
Abstract
Objective:
The objective of this study was to quantify the organizational commitment of sonographers and determine factors influencing their connection or bond with their employer.
Materials and Methods:
One thousand nationally credentialed sonographers and vascular technologists in the mid-Atlantic region were surveyed using a systematic sampling model. Measurement tools included the Affective, Continuance, and Normative Commitment Scales. Descriptive and inferential statistics based on stepwise regression were used to define organizational commitment levels and the impact of sociodemographic characteristics on organizational commitment.
Results:
Of the 1000 surveys mailed, 110 usable surveys were returned (11% response rate). Affective, continuance, and normative commitment scores were 4.30, 4.62, and 3.46 out of 7, respectively. Results showed living in Pennsylvania, years at current organization, being a registered cardiac sonographer, and being unmarried had a statistically significant impact upon the variance in sonographers’ organizational commitment scores.
Conclusion:
Sonographers indicated feeling little obligation to remain with the employer but may do so because of the perceived costs of leaving. As a result, sonographers’ performance, work behavior, and attendance may be affected negatively. Factors such as locale, marital status, work tenure, and registration as a cardiac sonographer impact sonographers’ organizational commitment.
Keywords
Key Takeaways
Knowledge of employees’ organizational commitment and its individual components can help employers create programs and policies that promote employee retention, job satisfaction, and positive work behaviors.
The study’s sample of sonographers was not emotionally attached to the organization for which they worked, which can potentially lead to behaviors such as absenteeism and turnover.
The study’s sample of sonographers did not feel obligated to work for their current employer, which can be influenced by socialization experiences as new employees and by investments an organization makes in their employee.
Living in Pennsylvania influenced all three of the components of organizational commitment (i.e., affective, normative, and continuance). Further exploration of sonography practice in Pennsylvania may be worthwhile.
Organizational commitment refers to the mindset reflecting a desire, need, or obligation to maintain membership in an organization. Some employees remain with an organization because of an emotional attachment to the organization. Employees with this emotional attachment typically have a good attendance record, better job performance, and organizational citizenship behavior, crucial to their organization’s success. 1 Examples of organizational citizenship behavior include working as a team and decision making based on the organization’s best interest. Emotionally attached employees also accept circumstances as they are, exhibit loyalty to the organization, and are more vocal when suggesting improvements. 1 In contrast, employees with commitment to the organization driven more by the costs associated with leaving (e.g., loss of seniority, salary reduction, loss of friendships, or a sense of obligation) tend to possess behaviors different from those with high emotional attachment. 1 Studies have found notable outcomes associated with organizational commitment such as turnover,2–4 work quality, 1 job satisfaction,1,3–6 absenteeism, 7 and burnout.8–11
Organizational commitment has been conceptualized and investigated extensively over the past five decades by various researchers such as Meyer 1 and Allen, 12 Mowday, 13 Porter, 3 and Steers. 5 The model of organizational commitment has evolved from a two-component model (i.e., the employee is either committed or not committed to the organization) to the current three-component model (see Figure 1). Divided into three components, organizational commitment consists of affective, normative, and continuance commitment. Each component comprises leading reasons employees remain with organizations and may be evidenced by different behaviors exhibited by employees who display more of one component over another.
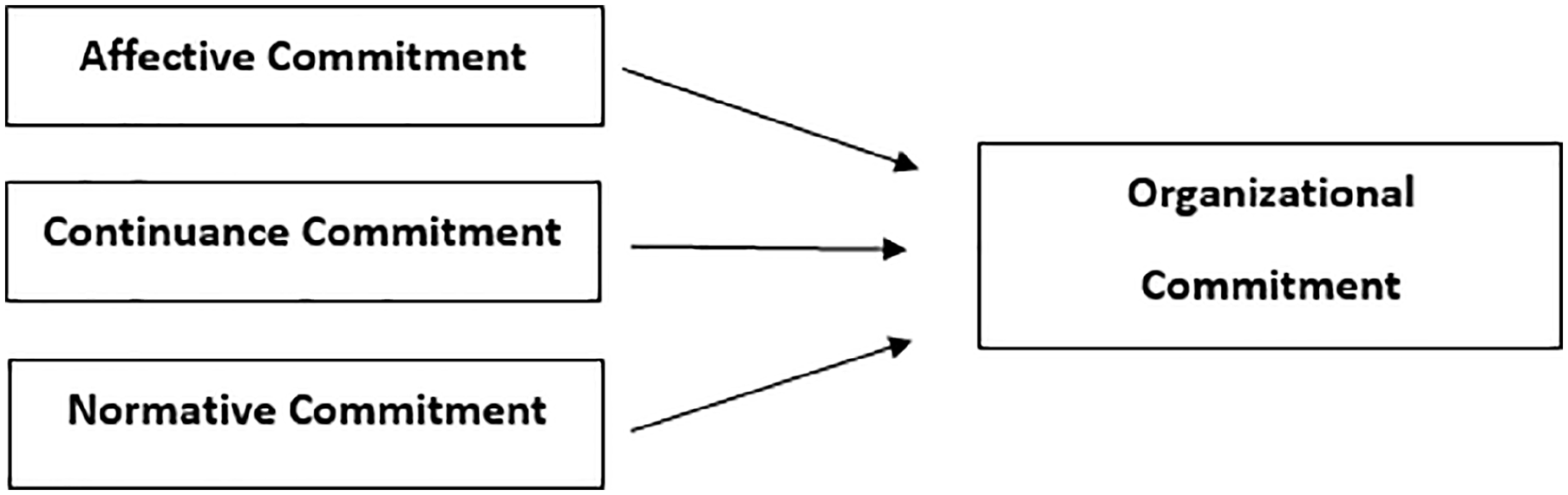
A representation of the three-component model of organizational commitment.
