
Abstract
While originally described in the 18th century, the incidental detection of renal artery aneurysms (RAAs) has increased significantly with the advent and increased usage of modern cross-sectional imaging. Although the incidence remains low, RAAs are clinically important, especially if measuring greater than 2 cm in diameter. Therefore, ultrasonographers and radiologists alike should be aware of its features on multiple imaging modalities as well as imaging pitfalls. Renal duplex sonography is widely used for the evaluation of renal arteries stenosis, fibromuscular dysplasia, renal veins patency, and for the status of renal transplants. RAA is another, albeit rare, indication for renal arteries duplex examination. Furthermore, RAAs may be an incidental finding on abdominal or renal ultrasound. Therefore, familiarity with the sonographic presentation of a RAA is important. Diagnosing RAAs with duplex ultrasound may become exceptionally difficult when the aneurysm has peripheral calcification, even more so when the aneurysm is situated by the renal hilum. Those calcified arterial walls may produce strong acoustic shadowing, mimicking a renal calculus.
A normal renal artery usually measures up to 6 to 7 mm in diameter. In a patient with normal situs, the right renal artery is typically longer than the left and reaches up to 5 cm. The left renal artery is naturally shorter and measures up to 4 cm in length. The renal arteries are typically larger in diameter and length in males when compared to females. 1
Most commonly, a single renal artery supplies blood to each kidney, although there may be unilateral or bilateral duplicated renal arteries and up to 30% of the population, usually with one more dominant than the other. 2 The renal arteries arise from the abdominal aorta below origin of the superior mesenteric artery, generally at the level of the L2 vertebral body. Additional renal arteries usually arise from the abdominal aorta, or in some cases, one of the common iliac arteries. Of note, horseshoe kidneys always have multiple renal arteries. 3
A renal artery aneurysm (RAA) is defined as focal dilatation of the renal artery to at least twice the diameter of the adjacent normal segments. Based on angiographic studies, the incidence of RAA in the general population is 0.3% to 0.7%, typically higher in patients with hypertension. 4 RAAs may be divided into true aneurysms, with all three layers of the arterial wall being intact and false/pseudoaneurysms with at least one focally interrupted layer of the arterial wall. 5 True RAAs are more common in females than males. 6 Most RAAs are saccular and without calcification. 6 According to different authors, 18% to 40% of all RAAs have calcified walls.7,8
True RAAs have increased prevalence among patients with fibromuscular dysplasia, polyarteritis nodosa, Behcet’s disease, mycotic disease, or Ehlers-Danlos syndrome. Pseudoaneurysms are often caused by traumas or iatrogenic causes, such as angioplasty or biopsies. 3 Up to 70% of patients with RAAs have systemic arterial hypertension, many of which are asymptomatic. 8 True RAAs generally affect the trunk of the main renal artery, often near the bifurcation, while pseudoaneurysms of the renal artery are most often seen in the intrarenal arteries. 5
The mean diameter of RAAs is 2.1 cm, although some aneurysms may reach up to 8 cm in diameter. If less than 2 cm, aneurysms are generally followed to assess long-term stability. Aneurysms greater than 2 cm are considered for surgical treatment, including endovascular embolization. Of note, pregnant woman with RAAs have an increased risk of rupture and increased mortality rate. According to Smith and Hinman, 20% of reported RAAs cases were associated with rupture and death. 9
In the last decades, conventional angiography has been commonly used to detect RAAs, however, those aneurysms are increasingly seen incidentally on cross-sectional imaging, such as computed tomography (CT) or magnetic resonance imaging (MRI) as well as CT-angiography (CTA) and MR-angiography (MRA). Although usually not utilized for the detection of RAAs, renal artery duplex sonography (RADS) is an adequate modality for the general assessment of the renal arteries with approximately 75% to 95% accuracy. 10
RAAs with calcified walls may mimic renal stones on ultrasound, particularly if these are in the renal hilum. This may cause misdiagnosis of RAA.
