
Abstract
Objective:
To identify factors influencing sonographers’ practices in communicating adverse obstetric findings and to understand their views on the need for standardized national policies and guidelines.
Methods:
Qualified and trainee sonographers who currently perform obstetric sonography were invited to complete a survey through the Australasian Sonographers Association. Closed-ended questions sought information on the demographic profile of the participants and their experiences on a range of issues related to workplace practices and policies. Open-ended questions allowed respondents to elaborate on workplace interactions and their views on the communication roles of sonologists (radiologists and obstetricians) and sonographers.
Results:
The practice setting, the background of the sonologist, the type of adverse finding, and the trimester in which a patient is scanned have an impact on the level of difficulty for sonographers in obstetric communication. These findings highlight a lack of uniformity of sonographer and sonologist communication with patients due to limited training, lack of formalized departmental policies, inadequate support, and communication practices by radiologists. As a result, respondents strongly supported the development of a standardized national policy.
Conclusion:
In the current environment of patient-centered care, sonographers are in a challenging position as they do not have policies supporting them as independent health care professionals, autonomously deciding on the best approach to communicate findings with their patients. This may lead to anxiety and stress if they lack control over the interaction. More support from sonologists in a radiology setting is needed. These findings should encourage professional bodies to address these issues by working collaboratively and to recognize the importance of the sonographers’ role and their unique position with pregnant patients.
Keywords
Sonography is the gold standard for prenatal diagnosis of adverse findings in the 21st century.1,2 Technological advances have dramatically improved the visualization of fetal and maternal structures and the recognition of abnormalities.
In Australia, the majority of diagnostic obstetric sonograms are performed by accredited sonographers. 3 They provide a comprehensive image set and a summary worksheet for a sonologist (radiologist or obstetrician) to provide a final written report for the referring physician. Obstetric sonography in Australia is performed in a variety of settings: public and private hospitals, privately owned radiology or obstetrics practices, and rural and remote locations with remote reporting. As frontline practitioners, sonographers have direct contact with the patient and utilize high levels of interpersonal skills during the examination. This can be challenging, as pregnant patients expect and sometimes demand to know results immediately.4–7
Formal policies and departmental protocols are particularly problematic in obstetric sonography settings in Australia. 8 Where they do exist, some state that the sonographer is not permitted to provide feedback; others offer ambiguous information regarding the role of the sonographer in communicating adverse findings. 9 This puts sonographers in a challenging and potentially stressful position, as they risk betraying a patient’s trust in not disclosing the findings.10–14 In some practices, the sonologist will attend the patient to discuss an adverse finding if asked to do so by the sonographer. Increasingly sonologists lack the time or willingness to be directly involved with patients, 15 and some referring physicians may request nondisclosure of results by the sonography practice.16–19 Both these situations put further pressure on sonographers in their direct interaction with pregnant patients.
This study sought to identify factors influencing sonographer practices in communicating adverse obstetric findings, including sonologist influence, departmental policies or protocols, and sonographers’ views on the need for standardized national policies and guidelines.
Method
Research Design
A pilot study with semistructured interviews was conducted in 2015 by one of the coauthors (S.T.), a qualified obstetric sonographer. The issues and concerns raised by interview participants relating to their sonographer role, communication practices, and professional relationships within workplaces were incorporated into the 2018 online survey being reported here. The survey instrument was piloted with five qualified obstetrics sonographers and one student sonographer. Their feedback on content, structure, and time taken to complete the survey were incorporated into the final instrument administered nationally to sonographers. The survey included 30 closed-ended and 3 open-text items. The closed-ended, quantitative questions are reported here. The results of the qualitative, open-text questions have been published elsewhere. 15
Ethics approval for the survey was granted by the University of Sydney Human Research Ethics Committee (ethics approval 2017/932).
Participants and Recruitment Strategy
An invitation to participate in the survey was disseminated through the weekly online newsletter of the Australasian Sonographers Association (ASA) for 5 weeks in April-May 2018, with a weekly reminder. Participants were sonographers qualified to perform obstetric examinations or trainee student sonographers working under supervision in a clinical setting performing obstetric sonography. All 249 participants provided responses to the 30 closed-ended questions in the survey instrument.
Sample
The study population consisted of a possible 3715 qualified or student sonographer members of the ASA. The study sample consisted of 245 qualified sonographers and 4 student sonographers qualified or training to perform obstetrics (representing 15% of the ASA membership that is accredited or is training to perform obstetrics as part of ultrasound qualifications).
Instrument
The online survey data were collected and managed with Research Electronic Data Capture (REDCap), a secure web-based application. 20 The closed-ended questions sought information on the demographic profile of the participants and their experiences on a range of issues related to work practices in performing obstetric sonography, particularly in the case of a diagnosis of an adverse finding. The questions also sought information on workplace interactions among sonographers, sonologists, and pregnant patients, such as “How often does a sonologist communicate an adverse finding(s) to a pregnant patient in your department?” and “Which circumstances do you believe are acceptable for a sonographer to communicate an adverse finding(s) to a pregnant patient?”
Participants had the option of completing three open-text questions at the end of the instrument; this allowed for elaboration on closed-ended items and/or additional comments, such as “Do you think it should be part of the role of the reporting sonologist to directly communicate an adverse finding(s) to a pregnant patient?” and “Any additional comments you would like to make?” The response rate to the open-text questions was high, demonstrating participants’ engagement with this issue.
Data Preparation and Analysis
Data were analyzed with IBM SPSS Statistics 24 and NVivo12 analysis software.21,22 Descriptive statistics were performed, including frequencies and cross-tabulation analyses, across all demographic information against workplace setting, reporting sonologist, and level of communication. The significance threshold for the chi-square analyses was set at P < .05.
Results
The findings reported here were drawn from analysis of the closed-ended survey items with key points supported by selective extracts from the open-text responses.
Demographics
The demographic data were representative of sonographers currently practicing obstetric sonography throughout all settings in Australia. 23 Survey respondents were mainly female (84%), with an even representation across age groups. The gender and age distributions are consistent with the general Australian sonographer population. 24 Over half were qualified for more than 10 years (56.2%), and 54% reported working the equivalent of full-time employment (33+ hours per week) (Table 1).
Surveyed Sonographers’ Personal Characteristics (N = 249).
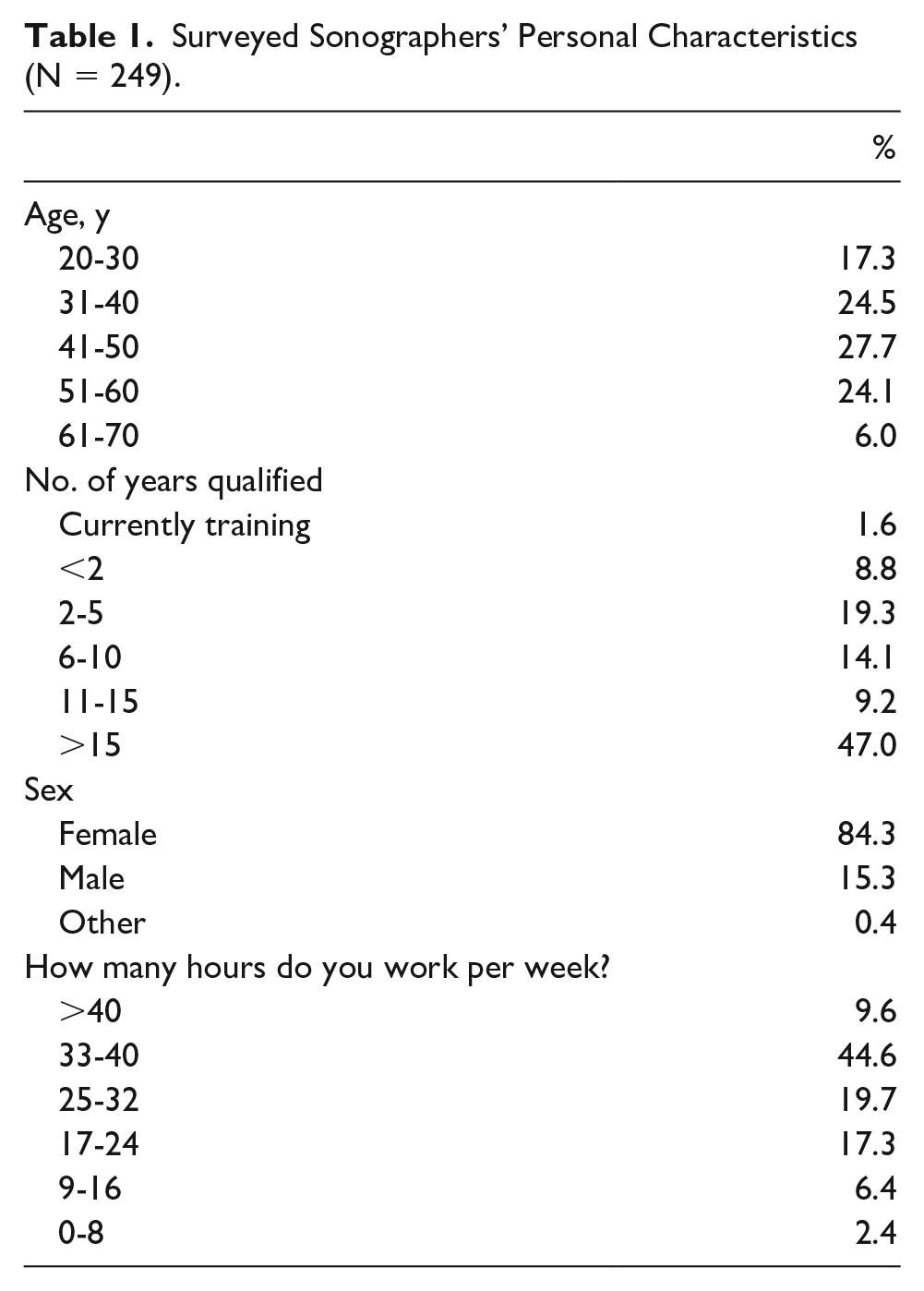
Most sonographers work 33 to 40 hours in metropolitan centers (55%) within a radiology setting (52.7% corporate or radiologist owned), followed by public hospitals, with most indicating that they perform scans in all trimesters. The majority of sonographers are in practice sites that have no departmental policies or training in place in how to communicate adverse findings, and most debrief with colleagues if they feel distressed (Table 2).