Affective organizational commitment is the emotional attachment held by the employee to remain with their employer; it includes the employee’s sense of fitting in or identifying with the organization’s goals and values. 1 Employees with higher levels of affective commitment are happy with their work-life experience, typically demonstrating good attendance, better job performance, and organizational citizenship behavior crucial to their organization’s success.
In contrast, employees with commitment to the organization driven more by the costs associated with leaving or by their feeling of obligation tend to behave differently than employees with high emotional attachment. This type of commitment, termed continuance commitment, may cause employees to remain with an organization because they feel the need to after calculating the costs of leaving. 1
Normative commitment is based on a sense of obligation and the feeling of a need to stay at the organization that is influenced by experiences both prior to and upon entry into an organization. 1 Examples of these experiences could include onboarding experiences as a new employee, previous salary/raise negotiations, and experience when a family member was a patient. Normative commitment is lower when an employee is unhappy in their organization or wants to pursue other opportunities. 1
Although the three components of commitment presumably increase the likelihood that employees will remain with the employing organization, employees’ motives for remaining, work behaviors, and productivity levels may differ based upon which component they most possess. Organizational commitment is moderated by antecedents (i.e., a thing or event existing before another) such as personal characteristics, job or role-related characteristics, and work experiences. 5
Personal characteristics are factors that define the employee such as age, education, opportunity for achievement, role tension, and central life interest.1,5 Job characteristics consist of the challenge of the job/work, opportunities for social interaction, and the amount of feedback provided by the employer.1,14 Identifying employees’ organizational commitment is necessary for organizations to understand the sustainability of their workforce. It also provides an opportunity to fully evaluate and understand employees’ behaviors, performance, attendance patterns, and interpersonal views toward the organization. Understanding employees’ commitment can help an organization implementor continue processes and policies that provide a competitive advantage, resulting in higher patient satisfaction scores and dedicated employees.
Organizational Commitment in the Health Professions
Among a sample of American Occupational Therapy Association members (n = 237), general working conditions, task involvement, task autonomy, and supervision positively affected the respondents’ organizational commitment to their employer. 15 A qualitative study of staff nurses (n = 30) from a large Los Angeles County university hospital identified themes positively impacting organizational commitment 14 (e.g., opportunities for learning and continued education, monetary benefits, patient care, and job security). Other themes, such as lack of appreciation and lack of job security, potentially decreased employees’ organizational commitment. Overall, these themes align with the antecedents of organizational commitment formulated originally by Steers. 5
No study of organizational commitment of sonographers was identified to date. However, radiographers (n = 119) from Gauteng, South Africa, have been surveyed to determine the extent to which perceived organizational support influenced their organizational commitment. 16 Using items from Meyer and Allen’s organizational commitment scale and other instruments, the authors reported a moderate level of affective and continuance commitment among participants, although normative commitment was considered low. 16
Akroyd et al. 17 focused on the predictive ability of organizational leadership, work role, and demographic variables on the organizational commitment of American Registry of Radiologic Technologists (ARRT)-registered radiographers (N = 456). The model demonstrated that 50% of the observed variance of affective commitment and 40% of normative commitment variance were accounted for by the linear combination of the predictor variables such as organizational support, years as a radiographer, education level, and organization type. For example, participants with certificates or associate degrees reported higher levels of continuance commitment than participants with bachelor’s or master’s degrees. 17
Another study examined the predictive abilities of organizational support, role ambiguity, role conflict, and managerial leadership on the organizational commitment of ARRT-registered radiation therapists (n = 176). 18 Similar to the study of radiographers, 17 results indicated that increased organizational support and high levels of supervisory transformational leadership behaviors were associated with higher levels of affective and normative commitment. However, the model was weak for predicting continuance commitment. 18
The purpose of the present study was to determine the three organizational commitment component scores for sonographers, in the mid-Atlantic region, of the United States and analyze the relationships between each commitment component and certain sociodemographic variables. Because the profession is forecasted to grow 14% from 2020 to 2030 (faster than the average for all occupations), 19 it is imperative that employers identify sonographers’ commitment components to anticipate their behavior, attendance, and teamwork on the job. It will also be important to learn how to manage and keep sonographers at their facility and determine which factors could influence sonographers’ organizational commitment.