Case Report
A hypertensive female patient with elevated level of cholesterol in her early 60s has had her general abdominal sonogram performed 3 years prior to the current renal arteries duplex sonography examination. A hyperechoic linear structure measuring 1.5 cm was found in her right kidney and reported as a renal stone (see Figure 1).
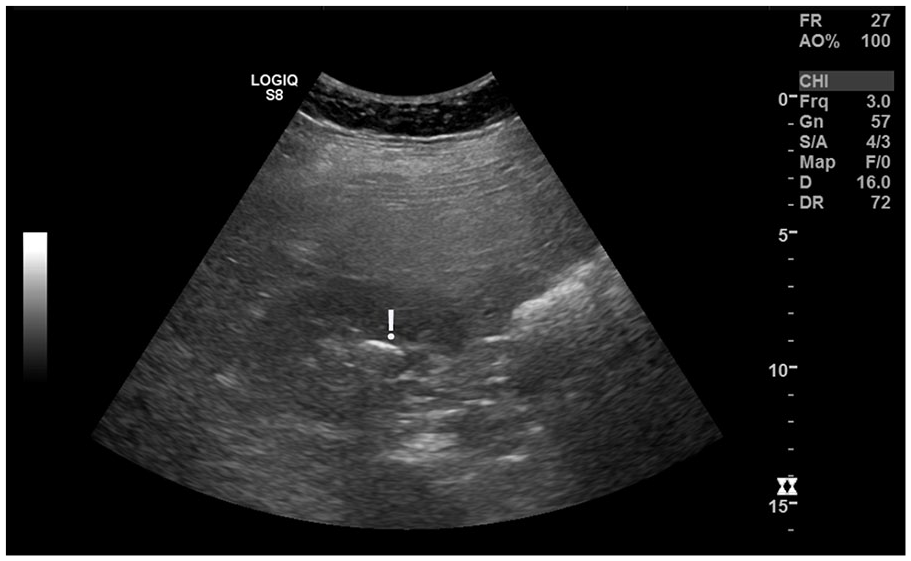
Grayscale Transverse Sonogram of the Right Kidney, as Part of an Abdominal Sonogram, Demonstrates a Linear Hyperechoic Structure (With the <!> above), Which was Interpreted as Renal Stone.
One year after the original abdominal sonogram, the patient had CTA, which was ordered to rule-out fibromuscular dysplasia and renal arteries stenosis because of persistent arterial hypertension and hyperlipidemia. There was neither fibromuscular dysplasia, no hemodynamically significant renal artery stenosis found bilaterally by CTA. However, CTA discovered that the renal “stone” was in fact a right RAA measuring 2.2 × 1.5 × 1.7 cm, with peripheral calcification situated by the renal hilum (see Figures 2–6).

The Axial Image From a Computed Tomographic Angiogram Demonstrates Right Renal Artery Aneurysm with Peripheral Calcification Situated by the Renal Hilum With the <!> Above.
