
Abstract
Trisomy 18 is the second-most common aneuploidy and greatly ranges in presentation. This case study examines the diagnostic procedures taken with an Amish woman’s Trisomy 18 pregnancy. The sonographic findings are examined and compared with typical presentations and cultural differences regarding obstetrical care plans. Current medical advances have altered prognoses and courses of treatment. This case study highlights the importance of patient-provider communication and the need for continuous amendment of information, within obstetrical care.
Trisomy 18, or Edward’s syndrome, is a severe chromosomal disorder caused by the creation of an extra chromosome 18 and occurs in approximately 1 of every 1500 pregnancies. With advanced maternal age is the strongest risk factor, Trisomy 18 is one of the most common aneuploidies only second to Trisomy 21 or Down syndrome. 1 Depending on the phenotype, which includes full, partial, or mosaic, the severity of physical and cognitive anomalies range significantly. 2
The case study patient was a 20-year-old woman residing in an Amish community. This was a first pregnancy, and she reported no pain, vaginal bleeding, cancer diagnoses, or pelvic surgeries. The Amish community and immediate family are a significant factor in how an Amish patient goes about receiving medical intervention. 3 Although the Amish will utilize mainstream medicine in emergent situations, the preferred methods of care are natural remedies and prayer. 3 Pregnancy is normalized within the community and the use of birth control or abortive services are highly impermissible. 3 Barriers such as transportation, finances, and feelings of helplessness and unfamiliarity can interfere with treatment and should be accounted for to the best of the provider’s ability. 3
Case Report
The patient came to a 25-bed critical access hospital for an outpatient sonogram to determine fetal position. 4 However, after visualizing abnormalities in the breech fetus, the sonographer did a complete obstetrical examination using a GE Logiq ultrasound equipment system and a 6-MHz curvilinear probe. Atrioventricular septal defects were evident along with a dilated right lateral ventricle of 2.5 cm, a hypoplastic cerebellum (see Figure 1), and a non-visualized cavum septi pellucidi (CSP) (see Figure 2). Both lower extremities were suspicious for club foot or rocker bottom (see Figure 3) and the fetus was small for gestational age (SGA). A fetal echocardiogram and corresponding sonogram, conducted in the Maternal-Fetal Medicine department, confirmed an absent CSP and a 2.9-cm right lateral ventricle (see Figure 4), along with a Tetralogy of Fallot (see Figure 5). Abdominally, the right kidney was significantly smaller than the left, which had a double renal collecting system (see Figure 6). The biophysical profile was given a score of 8 out of 10, due to absent of fetal tone. These findings were reported as suspicious for Trisomy 21. An ultrasound-guided amniocentesis officially provided the diagnosis of Trisomy 18. A fetal nonstress test was recommended twice weekly until planned inducement around 37-weeks gestational age. The patient planned to deliver at home and to remain with minimal intervention.
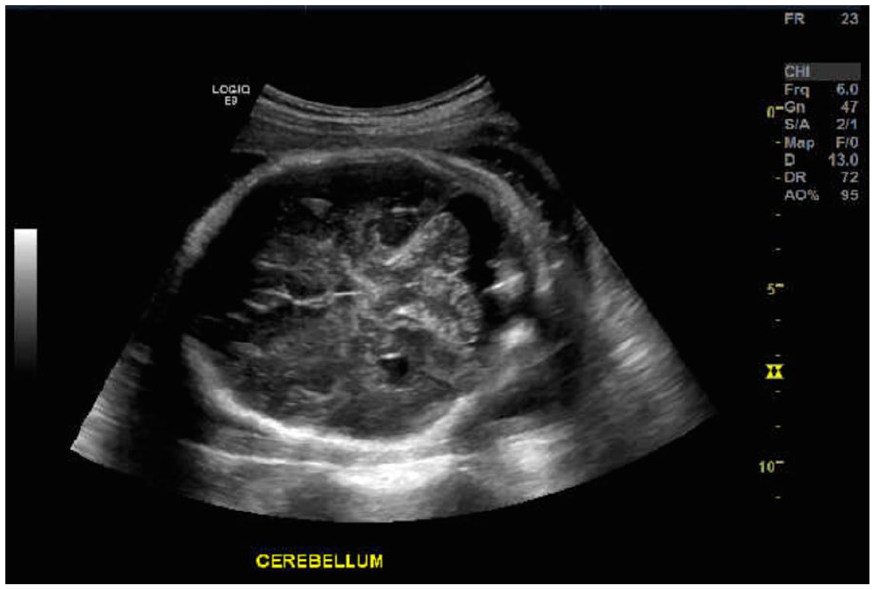
The transverse view of the fetal head which demonstrated a hypoplastic cerebellum.
