
Abstract
Pentalogy of Cantrell (POC) is a rare syndrome, with an omphalocele and ectopia cordis (EC) being pathognomonic anomalies. In this case report, a 12-week fetus, for nuchal translucency (NT) assessment, displayed a sac protruding through the midline of the fetal abdomen and lower thorax. The fetus’ cardiac activity was detected within the sac. These sonographic appearances are consistent with omphalocele and EC, respectively. A thickened NT and cystic hygroma (CH) were also identified. An important finding was a 1.8 mm maxillary gap (MG), which is a new marker for possible early diagnosis of cleft lip and palate (CLP), in the first trimester. The coexistence of a MG with POC is unique.
Pentalogy of Cantrell (POC) or Cantrell syndrome is a rare congenital syndrome. The prevalence ranges from 1:65 000 to 1:200 000 cases. 1 It consists of 5 fetal anomalies. They are supra-umbilical midline wall defect, a defect of the anterior diaphragm, a diaphragmatic pericardium (a defect of the lower sternum), and several intracardiac defects. 2 However, few patients demonstrate this full spectrum of defects. An ectopia cordis (EC) and omphalocele are pathognomonic anomalies. 3 Pentalogy of Cantrell can be associated with a wide range of other anomalies such as cleft lip and palate (CLP). 4 Cleft lip and palate is usually detected in the second trimester during the fetal anatomy scan. A maxillary gap (MG) is a visible gap of the maxilla, in the midsagittal view of the fetal face (see Figure 1). If a MG exists, it can be appreciated and measured in the same plane for nuchal translucency (NT) measurement, on a 2D sonogram. It has been proposed as a new marker for early diagnosis of CLP. 5 A MG larger than 1.5 mm may indicate a possible CLP as early as 11 to 13 weeks. 5 Here a case is described of a 12-week POC coexisting with a larger MG. This finding has not been reported previously.
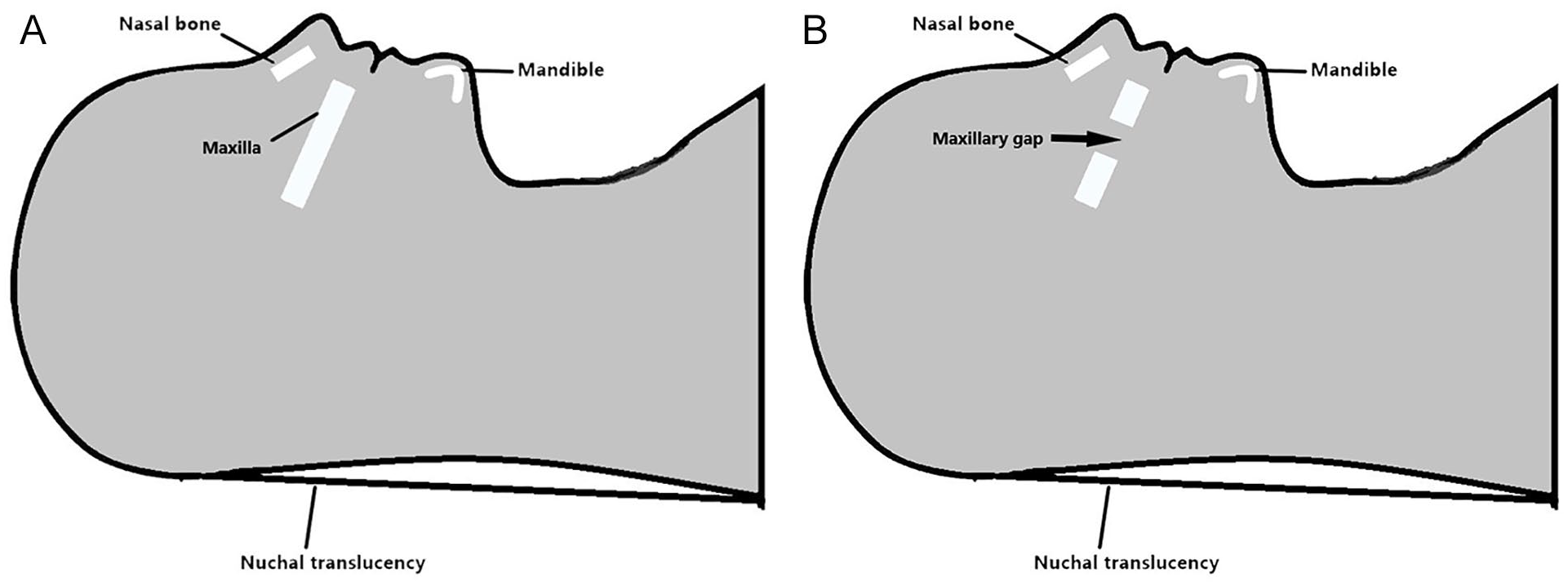
Maxilla and maxillary gap at gestational age of 11 to 13 weeks. Midsagittal view of the fetal faces show a normal maxilla (A) and a maxillary gap (B).