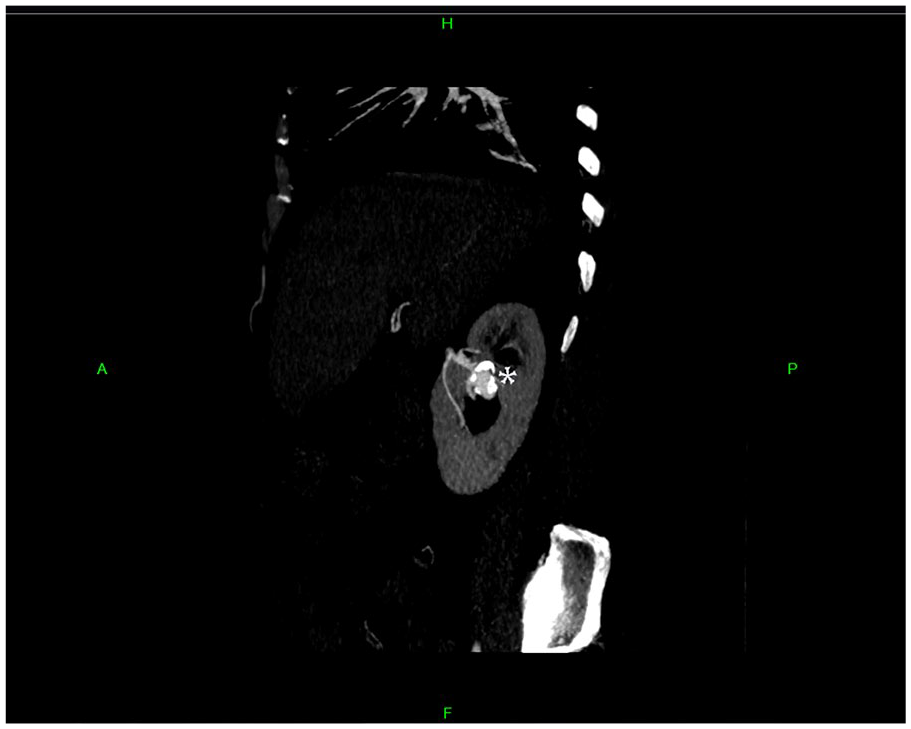
A Sagittal Image From a Computed Tomographic Angiogram Demonstrates a Right Renal Artery Aneurysm of the Proximal Middle Branch of the Right Renal Artery. It is Situated Within the Upper Aspect of the Renal Hilum—Marked With the <*>.
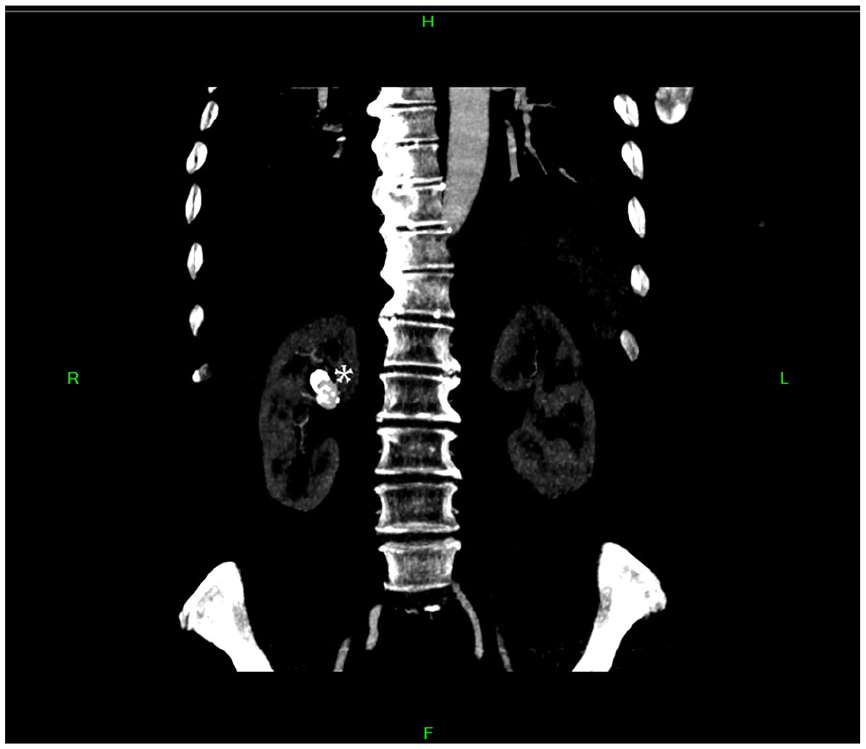
A Coronal Image from a Computed Tomographic Angiogram Demonstrates Right Renal Artery Aneurysm of the Proximal Middle Branch of the Right Renal Artery Situated Within the Upper Aspect of the Renal Hilum—Marked With the <*>.