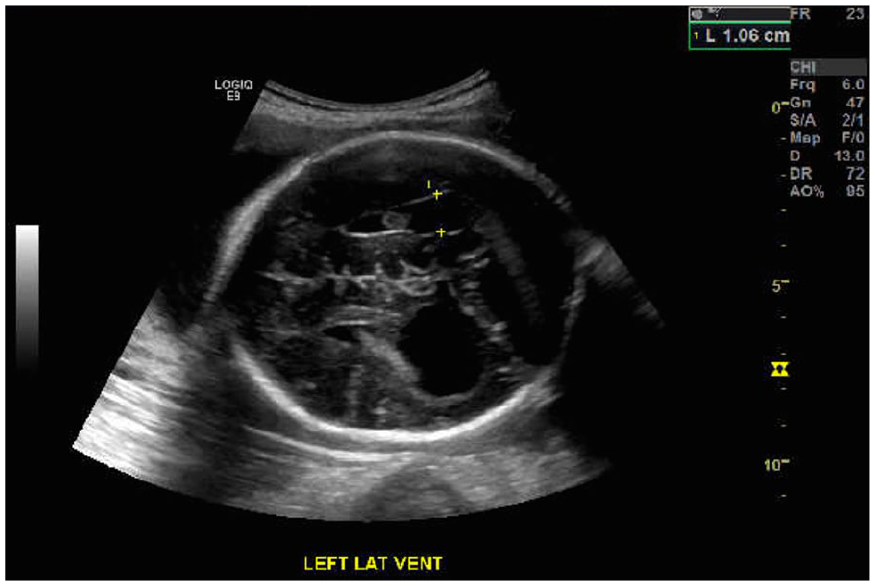
The transverse view of the fetal head, at the level of lateral ventricles, showing an absent CSP.
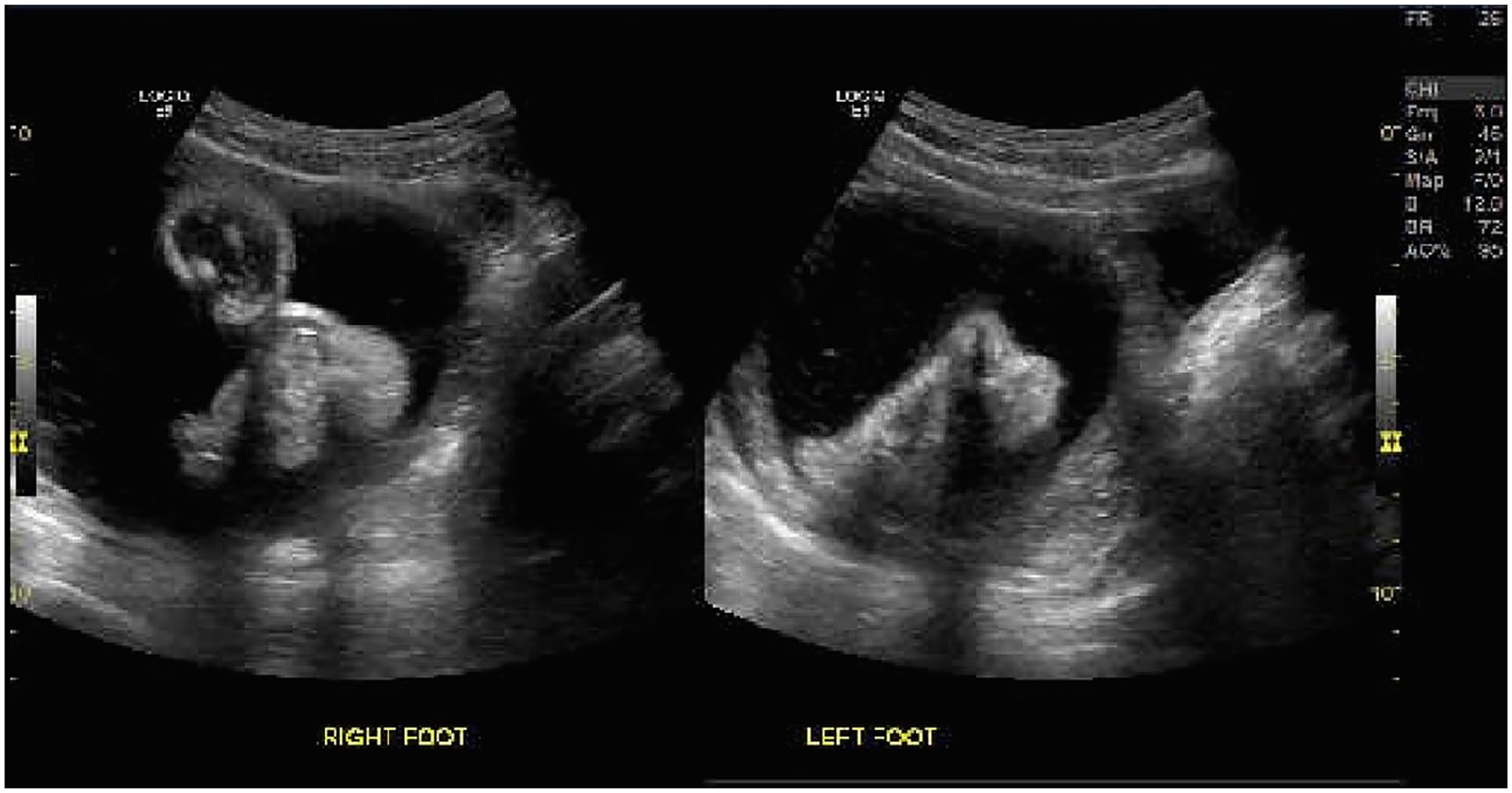
