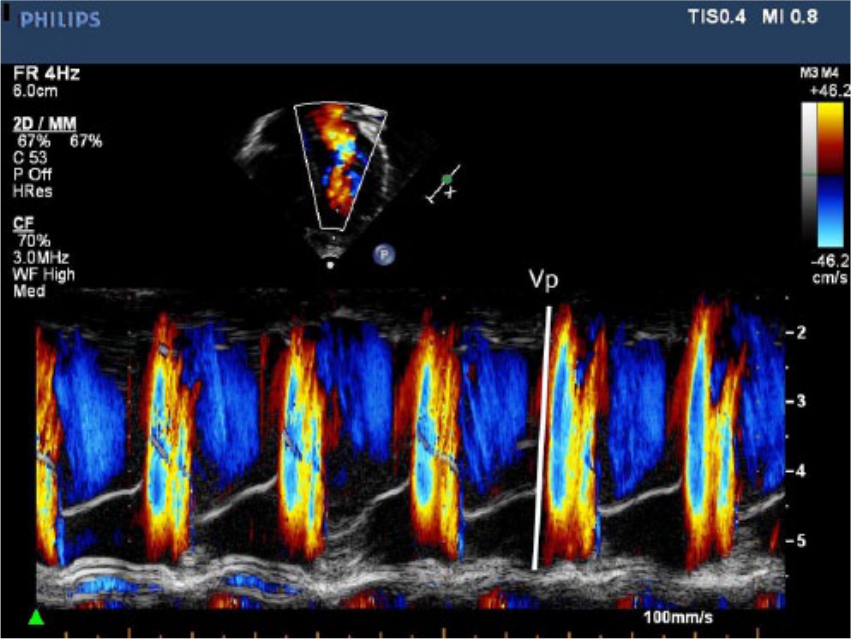
Left ventricle color M-mode velocity propagation (Vp) image. The aliasing slope captured during early diastole is representative of filling velocity through the left ventricle and illustrated here by the white line where the color change is at its brightest. (Reprinted with permission from Border WL et al: Color M-mode and Doppler tissue evaluation of diastolic function in children: simultaneous correlation with invasive indices.
Deformation Imaging: Speckle Tracking, Strain, and Strain Rate
Deformation, or myocardial fiber strain, is a complex modality originally described in 1973 by Mirsky and Parmley, as reported by Heimdal et al. 13 It was preliminarily used in 1994 for magnetic resonance imaging before being recognized shortly thereafter as an effective diagnostic echocardiographic tool.14,15 Deformation imaging measures the spatiotemporal twisting of the myocardium in three dimensions (longitudinal, radial, and circumferential) from its original relaxed state (strain). Two types of strain describe the 3D deformation of the left ventricle: normal strain, which comprises longitudinal, circumferential, and radial strain, and sheer strain, which is composed of circumferential-longitudinal, circumferential-radial, and longitudinal-radial. 16 These motions rotate the apical portions of the left ventricle clockwise while rotating the base counterclockwise and shortening the ventricle length from base toward the apex. It is this deformation that is measured with speckle tracking, from which strain and strain rate are derived. 5