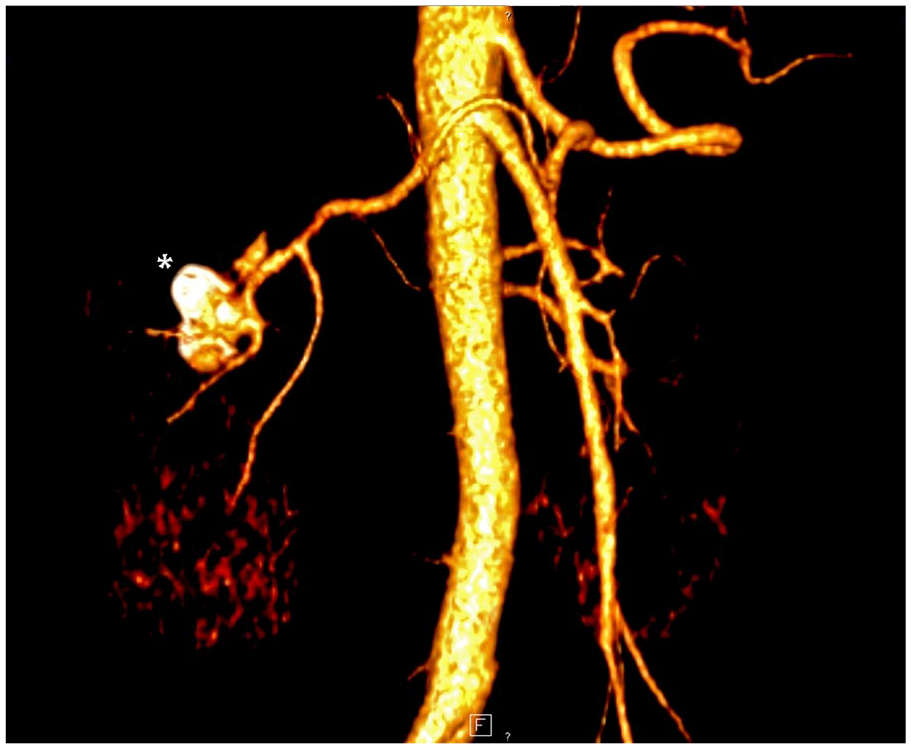
A 3D Reconstruction Image from a Computed Tomographic Angiogram Provides an Oblique View of a Right Renal Artery Aneurysm With Calcified Walls—Marked With the <*>.
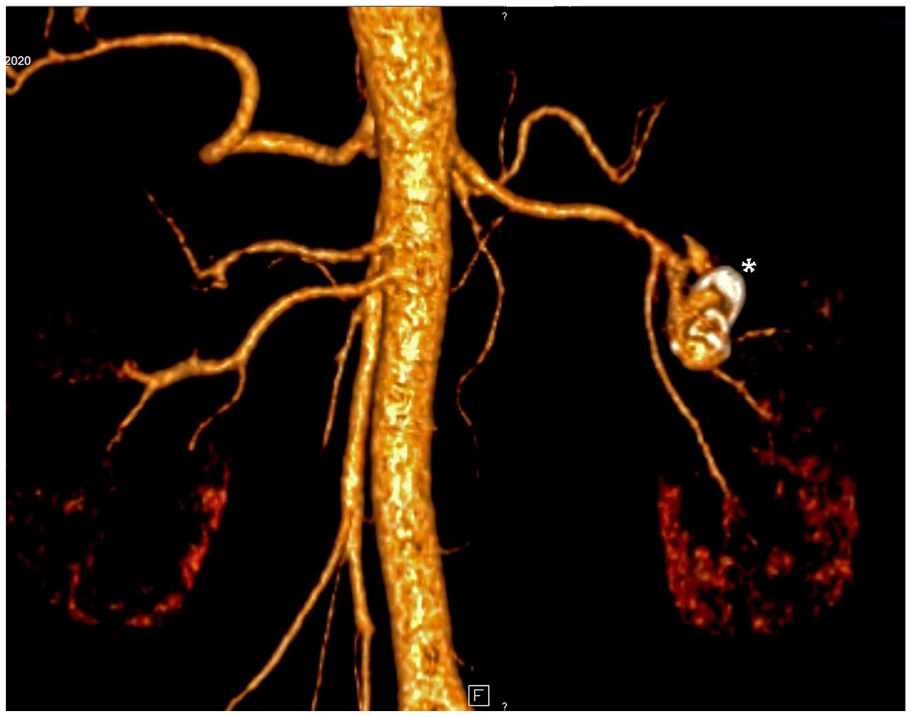
A 3D Reconstruction Image From a Computed Tomographic Angiogram Demonstrates a Posterior Coronal View of a Right Renal Artery Aneurysm With Calcified Walls—Marked With the <*>.