Dual sonographic imaging, which demonstrates views of both fetal feet.
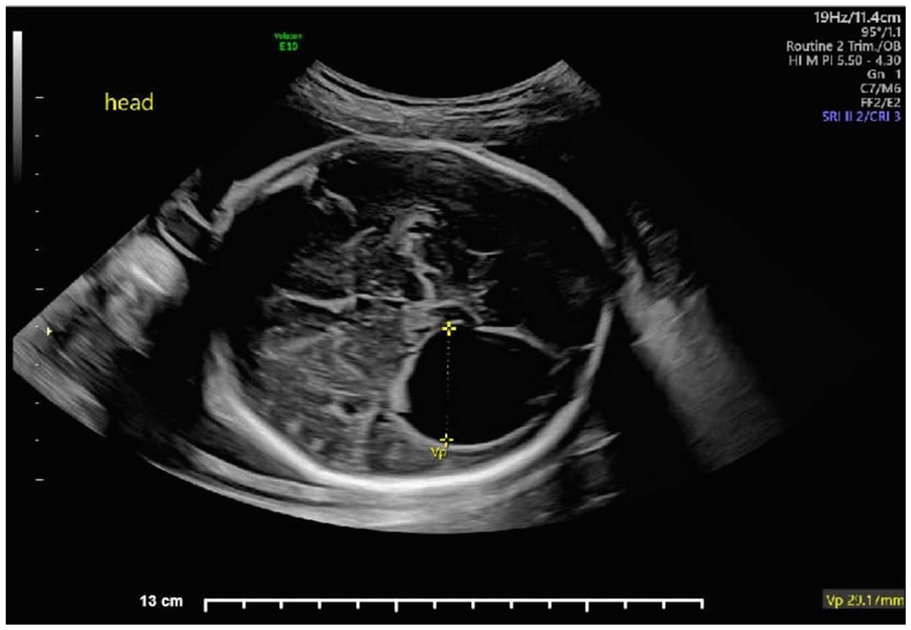
The transverse view of the fetal head, which demonstrated ventriculomegaly of right lateral ventricle.