Surveyed Sonographer Workplace Characteristics (N = 249). a
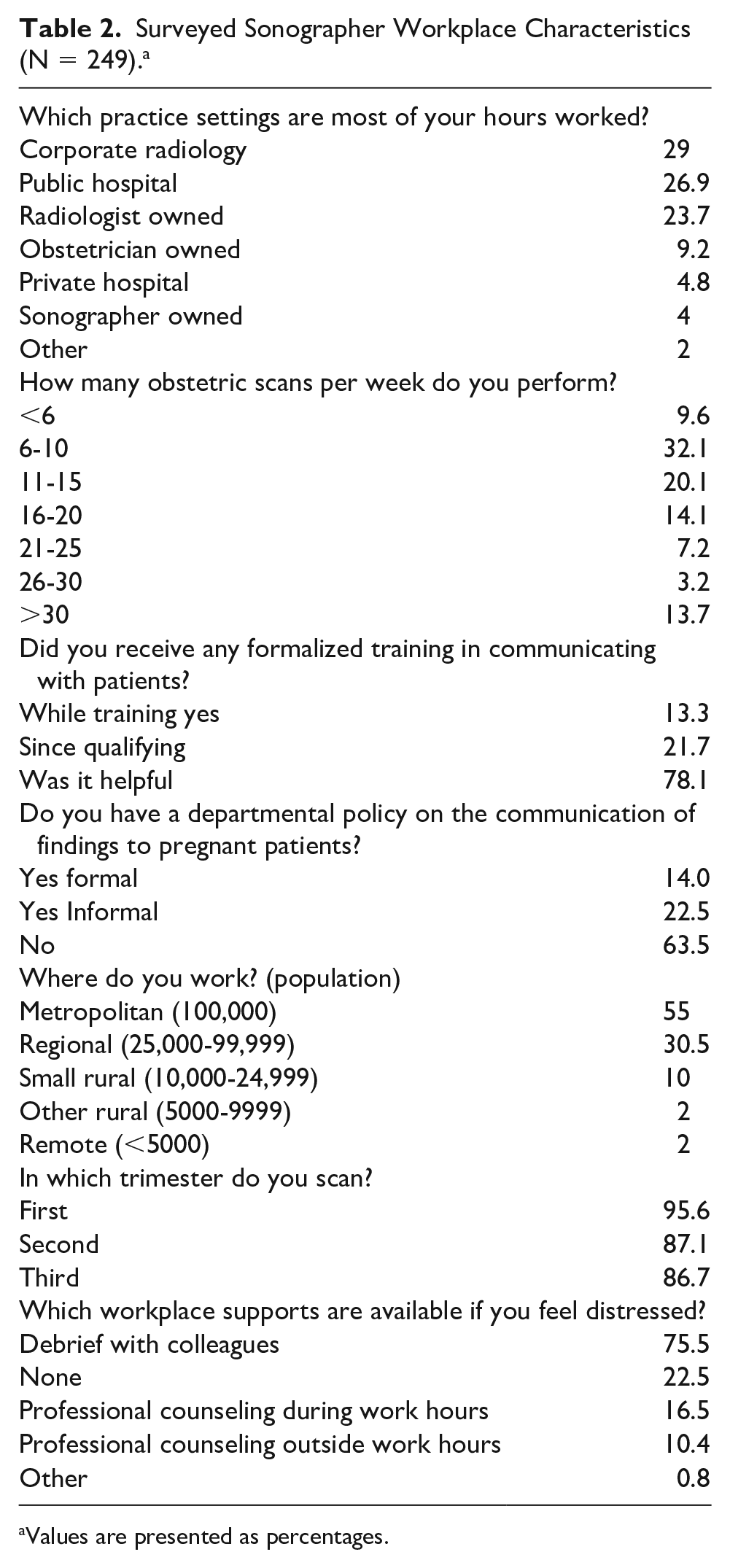
Values are presented as percentages.
Sonographer Communication
Most respondents (93.6%) have communicated an adverse finding directly to a pregnant patient, irrespective of whether there was a departmental policy in place. Most of the 249 sonographers (91%) believed it to be part of the sonographer’s role to communicate adverse findings directly to a patient, as compared with a limited number (6%) preferring not to be involved in communication, as they believed that it was the role of the referrer or sonologist. Open-text responses conveyed sonographers’ views on this: I would like to see this seen more widely as an accepted part of a sonographer’s role. Autonomy is an important aspect of our workplace.
An example of an open-text response against a formal policy on communicating adverse findings included the following: As a health professional, it important to have some flexibility and discretion rather than set rules.