Following prior examinations, the current renal arteries duplex was done using a GE-Logiq S8 scanner (GE Healthcare Ultrasound, Waukesha, Wisconsin) utilizing a curvilinear 4.0-MHz transducer. The protocol included sagittal and transverse scanning of the aorta and both kidneys using grayscale as well as color and spectral Doppler interrogation of the right and left main renal arteries and veins, and bilateral intrarenal segmental arteries.
The hyperechoic structure by the right renal hilum was rediscovered (see Figure 7) with some additional—clarifying oblique views in grayscale (see Figure 8) plus color and spectral Doppler of the aneurysm (see Figures 9 and 10) recorded.
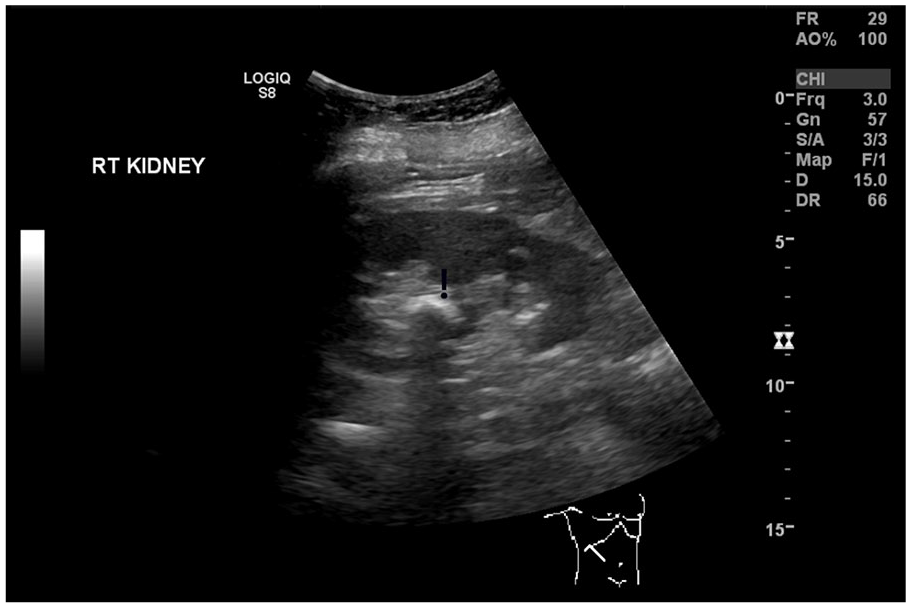
Grayscale Sagittal Image of the Right Kidney (As Part of Renal Duplex) Shows a Curved Hyperechoic Structure (With the <!> Above), Situated By the Renal Hilum, With Noticeable Posterior Acoustic Shadow.