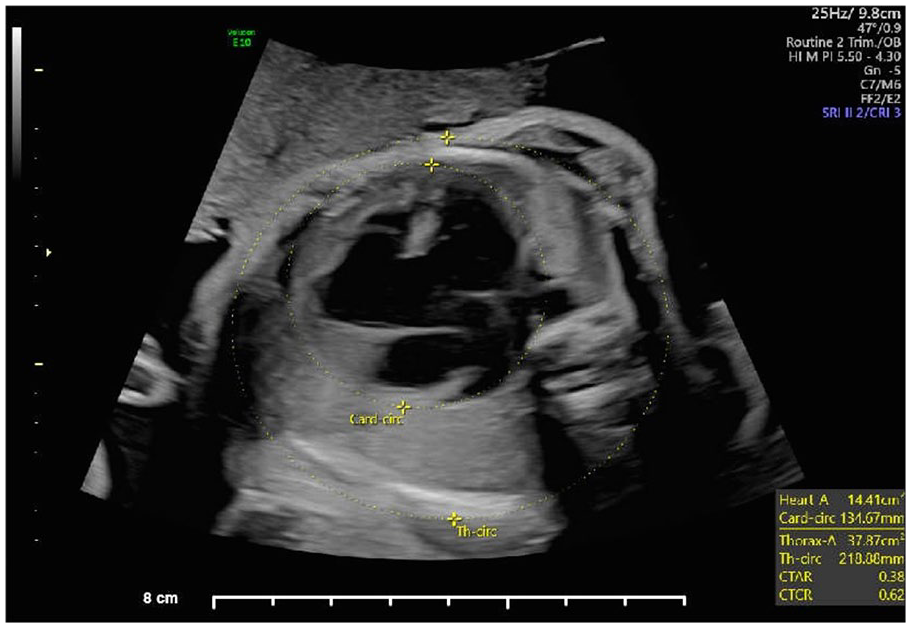
The transverse view of the fetal chest demonstrating an AVSD and overriding aorta.
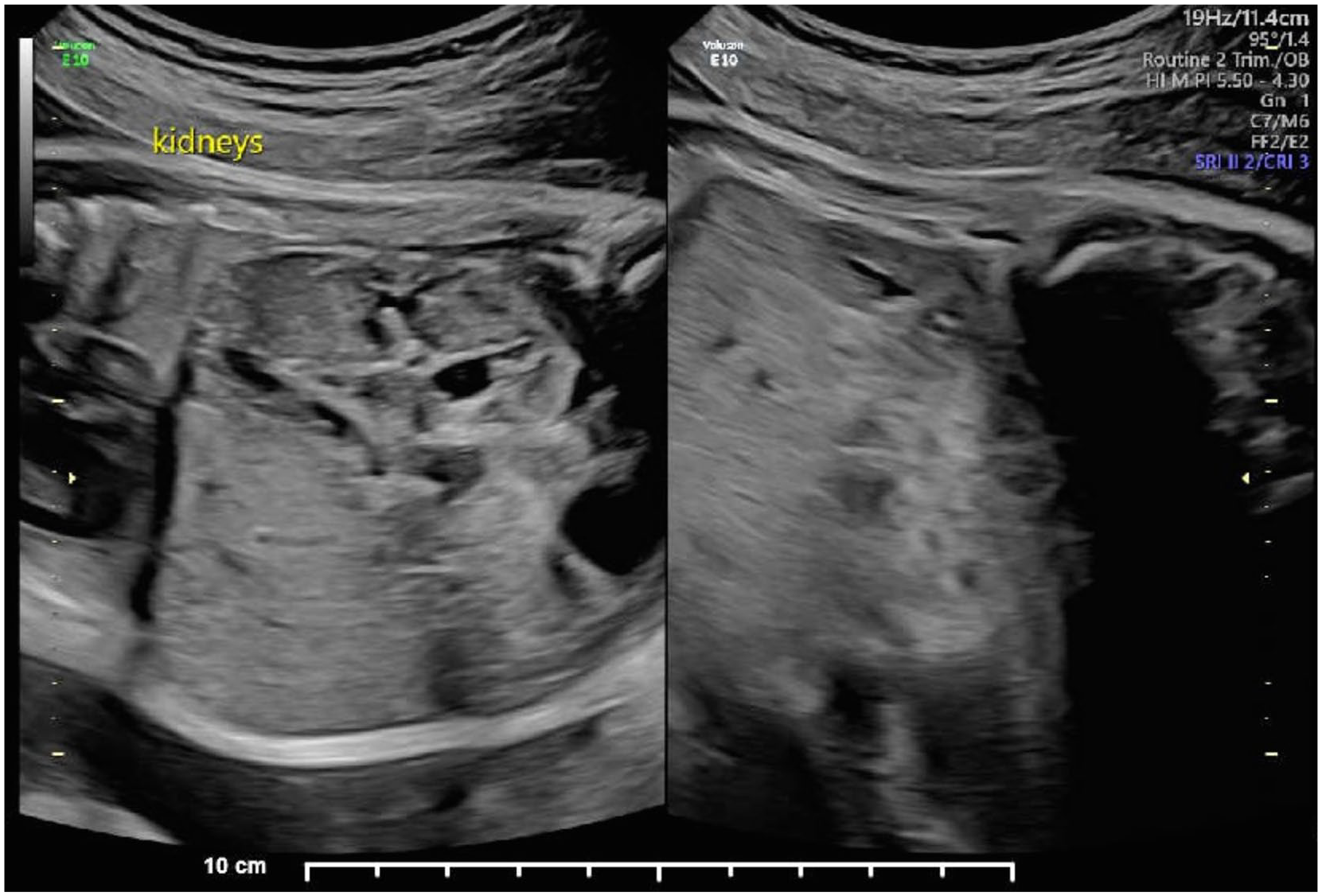
Longitudinal kidneys demonstrating dual collecting system of the left.
Discussion
Trisomy 18 can manifest itself in a variety of anomalies (see Table 1). Studies have demonstrated ventricular septal defects and choroid plexus cysts to be some of the most common findings. However, intrauterine growth restrictions (IUGRs) are also typical and become increasingly significant with pregnancy progression. 5 Gastrointestinal defects can include esophageal atresia, omphaloceles, or hernias. 6 Clinodactyly, single umbilical artery, and polyhydramnios are also associated with this genetic manifestation. Sonography is a valuable tool in the diagnosis of Trisomy 18 with a sensitivity between 70% and 100%. Optimal detection occurs around 20 weeks; however, first trimester exams can determine an early IUGR, with possible abdominal wall or neck defects. 5 A first trimester sonogram can also reveal specific trisomy markers such as an abnormally thickened nuchal translucency, cystic hygromas, or an absent nasal bone. 7 These markers can then be compared with maternal lab work, in the early phases of gestation (see Table 2). 7
Ultrasound Markers for Trisomy 18.