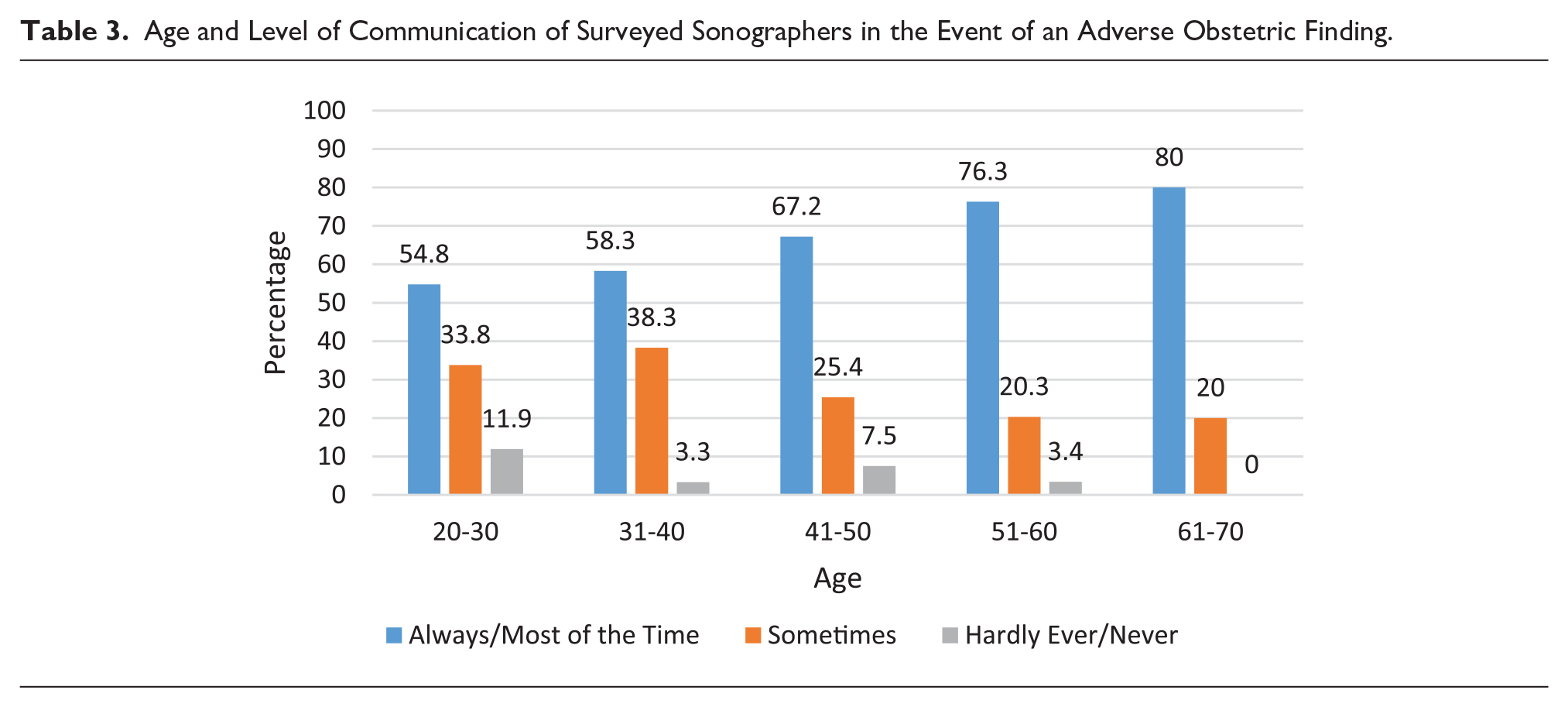
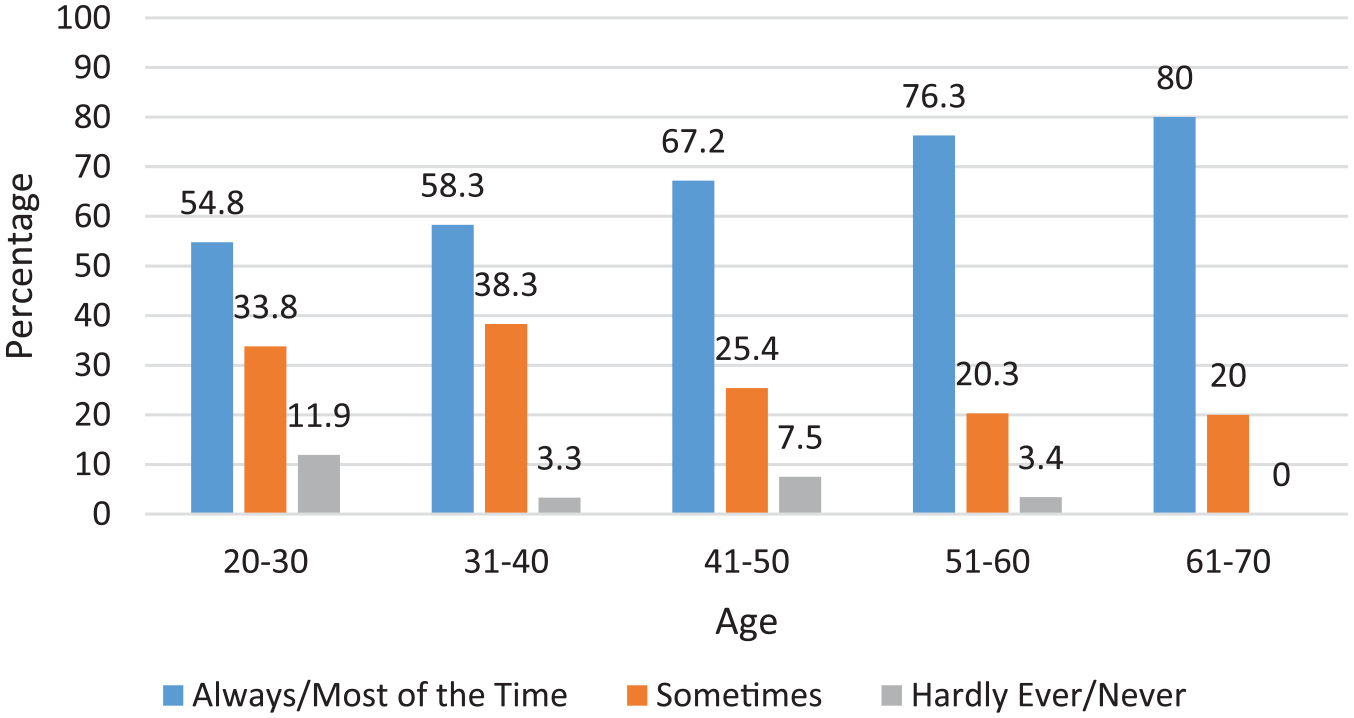
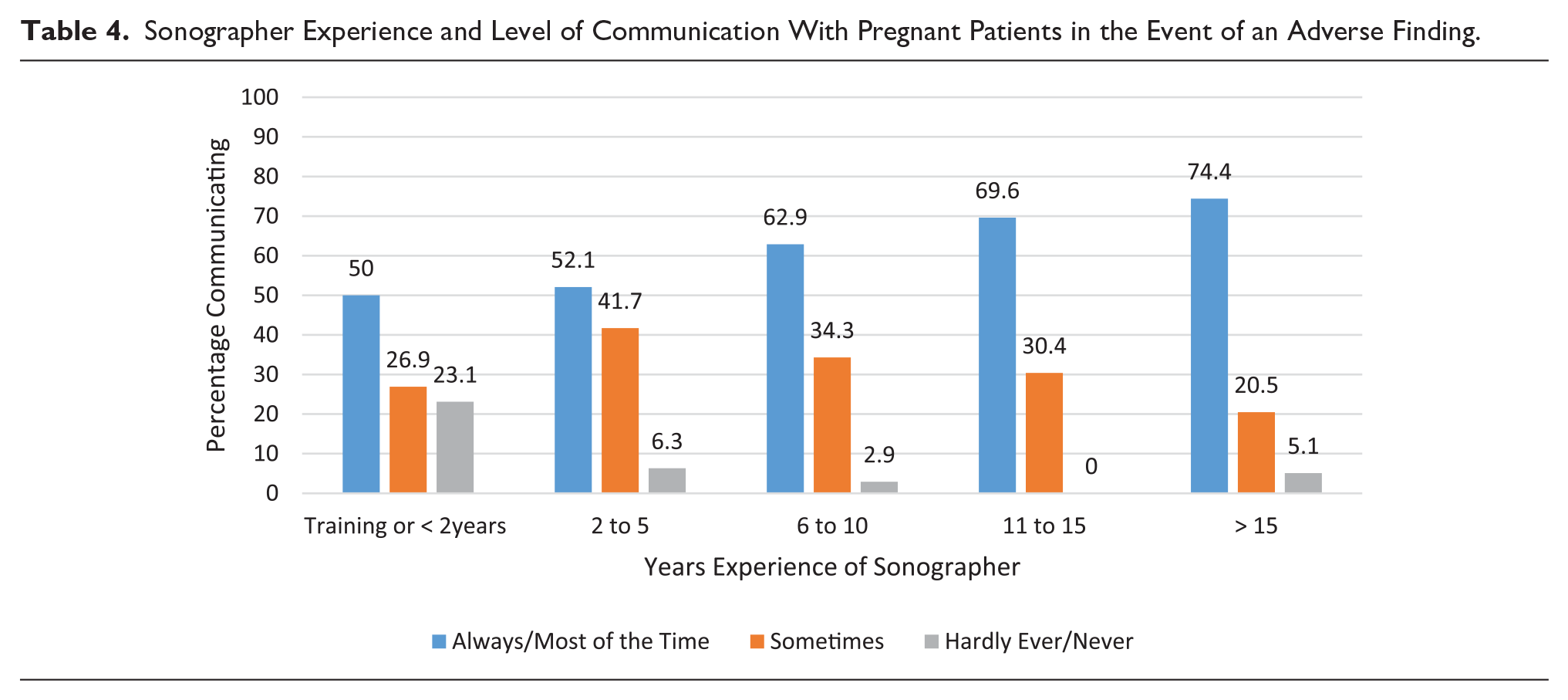
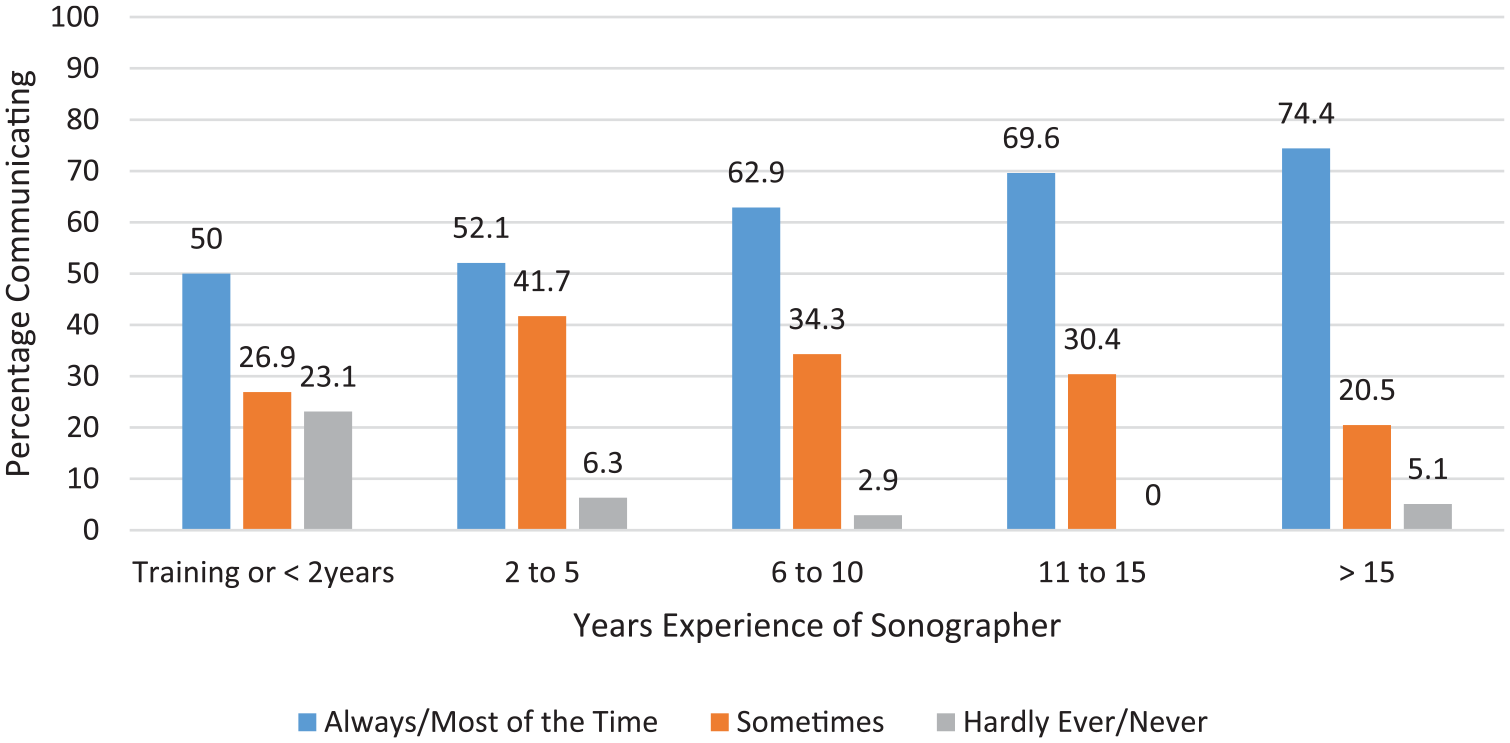
Respondents’ views on their role in communicating adverse findings showed no significant relationships with practice locations or gender. With increasing age and scanning experience, however, there was an increase in sonographer communication of adverse findings (Tables 3 and 4). One experienced sonographer reported, I have many years’ experience (over 40 years in fact) in ultrasound and also a lot of “life experience” and empathy qualities which I personally feel helps me deliver news to patients and partners . . . especially as I have more than likely already formed a rapport with the patient and partner as opposed to a “stranger” in the form of a radiologist entering the room.