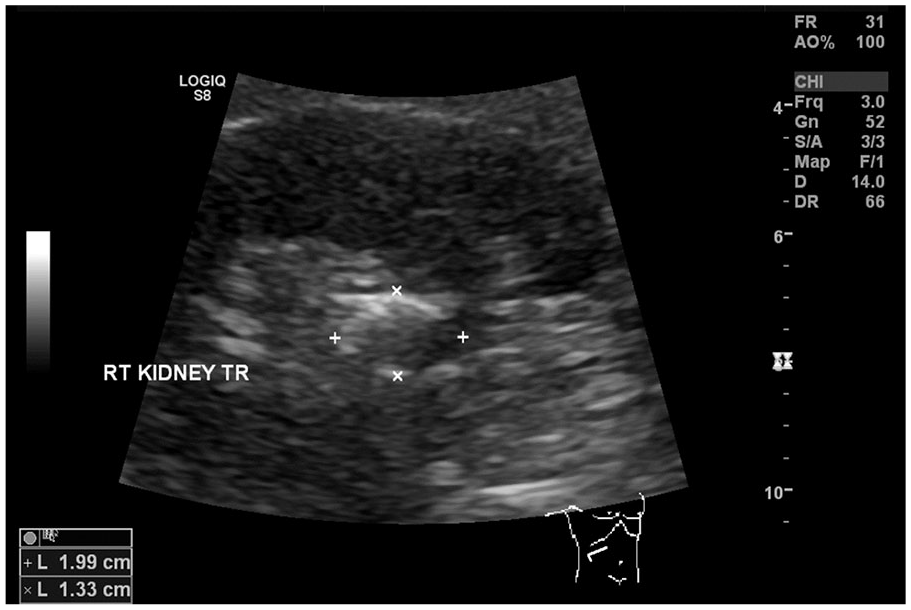
Grayscale Oblique Image of the Right Kidney (As Part of Renal Duplex) Demonstrates the Renal Artery Aneurysm with Partially Calcified Walls Measuring up to 2 cm in the Maximal Dimension.
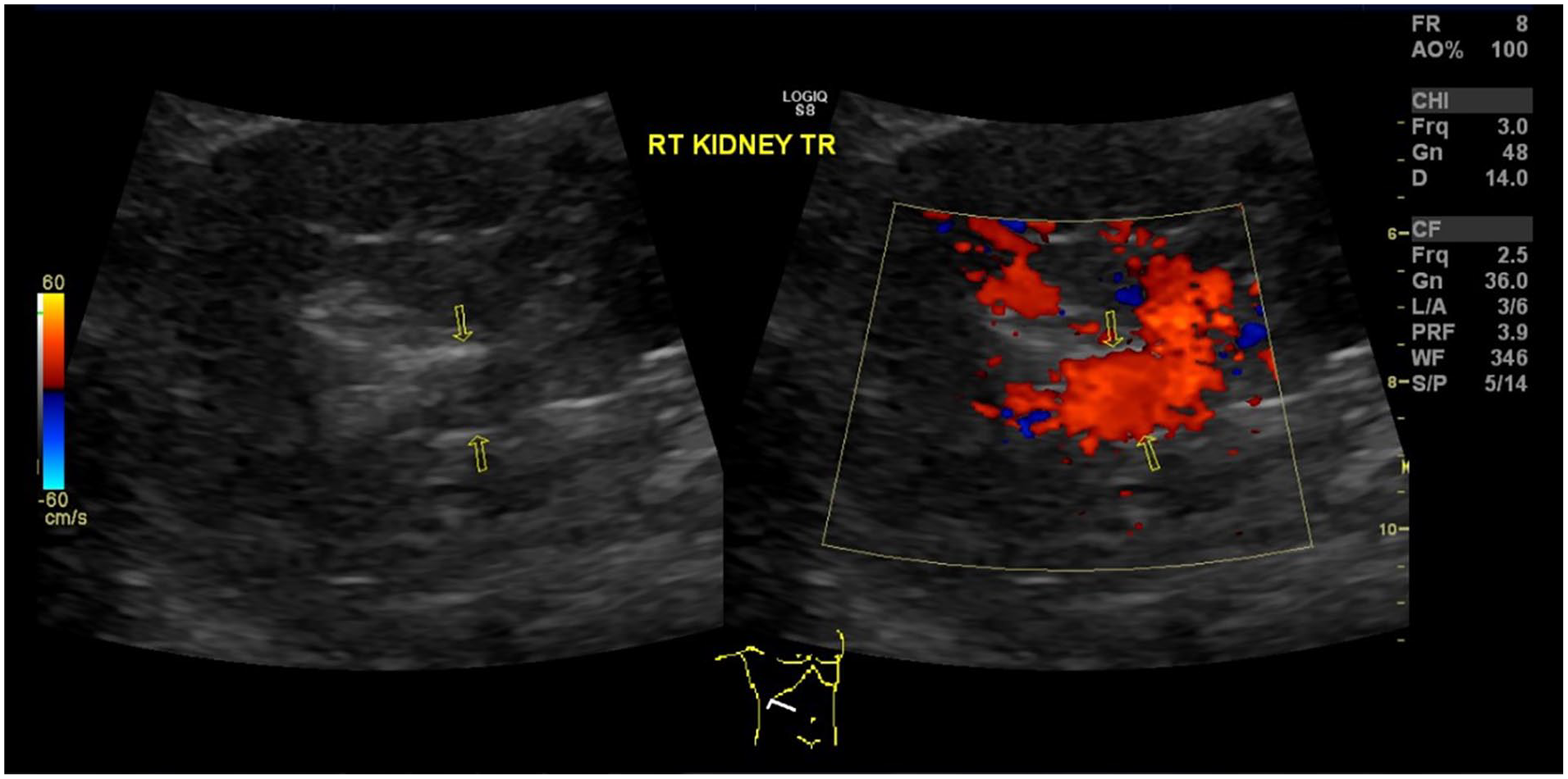