Materials and Methods
This quantitative study used a cross-sectional research design to measure sonographers’ three organizational commitment components and identify relationships between each commitment component and sociodemographic variables. Specifically, this study addressed the following research questions:
The institutional review board of Virginia Commonwealth University classified the research as exempt from ethics approval and informed consent according to 45 CFR 46 since this research only included interactions involving tests, surveys, or interview procedures, or observations of public behavior when identifiable information is recorded by the investigators. The study was also supported by the ARDMS.
Study Population and Sample Frame
The mailing list of ARDMS registrants was managed by Infocus Marketing, Inc., which provided a list of ARDMS-registered sonographers (i.e., diagnostic medical sonographers [RDMS], diagnostic cardiac sonographers [RDCS], and vascular technologists [RVT]) residing in the mid-Atlantic region of the United States (i.e., Delaware, District of Columbia, Maryland, Pennsylvania, Virginia, and West Virginia). The ARDMS required all mailings to include the following disclaimer on each mail piece using the ARDMS mailing list: “This product (service) is not affiliated with or endorsed by Inteleos™. ARDMS® and APCA™ are part of the Inteleos™ family of certification councils.”
The estimated sample size was calculated by using an a priori sample size calculator for multiple regression. 20 An estimated sample of 156 respondents was necessary based on the following parameters: α = 0.05, desired power = 0.80, medium effect size = 0.15 and 20 predictors. To account for potential low response rates to the mailed survey, 20% was added to the desired sample size, resulting in a desired sample size of n = 187. One thousand nationally credentialed sonographers and vascular technologists in the Mid-Atlantic region of the United States were surveyed on sociodemographic and professional data using a systematic sampling model. Measurement tools included the Affective, Continuance, and Normative Commitment Scales. Descriptive statistics and inference based on stepwise regression were used to define organizational commitment levels and the impact of sociodemographic and professional characteristics on organizational commitment. To further encourage participation, a second survey packet was mailed to all non-respondents eight weeks later.
Instrumentation
This study used the Affective Commitment Scale (ACS), Continuance Commitment Scale (CCS), and Normative Commitment Scale (NCS). The ACS consists of eight items and uses a 7-point Likert scale response format of strongly disagree to strongly agree. Median internal reliability is reported as 0.85. 1 The ACS evaluates the employee’s emotional attachment to and identification with the organization. The CCS assesses the extent to which employees feel committed to their organization after considering the costs associated with leaving and consists of nine items measured by the same 7-point Likert scale. 21 Median internal reliability for this measure is reported as 0.79 1 and is not correlated with the ACS. 21 Last, the NCS was employed to assess commitment based on a sense of obligation to the organization. 12 Consisting of six items using the same Likert scale as the ACS and CCS, this measure’s median internal reliability is 0.73. 1
For all three scales, factor analysis indicates that all three forms of organizational commitment are distinguishable constructs and different from instruments measuring other concepts such as job satisfaction, career commitment, occupational commitment, and perceived organizational support. 1 Authors of the three-component model of organizational commitment suggest not assigning high, medium, or low values to the commitment component scores. 1
Study Variables
The affective, normative, and continuance commitment scores were calculated using the published methodology. 1 The organizational commitment scales were reported as a mean based on the 7-point Likert-type scale with a range from 1 (strongly disagree) to 7 (strongly agree). The following sociodemographic variables were included: age (years), race/ethnicity, birth gender, state of residence, and marital status. Professional characteristics included type of ARDMS credential(s) (i.e., RDMS, RDCS, RVT), level of sonography education (i.e., certificate, associate, bachelor’s, or other), highest academic degree obtained (i.e., certificate, associate, bachelor’s, or other), years at current facility, employment status (i.e., full time or other), years in current sonographer position, and facility type (i.e., hospital, outpatient facility, doctor’s office, or other). Last, because the surveys were mailed on two separate occasions (i.e., two waves), a wave effect variable (i.e., first or second mailing) was included to address the potential for bias. Respondents in the first mailing/wave were compared with those in the second to determine whether differences existed. T tests were used to compare the means of overall affective, normative, and continuance commitment.