Age and Level of Communication of Surveyed Sonographers in the Event of an Adverse Obstetric Finding.
Sonographer Experience and Level of Communication With Pregnant Patients in the Event of an Adverse Finding.
Factors Influencing Communication Practices
Although the clear majority of sonographers expressed their desire to communicate with pregnant patients, the situations in which sonographers do communicate were explored further. Survey respondents were asked to report on the nature of the adverse findings that they had communicated to any pregnant patient from examinations undertaken in the month prior to completing the survey. The most common was a miscarriage or fetal demise (Table 5). All participants had communicated some form of adverse finding to patients in the previous month.
Adverse Findings Communicated to Pregnant Patients by Sonographers in the Month Prior to Survey. a
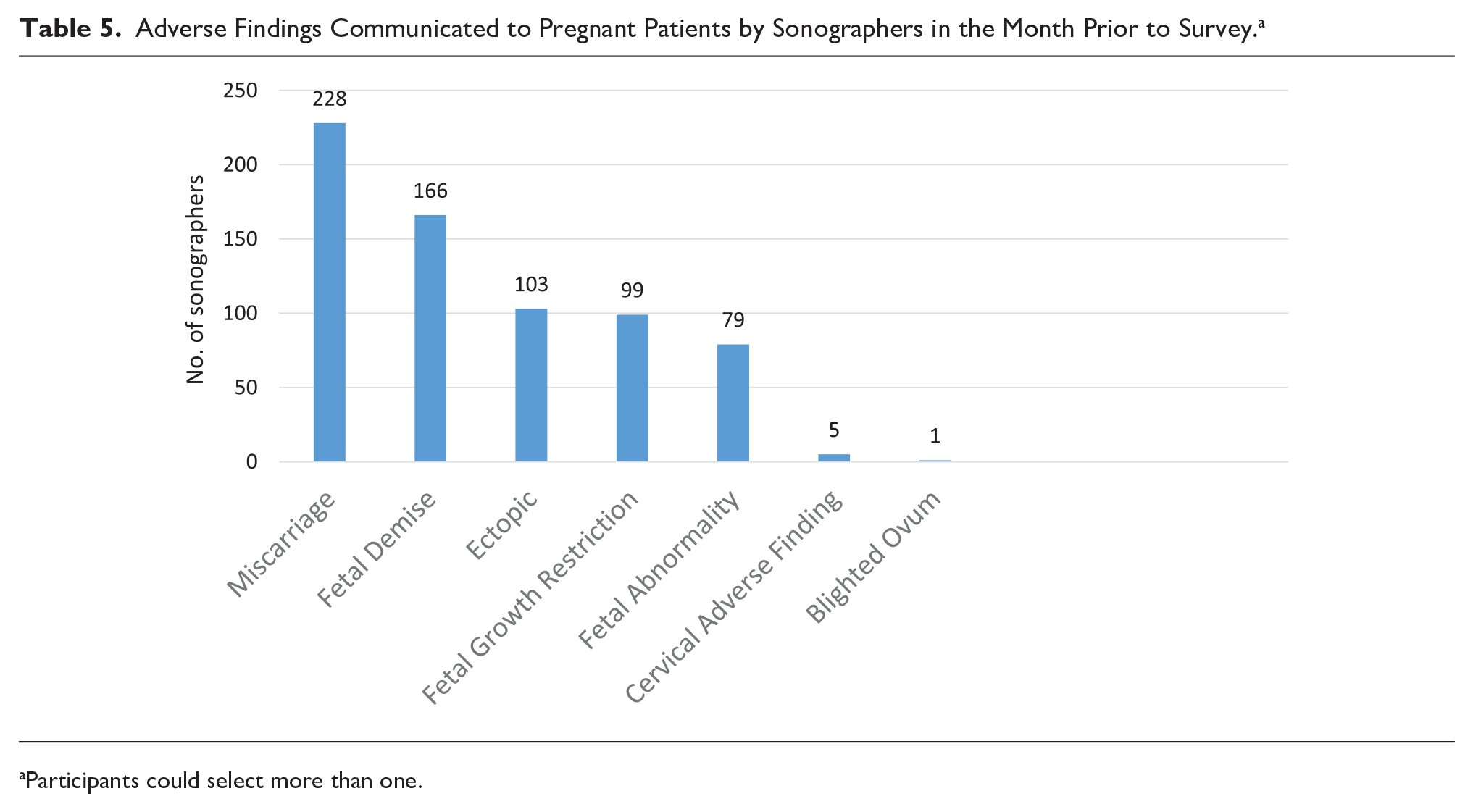
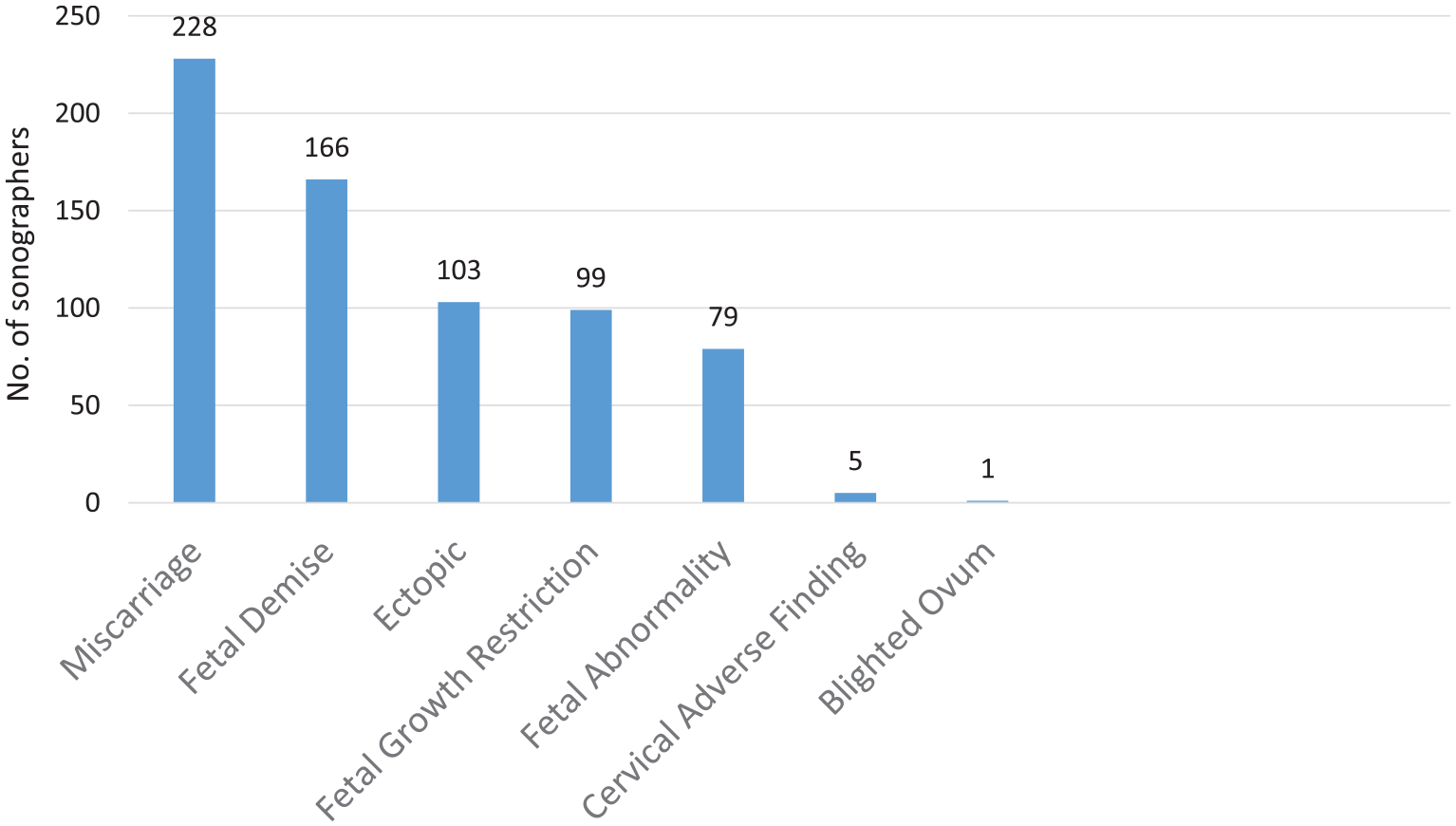
Participants could select more than one.