Dual-Screen View of the Right Kidney (Grayscale on the Left and Color Doppler on the Right) Shows Presence of the Renal Artery Aneurysm with Internal Blood Flow.
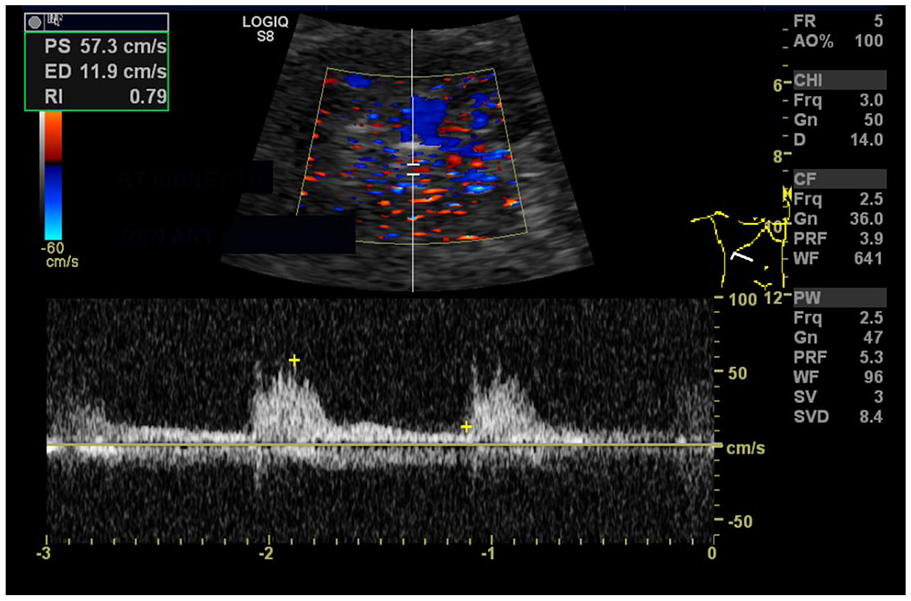
A Spectral Doppler Evaluation, With the Sample Gate Placed Inside the Aneurysm, is Used to Confirm Patency of the Renal Artery Aneurysm.