Deformation analysis utilizes Doppler-derived technology to measure velocities of a myocardial segment as the ventricle changes shape during twisting and untwisting between active and passive phases over the course of one cardiac cycle. 17 The velocity of the untwisting occurs during isovolumic relaxation, which precedes early diastolic filling and is used as a parameter to measure diastolic function. 5 From any of the traditional apical views, specialized software systems allow the transducer to identify evenly spaced natural acoustic markers, or “speckle” within the myocardium, and track their movement with very high resolution over one cardiac cycle, measuring the myocardial velocity (strain rate) frame to frame during postprocessing17,18 (Figure 3). Singh et al. reported one of the early studies using speckle tracking in 2010 that included 22 children with normal cardiac anatomy and 15 with congenital heart defects and that assessed 16 ventricular segmental measurements, which were averaged and analyzed to conclude overall function. 14
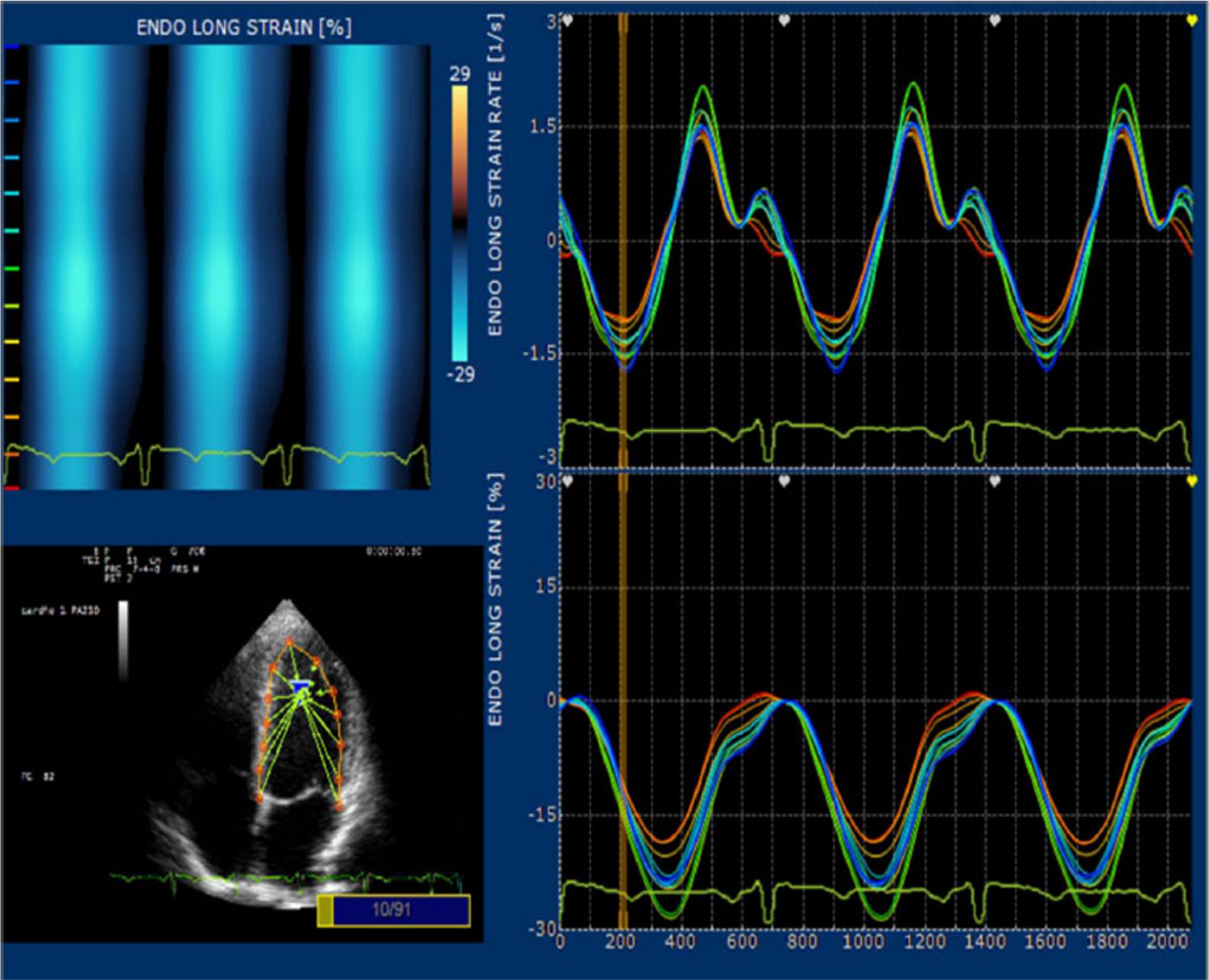
Selected points within the left ventricle are color coded and tracked to illustrate deformation and evaluate longitudinal strain and strain rate of the myocardium. (Reprint permission via Open Access article distributed under the terms of the Creative Commons Attribution License from Bussadori C et al: A new 2D-based method for myocardial velocity strain and strain rate quantification in a normal adult and paediatric population: assessment of reference values. Cardiovasc Ultrasound 2009;7:8.)