To understand the circumstances in which sonographers believe that it is acceptable to communicate adverse findings directly to patients, respondents were asked what would influence their decision making. Most sonographers (71.9%) believe that it is acceptable to directly communicate the absence of a fetal heartbeat, while only 28% indicated that they would do this if unable to consult a sonologist first (Table 6). Participants selected “other” for various reasons: some believed that it was not the sonographer’s responsibility, or they did not feel capable or confident in communicating the findings.
Factors Contributing to Surveyed Sonographers’ Comfort Level in Communicating Adverse News Directly to a Patient. a
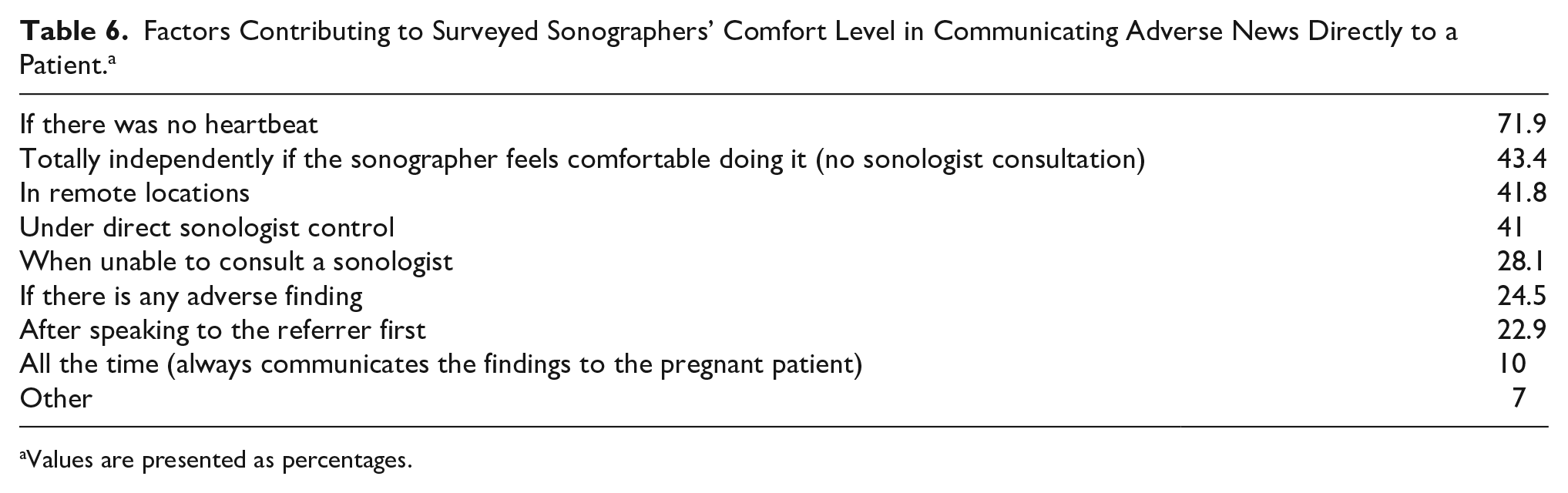
Values are presented as percentages.
A limiting factor in sonographers’ communication is the direct sonologist control of a sonographer’s actions, as it inhibits sonographer autonomy in decision making (41%). A further limitation is a demand for nondisclosure of results by the referring physician (23%), as this control affects the ability of the sonographer to be open and honest with the patient. Typical responses included the following: Each practice and each radiologist/sonologist wants something different. Each day, we have different reporting doctors who have differing expectations of what we tell the patients. We have had issues with visiting obstetricians objecting to us communicating with patients and demanding we tell our ladies nothing. Referring doctors often want to impart this information to their patients.
Sonographers found the most difficult situation in which to communicate adverse findings was at the routine 18- to 20-week sonogram (43.8%), with a third reporting that it is the third-trimester scan, and more than a third (35.3%) finding it difficult at any stage. However, if the sonogram was carried out due to the doctor’s or the patient’s concerns about the pregnancy, then very few (4.8%) found it stressful to communicate results given that the patient is already aware there could be a problem (Table 7).
Examples of Difficulty in Communicating Adverse Sonographic Findings. a
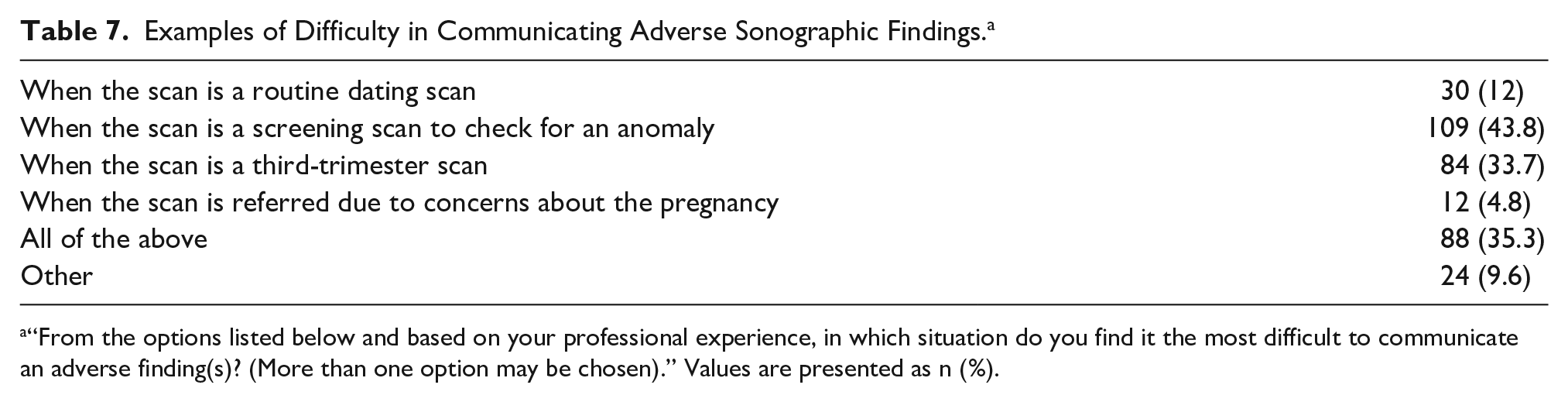
“From the options listed below and based on your professional experience, in which situation do you find it the most difficult to communicate an adverse finding(s)? (More than one option may be chosen).” Values are presented as n (%).