Discussion
Nebel described the first instance of RAA in 1719 (it was an aneurysm of the left renal artery observed in a young physician). 11 By 1932, there were only 56 reported cases of RAA. 12 Most of RAAs at that time were discovered incidentally during autopsies—after the patients had died from unrelated illnesses or catastrophic traumas. By 1975, with the advance of various radiologic diagnostic modalities, RAA was no longer considered as an exceptionally rare pathology, being detected in live patients by utilizing transfemoral aortograms and arteriograms. 7 One of the studies published in 1983, had shown that in the patients that had dedicated renal angiography for various reasons, including renovascular hypertension, renal tumors and preoperative evaluation of potential kidney donor, the incidence of RAAs was approximately 1%. 8 Most (80%) of those aneurysms were saccular, the rest were fusiform, dissecting and pseudoaneurysms. 8
One of the first cases of partially calcified RAA had been documented in 1901. It was found incidentally on a postmortem examination in a 9-year-old boy who had died after a severe trauma. At that time, the pathologist who described that case had assumed that the boy’s RAA was a consequence of mitral stenosis. 13
In the 1970s, it was presumed that most saccular RAAs were congenital. 7 Decades later, with more data available, current cause of RAAs in pediatric patients includes connective tissue disorders, such as Ehlers-Danlos or Marfan’s syndrome, various arteritides (Takayasu’s, polyarteritis nodosa, or Kawasaki’s disease), tuberous sclerosis, trauma, and infection. 14 In adults, the most common causes of true RAA are fibromuscular dysplasia and atherosclerosis, whereas pseudoaneurysms of renal arteries usually triggered by iatrogenic traumas (medical interventions) and infections.4,5
Currently, catheter-based arteriography is the gold standard for the detection of RAAs, while CTA and MRA are less invasive and more commonly utilized; renal arteries duplex sonography is also useful but less sensitive and specific. 14 Currently, the accepted indications for RAA interventions include a size exciding 2 cm, female patients of childbearing age and ruptured RAAs. 3 The main methods of radical RAAs treatment consist of surgical resection and endovascular repair. 15
In most patients, rupture of RAAs is unlikely. It is unclear whether the presence of RAA calcifications prevents their rupture. 16
RAAs often detected in the sixth decade of life. 17 RAAs affect predominantly females and more than 65% of them have underlying fibromuscular dysplasia. 17
Partially or completely calcified RAA, especially situated by the renal hilum or anywhere inside the kidney, could be easily mistaken for a renal stone on a routine abdominal or renal sonographic examination. Both ultrasonographers and radiologists should be aware of such possibility, especially in older female patients with hypertension and/or known fibromuscular dysplasia. Various oblique views help to obtain better sonographic images of partially calcified RAAs, while color and spectral Doppler modalities confirm aneurysms’ patency or thrombosis.
Conclusion
More than 110 years after RAAs were described as the rarest of all aneurysms in a textbook of medicine (published in 1908), 18 they are still uncommon but maybe encountered incidentally in asymptomatic patients of different age and sex, including children, on routine sonographic examinations of abdomen or renal arteries duplex.
The presented case of calcified RAA illustrates a diagnostic challenge for ultrasonographers because such aneurysm mimics kidney stone on a sonogram, especially when RAA is situated by the renal hilum or inside the kidney. Therefore, differential diagnosis of RAA in patients with nephrolithiasis, especially those that have certain risk factors, such as fibromuscular dysplasia, polyarteritis nodosa, Behcet’s disease, mycotic disease or Ehlers-Danlos syndrome, should be considered.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval was not sought for the present study because the reported examinations on one patient did not constitute research when they were performed.
Informed Consent
Informed consent was not sought for the present study because all case data were deidentified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).