Data Analysis
Data from the surveys were entered into version 27 of the IBM Statistical Package for the Social Sciences. Sample size, mean, and standard deviation of the three individual commitment scales were computed and reported using descriptive statistics to answer Research Question 1. Multiple regression using a stepwise approach was used to assess relationships between respondents’ affective, continuance, and normative commitment and the study variables (Research Question 2). Because multiple statistical analyses were performed on the same data, a stratified alpha using Bonferroni-type adjustment was used to control for Type 1 errors of rejecting a null hypothesis that was true. An overall familywise error rate (alpha) of .05 remained for the study but more stringent alpha levels of .008 were used to test specific critical values. This alpha was determined by dividing the total familywise error rate of the study by 6, which represents the number of statistical analyses that would be conducted on the sample data. The equation for this adjustment is
α i = adjusted alpha, α fw = familywise error rate, and p = number of tests:
Results
Of the 1000 surveys mailed to the study sample, 110 usable surveys were received, resulting in an 11% response rate. The characteristics of the study sample are found in Table 1. Women comprised 90% of respondents. The average age of participants was 48.4 years, with the majority in the 40- to 59-year-old age range. The vast majority were Caucasian (91.8%), while African Americans comprised 4.5%. The largest percentage of respondents resided in Pennsylvania (44.5%) and Virginia (31.8%). Approximately 55% of participants held certificates in sonography, and 77.2% reported either the associate or bachelor’s degree as the highest degree obtained. Nearly 81% of the study participants were married or in a significant relationship.
Characteristics of the Study Respondents (N = 110).
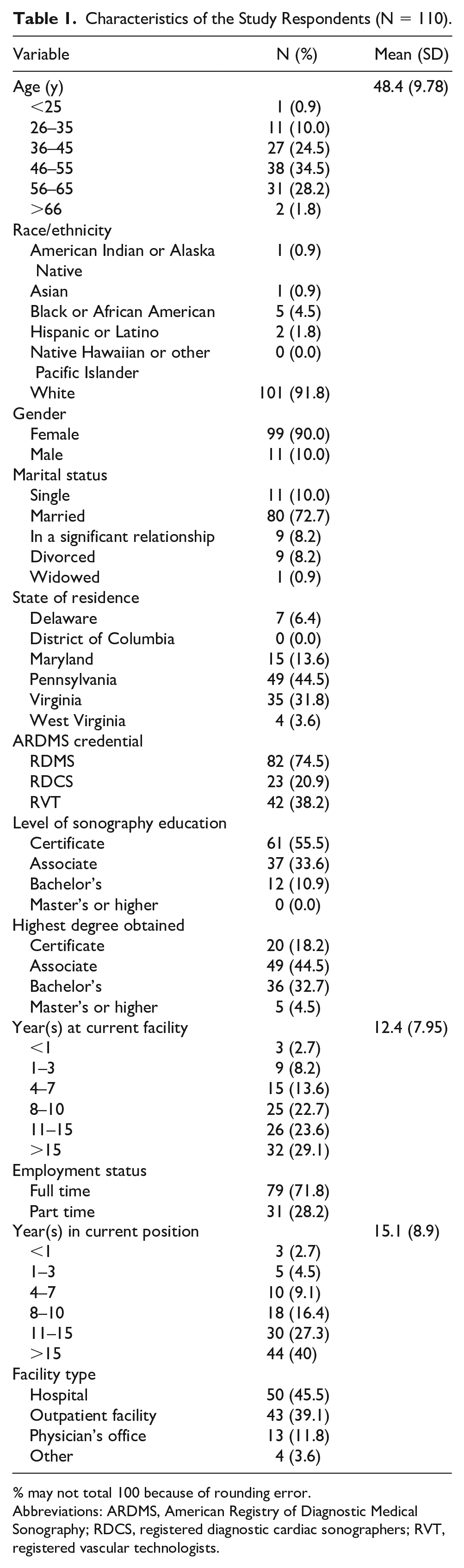
% may not total 100 because of rounding error.