Departmental Policies and Guidelines
Several questions explored the existence of departmental policies for communicating adverse findings to pregnant patients, and results were compared among practice settings, locations, and reporting sonologists. Only 14% of respondents had a formalized departmental policy in place, with a further 22.5% having an informal policy (Table 2). The smaller practice settings, such as obstetrician-owned specialist practices and sonographer-owned practices, reported the highest percentage of policies in place (47.8% and 50%).
The desire of sonographers to have a national standardized policy, one to which all professional bodies agreed, was also investigated. Respondents strongly supported a standardized national policy (76%) irrespective of whether there was an existing departmental policy (Table 8). This was captured in the following text responses: Standardized policy = standardized practice! Uniform standard of practice would result in less complaints and greater patient satisfaction! A standardized policy would help sonographers to know when and what information is appropriate to tell patients but this would vary between settings, e.g. specialist obstetric practice to small regional radiology practice.
Desire for a Standardized Policy vs Currently Having a Departmental Policy in Place (One Response Allowed).
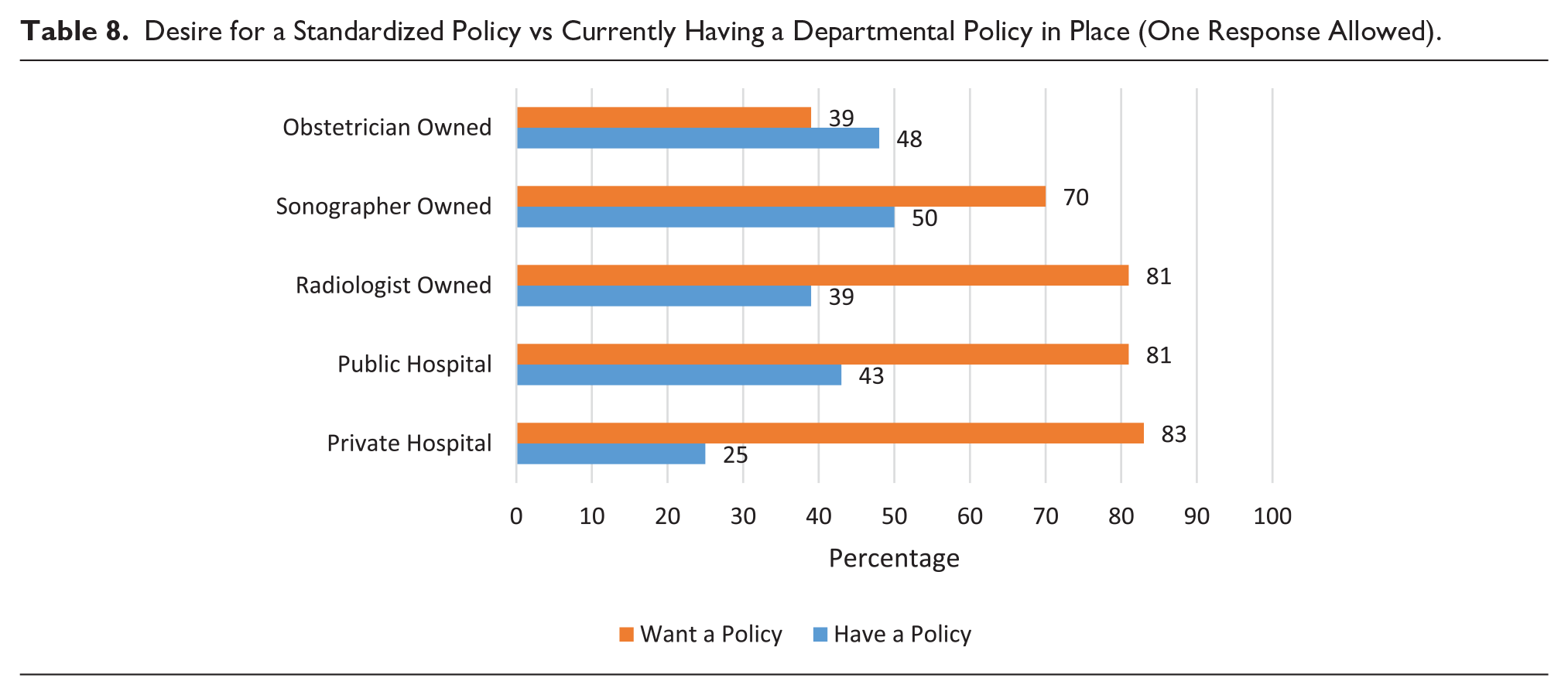
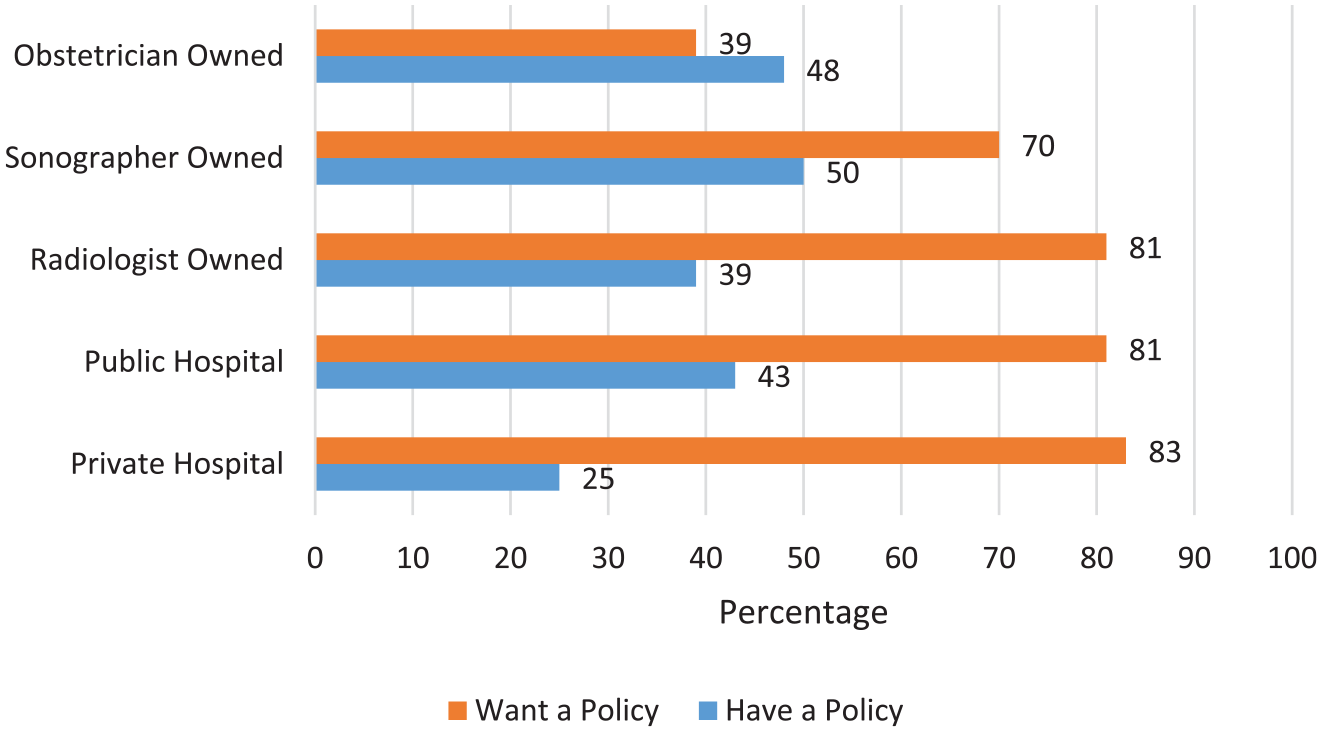
The one exception to this was in obstetrician-owned practices. The following quote reflects the support and backup that sonographers feel that they have while working in this specialized setting: I work in fetal medicine so there is a lot of support and knowledge and experience so communicating information like this with a patient is a lot easier to do compared to a general sonographer.
Sonographer Training and Support
Only 13.3% of respondents reported receiving any training in how to communicate adverse outcomes before they qualified as a sonographer, and 21.7% had undertaken training since qualifying. Lecture-based training was the most common format, with 2.5 hours being the median time spent in training. The majority of the respondents who had undergone training found it helpful (78%). Options available to sonographers, if they felt distressed after communicating adverse findings, showed that debriefing with sonographer colleagues was most prevalent (75.5%); however, 22.5% reported not receiving any form of support. A small proportion of respondents had professional counseling available during work hours (16.5%) or outside of work hours (10.4%).
More training on how to deliver the bad news would be extremely useful. I think more effort should be made to improve sonographers’ mental health and well-being. It is a difficult job that can have huge ramifications, and little support is provided.