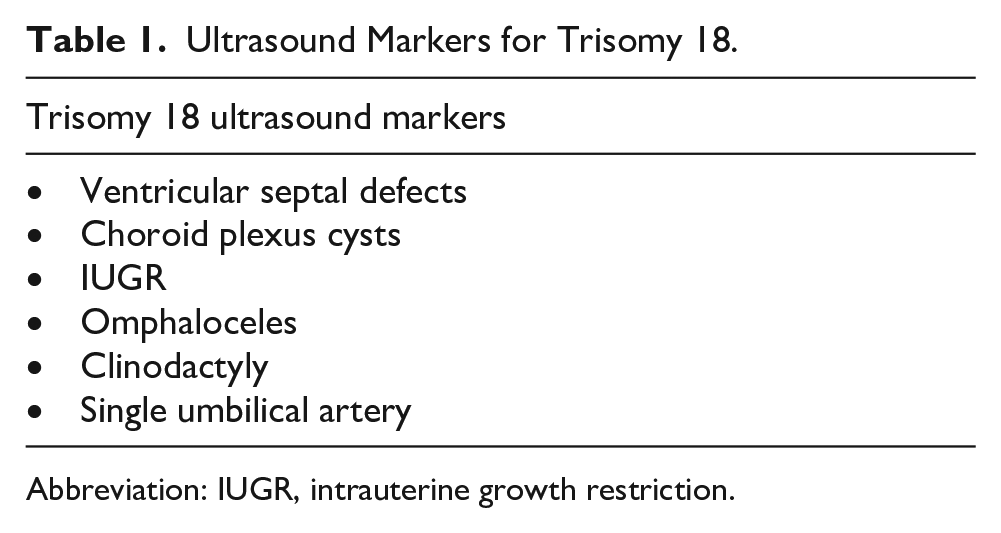
Abbreviation: IUGR, intrauterine growth restriction.
First Trimester Aneuploidy Markers.
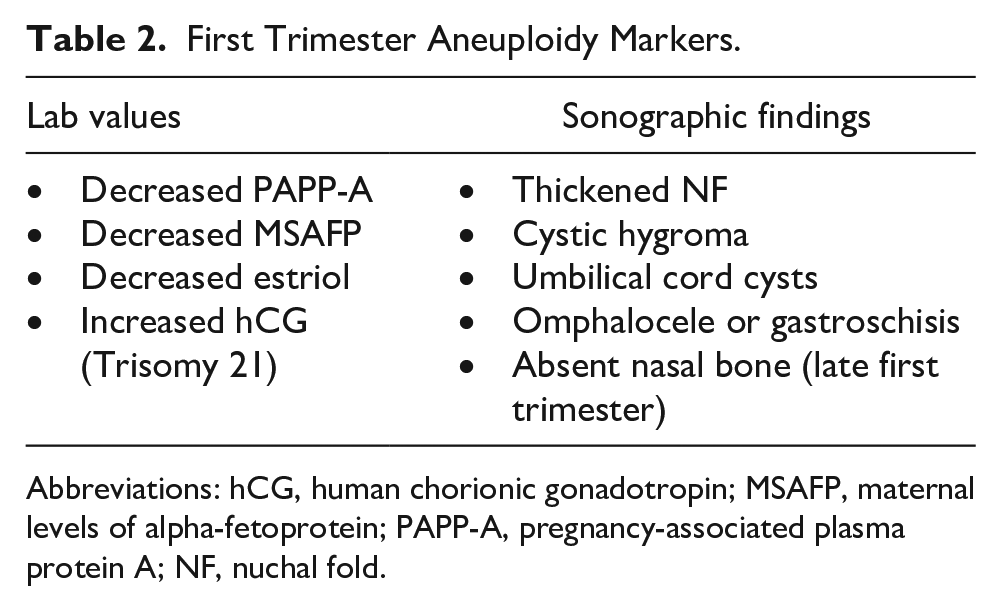
Abbreviations: hCG, human chorionic gonadotropin; MSAFP, maternal levels of alpha-fetoprotein; PAPP-A, pregnancy-associated plasma protein A; NF, nuchal fold.