Abbreviations: ARDMS, American Registry of Diagnostic Medical Sonography; RDCS, registered diagnostic cardiac sonographers; RVT, registered vascular technologists.
Almost 75% of the participants indicated holding the RDMS credential, 38.2% held the RVT credential, and nearly 20% reported holding the RDCS credential. Most survey respondents, approximately 86%, were employed in a hospital or outpatient setting; very few worked in an environment other than a hospital, outpatient facility, or physician’s office. Overall, 71.8% of the sample reported full-time employment with an average of 15.1 years in a staff sonographer position. The average number of years participants in the study had worked for their current organization was 12.4.
Organizational Commitment of the Sample
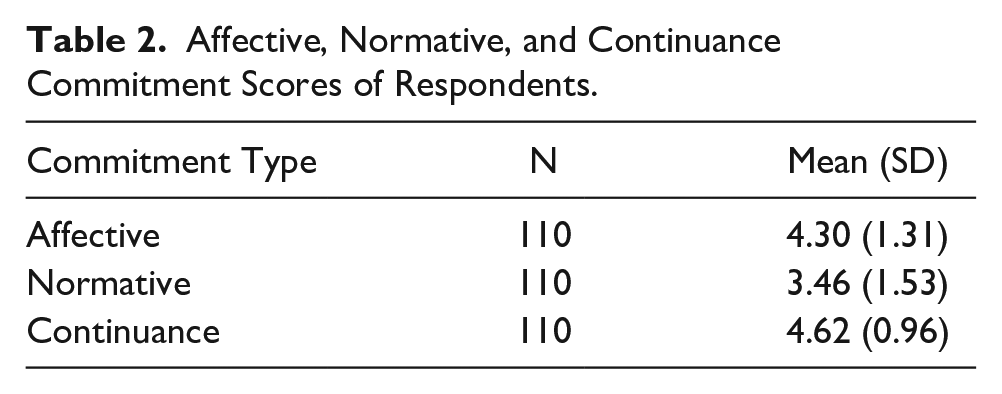
The affective, continuance, and normative organizational commitment of the sample is displayed in Table 2. With a range from 1 (strongly disagree) to 7 (strongly agree), continuance commitment had the highest mean of 4.62, followed by means of 4.30 and 3.46 for affective and normative commitment, respectively. These means place continuance and affective commitment in the “neither disagree nor agree” to “slightly agree” range. Thus, respondents demonstrated a moderate continuance commitment by remaining with the organization because of a need after evaluating the costs of leaving. The 3.46 mean for normative commitment translates as between “slightly disagree” and “neither disagree nor agree” range. The normative commitment score indicates that respondents were less likely to remain because of a sense of obligation to the organization.
Affective, Normative, and Continuance Commitment Scores of Respondents.
Relationships Between Organizational Commitment and Antecedents
As noted previously, the characteristics of the study’s participants and the date range in which they participated were identified as having a wave effect on the data. Therefore, the wave effect variable was not mentioned as a significant variable in the results that follow but should be considered because the contribution of the effect was accounted for in the regression analyses. The results of the three stepwise multiple regression models assessing whether a relationship existed between the three types of organizational commitment and study variables are found in Table 3.
Stepwise Regression Model Summary for the Affective, Normative, and Continuance Commitment.