Several studies determined that the frame rate for accurate speckle tracking imaging be kept between 50 and 90 frames per second with a temporal resolution >100 Hz to avoid undersampling because of the higher heart rates of children.14,16,17 Geyer et al. reported that subendocardial segments produce higher values of sheer strain and are the predominant force behind ventricular function. 16 This segment is also more susceptible to disease, showing earlier signs of dysfunction than myocardium and epicardium, both of which may overcompensate to maintain function. These segments can be detected easily through speckle tracking.
Dandel et al. reported deformation imaging to be very sensitive and variability relatively low, ranging from 3.6% to 11.8% between intra- and interobserver findings for strain and strain rate measurements. 17 A 3-year study of 2888 patients in 2013 by Cheng et al. reported very low variation in speckle-tracking based measurements, ranging from <4% to <9%. 18 According to several deformation imaging studies, speckle tracking has shown higher sensitivity to preclinical ventricular dysfunction than traditional TDI and has a low rate of variability and a high rate of reproducibility.14,16-19 Several studies concluded that deformation imaging is an important component of echocardiographic examinations in detecting heart failure subclinically before myocardial dysfunction becomes symptomatic and that it also provides accurate prognostic data, particularly after surgical intervention; thus, it is recommended as part of regular echocardiographic examinations.5,16,17
Discussion
The recognition of diastolic dysfunction is increasingly used as an indicator of myocardial health, a precursor to a disease state, heart failure, and mortality.20,21,22 The stages of abnormal diastolic dysfunction are classified as mild, moderate, and severe, as determined by the combined published parameters referenced in this literature review, inclusive of limiting factors and variables defined and as reported in prior published studies. Understanding the relevance and progression of diastolic dysfunction has become a useful tool in developing treatment plans, and its severity can be a strong indicator of increased risk of hospitalization, prolonged hospital stays, and an increased risk of death.20,23 Its usefulness as a determinant for prognosis is notable in patients with dilated cardiomyopathy, noncompaction cardiomyopathy, hypertrophic cardiomyopathy, amyloidosis and other restrictive diseases of the myocardium, single ventricle morphology, postoperative Fontan, and other repair procedures, as well as in patients with aortic stenosis, renal failure, transplantation, hypertension, and coronary artery disease.24-30
Additionally, left ventricular diastolic dysfunction is shown to be greatly impaired after surgical correction of significant congenital heart diseases, such as those mentioned above.21,25 To date, the number of studies and data correlating the effect of congenital heart disease on diastolic function are limited and consistently reported as needing further research.24,25,29
Similarly, the importance of performing diastolic dysfunction parameters on the right ventricle has been suggested, but studies are limited and not yet validated.24,25,31,32 As with the left ventricle, there is no gold standard in diastolic dysfunction parameters for pediatric patients 25 ; however, it has been recommended that right ventricular diastolic dysfunction be more closely studied, as the processes leading to heart failure progress similarly in both ventricles. 31 An example given in a study published in 2011 by Morris et al. found that of patients who exhibited left ventricular diastolic dysfunction in the setting of heart failure with a normal ejection fraction, 48% to 75% also had right ventricular diastolic dysfunction, as calculated with strain rate methodology. 31 In the setting of cardiomyopathies most affecting the right ventricle, such as tetralogy of Fallot, assessing right ventricular diastolic dysfunction is important to identify these at their onset, as prognosis is poor once diastolic dysfunction becomes apparent.9,33
Currently, there is no consensus on standardized quantitative values used for the pediatric population in grading diastolic dysfunction. Numerous studies published offer a wide range of values for each parameter of diastolic assessment and provide insight to understanding the limitations that practitioners and expertly trained medical professionals must consider when referencing these values to grade diastolic dysfunction. These include the effects of heart rate, age, body surface area, conduction abnormalities, and valvular regurgitation, among other factors. * Likewise in adults, criteria by which diastolic dysfunction is graded leave a significant amount of room for interpretation. 20