Impact of the Sonologist Background
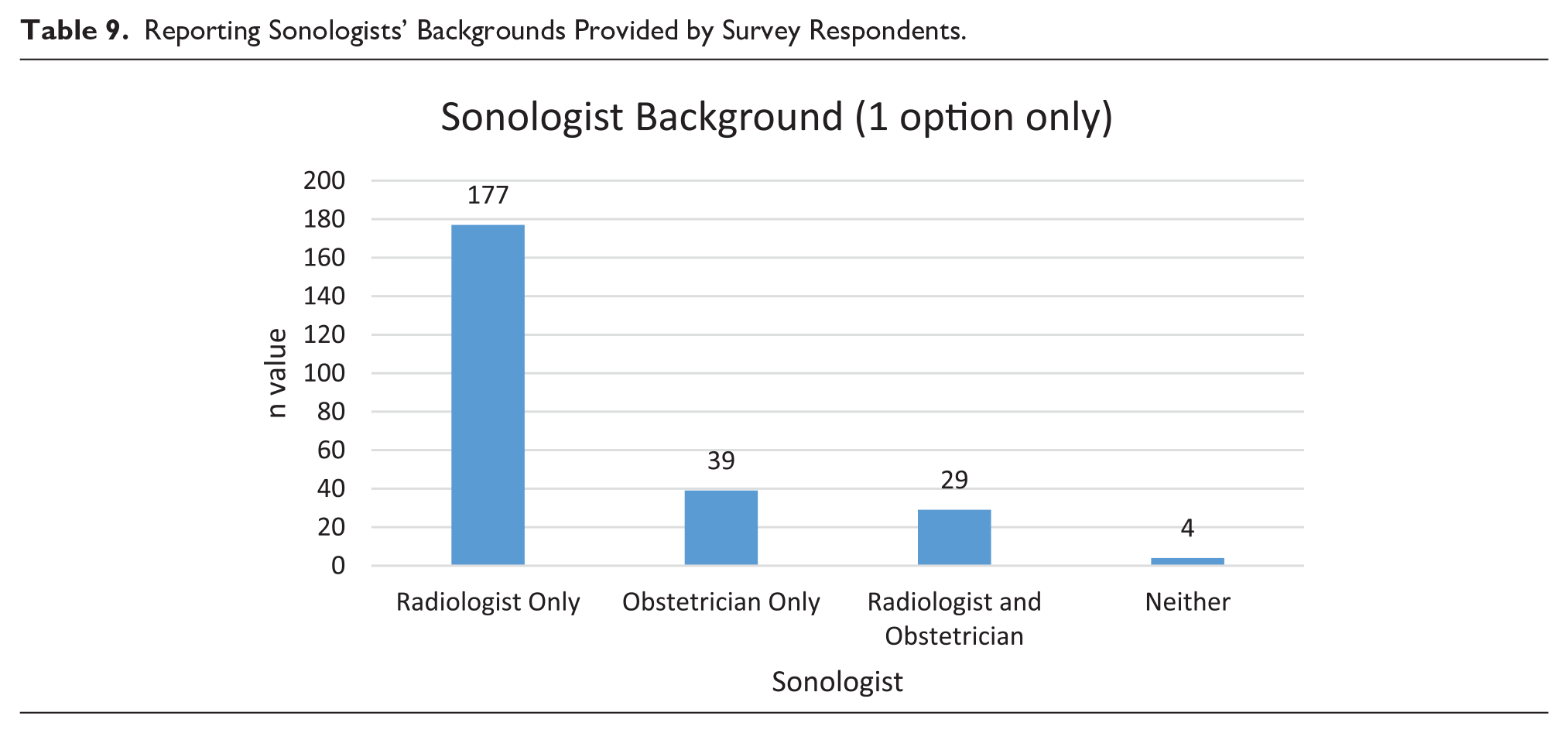
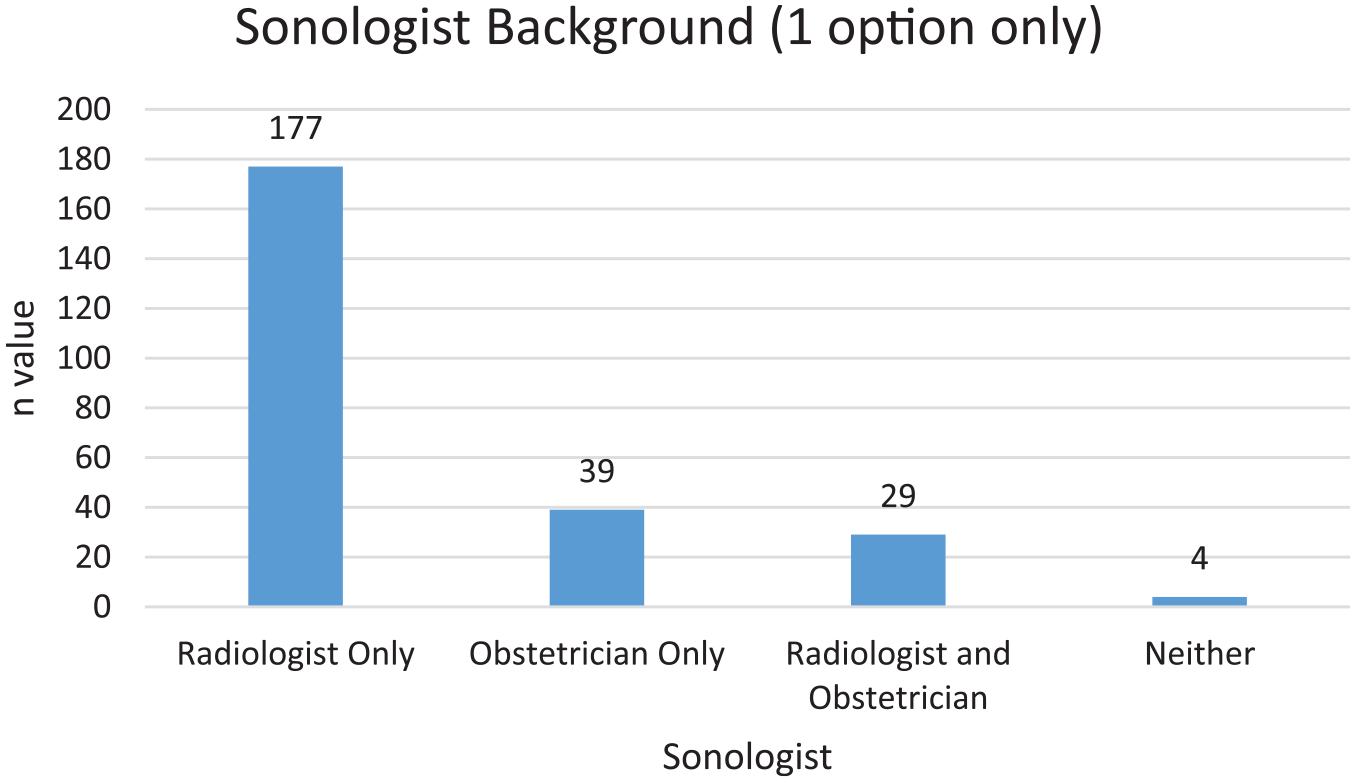
Variations between sonologists’ medical specialty and their level of involvement with patient communication were investigated. These results are based on categorizing respondent sonographers into four groups, defined by the type of sonologist reporting on the scans. The first group, “radiologist only” (n = 177), includes respondents who had only radiologists reporting on scans. Respondents who had only obstetricians reporting on sonograms were termed the “obstetrician-only” group (n = 39). Some respondents worked in situations where both radiologists and obstetricians reported on their sonograms (29). A small number of respondents had neither a radiologist nor an obstetrician reporting (n = 4), and these were excluded from this analysis (Table 9).
Reporting Sonologists’ Backgrounds Provided by Survey Respondents.
Impact on Sonographers
As might be expected, in the obstetric-only group, the majority (87.2%) of respondents scanned more than 16 obstetric cases per week, as compared with 29.1% for the other two groups combined, χ2(7) = 87.813 (P < .001). They also had more training in communicating with pregnant patients (43% vs. 18.1%), χ2(2) = 11.549 (P < .003).
Most sonographers in the radiologist-only and obstetrician-only groups reported communicating findings directly with patients, while only 7% of respondents rarely communicated with their patients. In the combined radiologist-obstetrician group, sonographers showed a significantly higher communication level, with 51.7% reporting that they “always communicate,” χ2(4) = 10.131 (P < .038).
Respondents reported significant differences in the level of communication to which their sonologists engaged with patients (Table 10). In the radiologist-only group, respondents stated that 62% of radiologists “hardly ever” or “never” communicate findings, as compared with only 2.6% of the obstetrician-only group, χ2(4) = 50.420 (P < .001). The radiologist-only group was significantly less likely to communicate findings “always” or “most of the time” as compared with the obstetrician-only group (11.9% vs. 71.8%), χ2(4) = 93.917 (P < .001) (Table 10). This open-text response is an example of the variation among radiologists: Some radiologists have an interest in obstetrics, or are invested in giving a higher level of service to their referrers/patients.