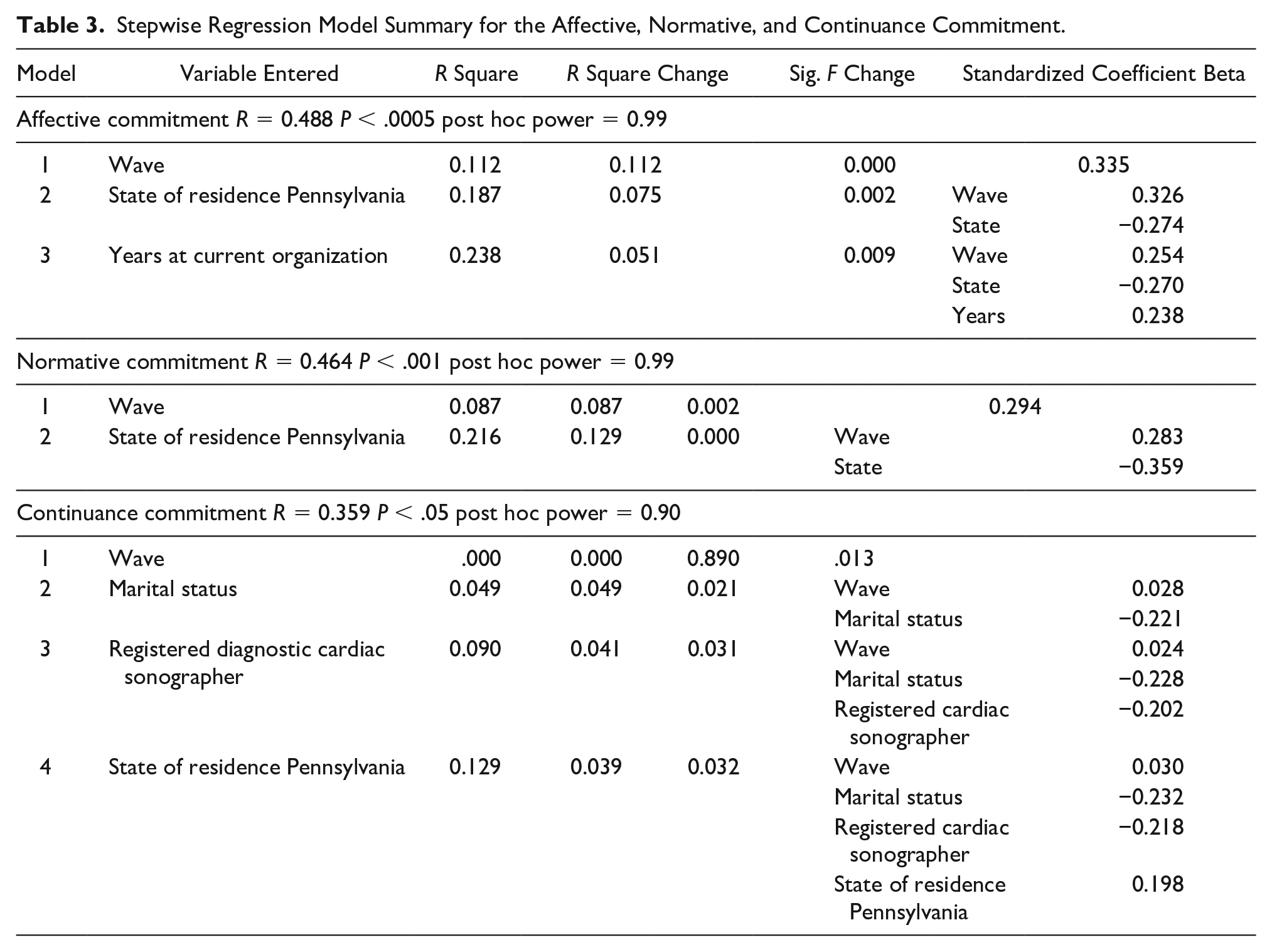
In the regression model evaluating the impact of sociodemographic factors on a sonographer’s affective commitment, residing in Pennsylvania and years at current organization were the best set of significant predictors, with a coefficient of determination (R2) of 23.8%. This indicates that 24% of the variability in a sonographer’s score in this sample on affective commitment to their organization was explained by living in Pennsylvania and the number of years a sonographer has been at their current organization.
In addition, after examining the beta weights there was no substantial change for the independent variables from model to model, which would indicate that the variance identified was describing an additional variance as opposed to variance already explained by independent variables in previous models. The highest beta weight is associated with residing in Pennsylvania, which shows a stronger relationship with affective commitment than any other predictor. In Table 3, the multiple correlation coefficient (R) of .488 seen in the best model implies a moderate linear level of association between the predictors in the regression model and affective commitment.
In the regression model evaluating the impact of sociodemographic factors on a sonographer’s normative commitment, residing in Pennsylvania was the best predictor, with a coefficient of determination (R2) of 21.6%. This indicates that 22% of the variability in a sonographer’s score in this sample on normative commitment to their organization was explained by living in Pennsylvania. In Table 3, the multiple correlation coefficient (R) of .464 seen in the best model implies a moderate linear level of association between the predictors in the regression model and normative commitment.
In the regression model evaluating the impact of sociodemographic factors on a sonographer’s continuance commitment, residing in Pennsylvania, being unmarried, and being a cardiac sonographer were the best set of significant predictors, with a coefficient of determination (R2) of 12.9%. This indicates that 13% of the variability in a sonographer’s score in this sample on continuance commitment to their organization was explained by living in Pennsylvania, being unmarried, and being a cardiac sonographer. Again, after examining the beta weights there was no substantial change for the independent variables from model to model, which would indicate that the variance identified was describing an additional variance as opposed to variance already explained by independent variables in previous models. Furthermore, the highest beta weight was associated with marital status. In Table 3, the multiple correlation coefficient (R) of .359 seen in the best model implies a low-to-moderate linear level of association between the predictors in the regression model and continuance commitment.