Further confounding the standardization of pediatric diastolic dysfunction values and parameters are the effects of sedation used during pediatric echocardiograms. While studies documenting the effects are scarce, a study by Vinch et al. in 2004 concluded that conscious sedation lowered mitral E velocities, myocardial wall stress, and the pressure gradient between the right ventricle and atrium. 40 As a result of these variations and an attempt to better classify diastolic dysfunction in children, a study published in 2013 by Dragulescu et al. set the value of each parameter as abnormal if >2 SDs for age groups in published references. 25
Mortality rates in children with diastolic dysfunction are not well documented, and data are lacking 20 ; however, an observational study by Sankar et al. in 2014 of 56 children suffering from fluid refractory septic shock stated the mortality rate as 43% in those who had diastolic dysfunction. 41 For comparison, adult mortality rates are similar to those of patients with systolic heart failure. 21 Diastolic dysfunction that worsens is indicative of poorer outcomes along with higher rates of morbidity and all-cause mortality with diastolic heart failure.28,42 Prognostic studies by Nagueh et al. in 2009 used diastolic Doppler parameters, and the data compiled provided insight into prognosis and mortality rates for the Doppler parameters measured in adults. 36 A study by Halley et al. in 2011 of 36,261 adult patients reported that the mortality rate increased as the severity of diastolic dysfunction worsened: 21%, 24%, and 39% exhibiting mild, moderate, and severe diastolic dysfunction, respectively. 43
Treatment options also are not well defined in the pediatric population for diastolic dysfunction. Studies of treatments in the adult population have proven difficult, as the primary clinical focus has been on improving systolic function in the setting of heart failure rather than on treating diastolic dysfunction.44-46
Because of the morphologic differences of ventricular geometry and orientation in very young patients, neonates, and those with cardiomyopathies, it can often be difficult to accurately assess myocardial health using the standard TDI and the pulsed wave Doppler imaging modalities described previously. As a result, non-Doppler-derived speckle tracking, strain, and strain rate imaging has recently developed. The effect of age and cardiac growth on quantitative values, as well as inconsistencies among institutions in data analysis and software, particularly for the newer modalities, has been reported in several studies.3-5,17,21 A higher variability of myocardial velocities in neonates and children <1 year old was consistently reported. Cardiac growth, rather than heart rate, was credited as having the greatest impact on myocardial velocity.4,22 This variability decreased substantially after the first year and was found to be closely correlated with left ventricular end diastole dimensions and size. 4 A study in 2008 by Lorch et al. found that maturational changes had a very low impact on deformation indices but should be compared against normalized z scores, 39 and a study published in 2004 by Schmitz et al. evaluating 234 neonates determined that this diastolic maturation process is complete by 3 months of age. 7
These inconsistencies and the difficult nature of pediatric echocardiography motivated medical professionals to develop standardized criteria to aide in diagnoses. In 2010,the American Society of Echocardiography published recommendations for performing a pediatric echocardiogram. 47 In addition, nomograms and z scores based on body surface area have been published, but reports concluded that further, more extensive studies with a higher number of participants are required before these values are proposed for standardization.3-5,21,23
Conclusion
Diagnosing diastolic function in pediatric patients has proved challenging for medical professionals due to cardiac size, morphologic and maturational changes, heart rate, sonographic techniques, and variability in technologies and data analysis. TDI, Vp, and deformation imaging all offer highly accurate, reproducible, comparable, and complementary data, but their application requires expert knowledge and experience in image acquisition and interpretation of results. Each of these echocardiographic imaging technologies provides beneficial diagnostic criteria for evaluating diastolic function in pediatric patients and exhibits a unique set of limitations. Vp offers high rates of sensitivity and specificity in analyzing diastolic function and is load independent, and ventricular function can be assessed in one image. TDI provides high spatiotemporal resolution but is angle and load dependent. 39 Deformation imaging has a higher percentage of reproducibility, is dimensionless and angle and load independent, and can be postprocessed offline after completion of patient examinations, but it requires higher frame rates to ensure accuracy, as well as expert readers.1,5,14,17,19,39 Deformation imaging through non-Doppler speckle tracking, strain, and strain rate, though not yet widely practiced in the clinical setting, provides sonographers and physicians with precise diagnostic information and is rapidly gaining support.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.