Noninvasive prenatal testing (NIPT) can be done in early portion of gestation by examining maternal levels of alpha-fetoprotein (MSAFP), human chorionic gonadotropin (hCG), and unconjugated estriol, known as a triple screen. 7 These levels can help to determine the presence of a congenital anomaly and can even help to characterize the specific type (see Table 3). 7 However, alpha-fetoprotein (AFP) is dependent on open neural tube defects and will be increased in the presence of the entity. 7 Quadruple screening adds the evaluation of dimeric inhibin A levels, which can help to better differentiate between Trisomy 21 and 18. 7 Considering the Amish lifestyle, early diagnostic testing may not be utilized as frequently due to financial limitations and the desire to remain with minimal amounts of intervention from modern medicine. 3 Furthermore, early testing may also not be as impactful to the Amish, since the decision to continue carrying the pregnancy would not be affected. 3
Triple Screen Levels and Their Associated Trisomy.
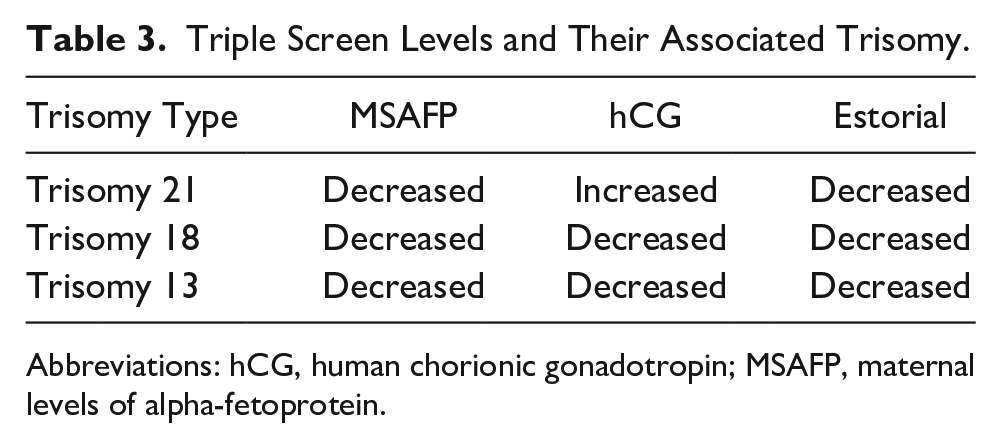
Abbreviations: hCG, human chorionic gonadotropin; MSAFP, maternal levels of alpha-fetoprotein.
With the high sensitivity of sonography and lab indications, it can raise questions of how parents should proceed with an early diagnosis of Trisomy 18. A study of families with Trisomy 18 babies revealed that 43% of them felt their physician pressured them into terminating the pregnancy and 42% felt rushed to make a decision. 1 It is vital that all diagnoses and treatments are clearly explained and that physicians are willing to incorporate and maintain as much of one’s cultural and religious beliefs as possible, in their plan of care. 8 It is also vital that physicians remain updated on medical advances that may improve prognosis. The common prognosis is that Trisomy 18 is “incompatible with life.” However, advancements have allowed surgical intervention to increase survival to years, depending on the severity of the anomalies. A recent study showed individuals can have a 23% survival rate for 5 years and 13% for 10 years with proper medical treatment. 2 Another study revealed cardiac surgery increased the opportunity for home care by improving a 3-year survival rate to 65%. 6 These results are not to diminish the severity of Trisomy 18, but to see the potential that should not be disregarded.
Conclusion
This study was a unique case of a Trisomy 18 diagnosis, within an Amish family. With the various cultures, religious beliefs, and personal preferences the health care system faces, it is challenging to anticipate how a family will receive an aneuploidy diagnosis. Regardless of these factors, families have the right to be fully informed about the given condition. Further studies should be conducted regarding the accessibility and availability of aneuploidy resources to families. While medical advances are important, it is equally vital that families are receiving adequate and relevant information in which they can make an informed decision about how to proceed. With this, Trisomy 18 is a great opportunity to encourage medical advances, accessibility of relevant information, and a safe environment between provider and patient.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The authors have complied with all the sponsoring institutions rules for release of this information.
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).