Discussion
The sonographers in this study had a mean score of 4.30 out of 7 for affective commitment, indicating, based on the Likert scale, they have a more than average desire to remain with the organization for which they work. Their commitment might be described as ambivalent, reflecting mixed feelings about why they are committed to their organization. They may agree with the statement, “I have somewhat of a desire to be with the organization that I work for.” Compared with national data for all occupations, this study sample’s affective commitment mean ranked at the 40th percentile. 22
The continuance commitment mean of 4.62 (out of 7) was higher, implying respondents are more committed to their organization because of the cost of leaving than they are because of emotional attachments to the organization. Among the study sample, continuance commitment was the highest commitment scale component. This finding means sonographers might agree with the statement, “I’m working for this organization because I would lose too much if I left.” Sonographers realize they have made costly investments that would be lost if they left the company that employs them. The study sample’s continuance commitment mean was higher than approximately 84% of the continuance commitment studies conducted in the United States. 22 Finally, for the sense of obligation to the organization or normative commitment, sonographers expressed less obligation to the organization (mean = 3.46 out of 7). This means, based on the Likert scale, they are not working for the organization that employs them because of a sense of obligation. They might agree with the statement, “I do not feel obligated to work for this organization.” Compared with national data for all occupations, the study sample’s normative commitment mean was higher than approximately 87% of other US-based studies. 22
Residing in Pennsylvania was the only variable that demonstrated a statistically significant relationship with all three components of commitment. Specifically, living in Pennsylvania was associated with decreased normative and affective commitment scores and increased continuance commitment scores. Although no literature was found on the influence of the state of residence on organizational commitment, it is hypothesized that salary, organization type, and workload may play a role.
Employment as a cardiac sonographer and being unmarried decreased the continuance commitment scores, while organizational tenure (years a sonographer had been at their current organization) increased affective commitment. Among cardiac sonographers, this finding may either indicate dissatisfaction with their current employer or recognition of increased job opportunities elsewhere. The relationship between organization tenure, gender, and affective commitment aligned with findings noted in the literature (i.e., no relationship between affective commitment and gender and a positive relationship between tenure and affective commitment, respectively). 1 Figure 2 visualizes the significant variables’ influence on sonographers’ organizational commitment in this study.
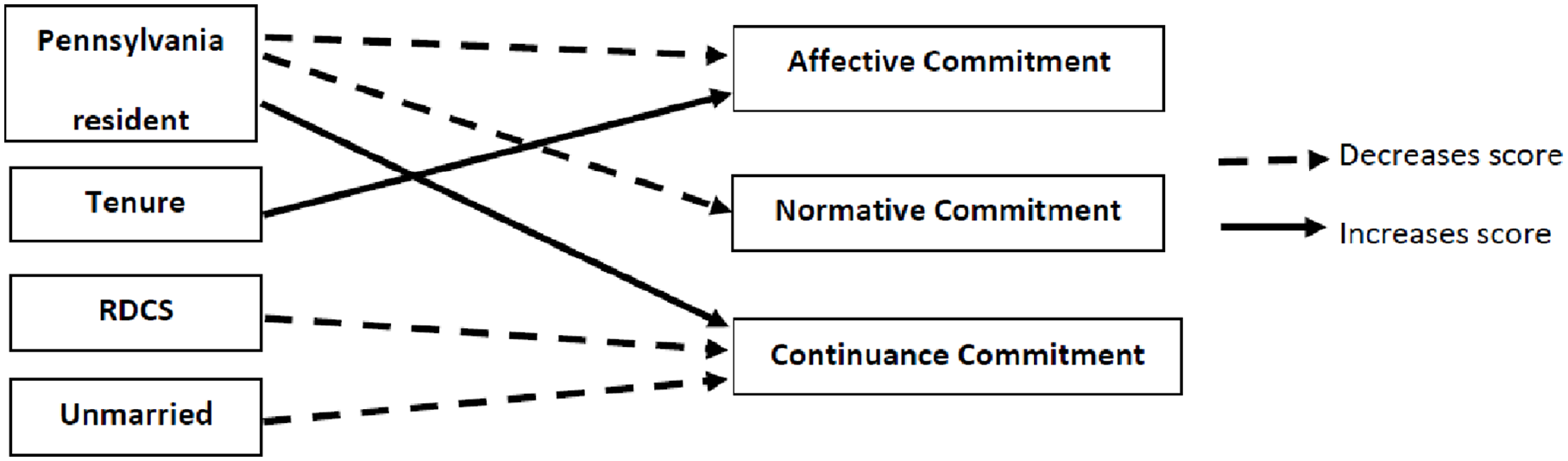
Summary of significant variables’ impact on organizational commitment in this study. RDCS, registered diagnostic cardiac sonographers.