Current Sonologist Communication With Obstetric Patients Reported by Respondents. a
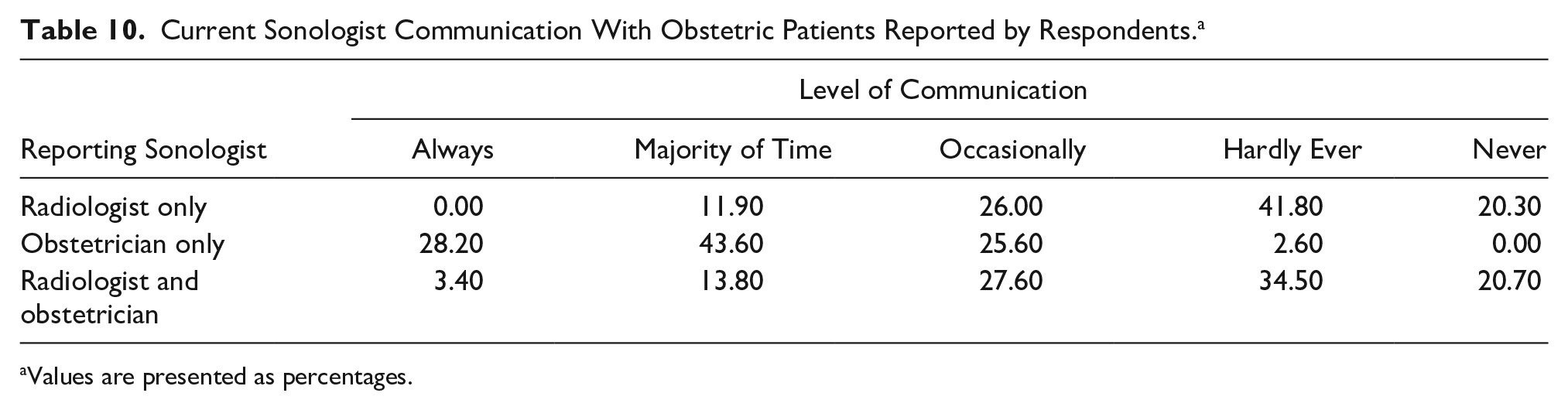
Values are presented as percentages.
Respondents’ views on the sonologist role in communicating findings to a pregnant patient showed significant differences. When compared with the obstetrician-only group (35.9%), the radiologist-only group did not believe that it was the sonologist’s role, other than it being necessary in “some cases” (72.3%), χ2(2) = 20.924 (P < .001). However, in contrast to the radiology-only group (21.5%), the obstetrician-only group believe that it is the sonologist’s role to do the communicating (64.1%), χ2(2) = 27.028 (P < .001). The following open-text response reflects the greater support provided in dedicated fetal medicine (obstetrician reporting) departments as compared with general radiology practices: I work in an obstetric hospital and we have a good pathway of communication between other teams and specialists who are available to assist in the event of complex adverse findings and early first trimester losses.
Discussion
Sonographer-performed examination for prenatal obstetric assessment is routine in Australia, the United States, Canada, and the United Kingdom. Sonographers have the ability to diagnose adverse findings, given their frontline diagnostic practitioner status. 25 Importantly, it has been widely acknowledged that the person scanning is responsible for documenting any abnormalities with appropriate image selection, ultimately instigating the diagnosis.25,26 An essential rapport is established between the patient and the sonographer during a sonographic examination. Despite this, in Australia there is a lack of uniformity in policy, practice, and expectations surrounding communication of adverse findings with the patient, who expects nothing less than full information. 15
The current study found that the majority of Australian sonographer respondents are communicating adverse findings directly to pregnant patients. This is despite limited training, the type of adverse finding, and sonologist instructions. Only a small number of sonographers had received training in carrying out this sensitive task. There is no requirement for sonographers in Australia to have attended an accredited course and achieve competency in this area. This lack of training contributes to a lack of uniformity in a sonographer’s actions and comfort level 27 when confronted with an adverse finding during a scan. It was not surprising that as a sonographer’s experience and age increased, so did the frequency of communicating an adverse outcome.
This study also found that adverse findings in the first trimester, such as the absence of a fetal heartbeat and miscarriage, are more likely to be directly communicated by sonographers. This may be due to the fact that a fetal death is difficult to conceal, as the expectation of seeing a normal active baby is anticipated and patients find it stressful if this information is withheld. 6 This is supported by multiple studies showing that women value immediate, clear information from a sympathetic newsgiver who is clearly focusing on their needs.4,28
A critical finding in this study was the impact of interprofessional role boundaries on sonographer practice, with 41% of respondents communicating adverse outcomes directly to patients only with the sonologist’s approval. This external control over the sonographer’s autonomy to communicate can cause distress and confusion for pregnant patients, as they expect that sonographers will convey the findings directly to them at the time of the scan.12,13,29,30 Referring physicians also have the power to limit a sonographer’s autonomy if they indicate that there should be no direct communication with the patient at the time of the sonogram. This is significant in the context of Australia’s health care system, which is structured around supporting patient-centered care and patient empowerment, with open communication between patients and all health care professionals. 31 This puts sonographers in a challenging position, as they are organizationally under the control of the sonologist who, in effect, influences the interaction between the sonographer and the pregnant patient. This position is exacerbated by the definition provided by radiology’s professional body, the Royal Australian and New Zealand College of Radiologists, 8 which clearly states that sonologists and referring physicians decide who can communicate with the patient. This places the sonographer in a subordinate role to the sonologists, which is consistent with the medically dominant structure of the Australian health care system.32,33 As a consequence and as Palmer and Short 34 suggest, various interest groups influence health policy making, and there are discrepancies between the “model” and the “reality.” This could be the reason why there was overwhelming support from sonographers for a standardized national policy and guidelines. As it stands, they may be unsure of their professional status, accountability, and legal stance if they directly communicate results to pregnant patients prior to the sonologist writing the final report. 8 In Australia, McGregor et al. 35 and Lewis et al. 36 suggest that the authority to instigate and formalize policies is hampered by medical specialists’ powerful position in setting role boundaries. If sonologists cannot accept honest and open communication by sonographers, this will cause frustration for the sonographer and loss of trust from the patient.
Unlike the situation in the United Kingdom, where sonographer practitioners report independently, 37 policies and professional guidelines on communication in Australian obstetric sonograms may be ambiguous. 9 Sonographers have been performing advanced practitioner roles over the last 30 years in the United Kingdom, 38 and there is extensive evidence that open communication with a patient, independent of a sonologist, has improved the patient experience. 39 Simpson and Bor 13 highlighted that the anxiety that sonographers experience in delivering adverse outcomes could be reduced only with structured guidelines and policies.
The lack of control over patient interaction and communication can cause stress and anxiety, and it can be compounded if sonographers feel that they do not have the support from the reporting sonologist. 9 This affects the sonographer’s ability to build a trusting relationship with the patient, which Asplin et al. 40 and Larrson et al. 41 found to be vital for a patient’s confidence in the health professions.
The current study found that most sonographers exercise some autonomy in their everyday practice, as evidenced by the level of communication in which they already engage. In particular, sonographers who work with radiologists reported that radiologists have very limited contact with pregnant patients when there are adverse findings, so the sonographers undertake the necessary task of communicating with the mother. This was in contrast to the obstetrician-run practices, with obstetricians more often communicating findings to the patient. Sonographers who work in privately owned obstetrician-run specialty practices have more departmental policies in place and more obstetrician support and had training in delivering adverse outcomes. This finding is consistent with a study by Ramsay and Fracchia 42 showing that obstetricians work as a team with sonographers and have a high level of involvement with their patients.
This study demonstrates that obstetrician-run and sonographer-owned practices were generally much smaller than radiology practices, pointing to such practices being able to support and instigate policies uniformly. Larger organizations, such as large hospitals and corporatized private practices, struggle with this, as they have many reporting sonologists and therefore no policies or potentially multiple individualized policies.
Most respondents believed that insufficient support mechanisms were in place for sonographers affected by adverse cases. Most found that debriefing with colleagues was their primary avenue of support. This may lead to increased pressure on fellow sonographers who lack the qualifications and time to assist others in overcoming stress on top of their individual needs.
It is difficult to measure the impacts of poor support and lack of policies on outcomes, effectiveness, and efficiency. Like Brasseur, 5 this study found that sonographers have a unique and complex relationship with the patient. This is undervalued and deserves further evidence-based research to understand their position. Professional recognition of the sonographer’s role in obstetrics is critical and requires immediate attention.
Limitations and Areas for Further Research
This study was limited to sonographers’ views only, which may give a biased perspective on the current practices within all Australian settings. Future studies should look to include all maternity care stakeholders—in particular, pregnant patients, sonologists, and the professional bodies representing the interests of relevant health professionals in obstetric settings.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.