It is evident that sonographers in the mid-Atlantic region are working for their current employers because they are truly attached to the organization and feel like they fit in, or it is too costly to leave so they remain. Although the continuance and affective commitment scores from this sample were close (4.62 and 4.30, respectively), these findings clearly show room for improvement. Improving sonographers’ commitment to the organization can circumvent negative consequences such as lack of desire to make positive contributions and feelings of resentment or frustration that can lead to inappropriate or unethical work behaviors (e.g., absenteeism, poor job performance, and increased employee turnover). 23
Examples of how human resource management policy and practice may improve an employee’s commitment include emphasizing training and skill development for future advancement/promotion. Meyer and Allen noted that recruitment and selection processes can set the stage for development of committed employees. 1 This entails creating realistic job previews to provide applicants with honest and accurate information on the positive and negative aspects of the job, as well as opportunities to evaluate the true ambience of the work environment. Also, supporting newly hired staff by assigning experienced mentors tends to increase employees’ organizational commitment. 23
This was the first study of the organizational commitment among sonographers using Meyer and Allen’s three-component model. The study may serve as a baseline for additional research such as a qualitative study allowing for a more in-depth evaluation of the work-life experiences of sonographers to gain a more robust understanding of why sonographers may possess more of one commitment component than another. For example, the following free responses from the survey suggest the need for a deeper look into the work experiences and organizational commitment of sonographers:
“[redacted] is an evil corporation that only cares about the numbers and money.”
“It’s all about the money. As long as I do as many studies as possible, they’re happy.”
“I have scaled back my hours in a hospital setting due to call. At this point in my life, I would leave the field before returning to a regular schedule of call.”
Limitations
The limitations for this study include respondent sample size and demographics, the limited geographical sampling, and the use of one credentialing body. Although the sample of 110 is lower than initial estimates, a post hoc analysis of the three organization commitment components indicated post hoc power ranging between .90 and .99. Thus, it was believed that the results indicated that this study had statistical conclusion validity. The gender and race/ethnicities of the study sample is consistent with national data wherein the vast majority of sonographers are women (86.6%) and are Caucasian (78.9%). 24
However, the study sample may overrepresent Caucasian sonographers over other races/ethnicities.
The decision to conduct a sample of a limited geographic region was based on the availability of resources to conduct the research. Likewise, one credentialing body was chosen (i.e., ARDMS) as it is the largest certifier of sonographers in the United States. The use of systematic sampling poses a threat to generalizability and external validity. Systematic sampling is not as precise and rigorous as using simple random sampling but does yield essentially similar results in a more efficient manner. 25 The low response rate could prohibit generalization of the sample to the larger population of sonographers. Using a survey could also create self-reporting bias, which poses a threat to the study’s internal validity. Last, this study was conducted during a pandemic, a presidential election, a national mail slowdown, and near the end of a typical academic semester; all of these could pose threats to the study’s external validity.
Conclusion
Using the three-component model of organizational commitment helped determine mid-Atlantic sonographers’ connection or bond with their employers. The findings indicate that sonographers believe that leaving their current employer was too costly to leave. While sonographers had some emotional attachment to the organization, there was no sense of obligation to the organization. Additional variables found to be associated with sonographers’ organizational commitment were: living in Pennsylvania, years employed at the organization, being a cardiac sonographer, and being unmarried. No relationship was found between organizational commitment and age, race/ethnicity, gender, sonography education, highest degree obtained, employment status, position tenure, or environment setting. Further investigation is warranted to document the organizational commitment of sonographers in other regions of the United States, enhance our understanding of the factors that influence a sonographers’ organizational commitment, and implement practices and policies that would improve the workplace environment for clinical staff and, potentially, increase patient satisfaction and safety. These results are important since lower scores seen on each of the three components of commitment have been related to negative workplace behaviors and could impact clinical operations. Employers must strive to know and understand the organizational commitment scores of sonographers in their ultrasound department to maintain a stable ultrasound workforce team, lessen turnover and unwanted behaviors, and aim to have sonographers who are working for their organization because of a desire to do so.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The institutional review board of Virginia Commonwealth University classified the research as exempt from ethics approval and informed consent according to 45 CFR 46.
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study.
Trial Registration
Not applicable.