Case Report
A 35-year-old primigravida, with a gestational age of 12 weeks, was referred for NT assessment. The pregnancy was a spontaneous conception. The gestational age had been estimated by a previous dating sonogram. The marriage was nonconsanguineous, neither spouse had a history of congenital malformations or genetic diseases in their respective families. The patient’s previous medical history reported the presence of primary hypertension, but she was on Nifedipine, with good control.
A sonography examination was performed, using a GE Voluson E8 ultrasound equipment system (GE Healthcare, Zipf, Austria), for transabdominal and transvaginal sonography. The measurement of the crown rump length (CRL) was 54 mm and the biparietal diameter (BPD) was 18 mm. These biometry measurements were consistent with the estimated gestational age, based on the dating sonogram. The first abnormality noted was a sac (13 × 15 × 13 mm) protruding in the midline of the fetal abdomen and lower thorax (see Figure 2A). To obtain natural and realistic images, a high definition (HD) live technique was applied. The umbilical cord was found attached in the center of the sac (see Figure 2B). The cardiac activity was detected in the sac with a fetal heart rate (FHR) of 148 bpm, but the heart chambers were only vaguely seen, due to the small gestational age. The hyperechoic and homogenous structure occupying the rest of the sac represented the liver evisceration (see Figure 3). A thickened NT (5.3 mm) and a cystic hygroma (CH) were also detected (see Figure 4). Furthermore, an MG was identified in the midsagittal view of the fetal face by enhancing contrast in gray-scale sonography. The measurement of the gap was 1.8 mm (see Figure 5).
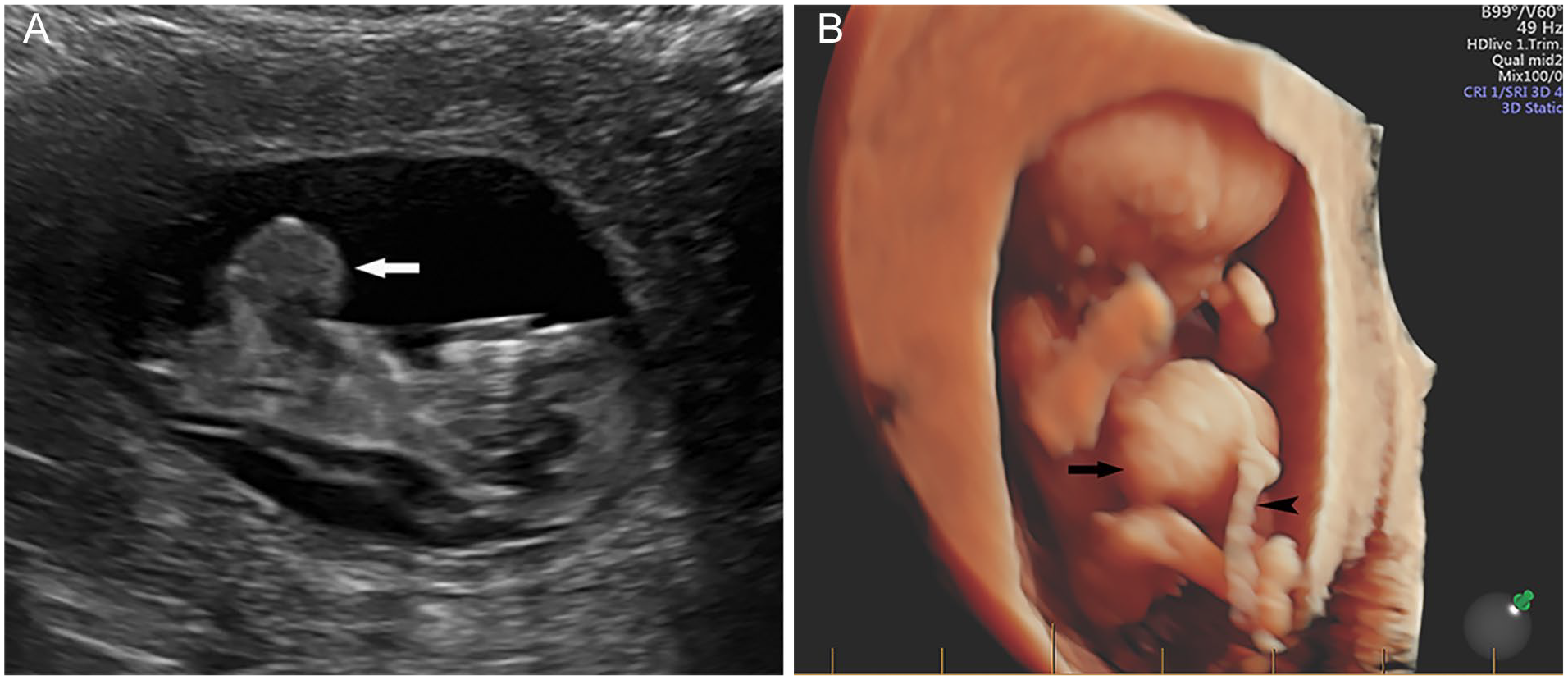
Protruded sac in the midline of the fetal abdomen and lower thorax. (A) 2D gray imaging of the sac (arrow) and (B) High-definition (HD) live showed that the umbilical cord (arrowhead) attached in the center of the sac (arrow).

Contents of the protruded sac are seen on the sonogram. The heart chambers (arrow) and the liver evisceration (arrowheads) are noted.
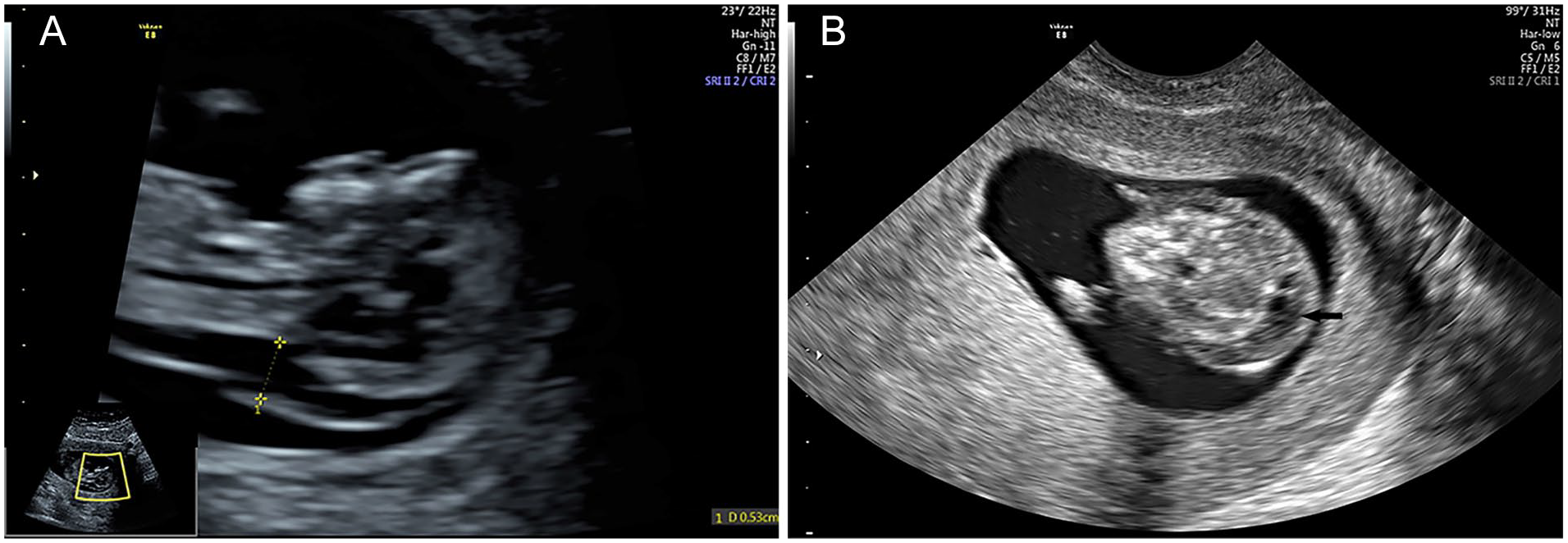
A thickened nuchal translucency (NT) and cystic hygroma are seen on the sonogram. (A) NT (between the calipers) and (B) Cystic hygroma (arrow).
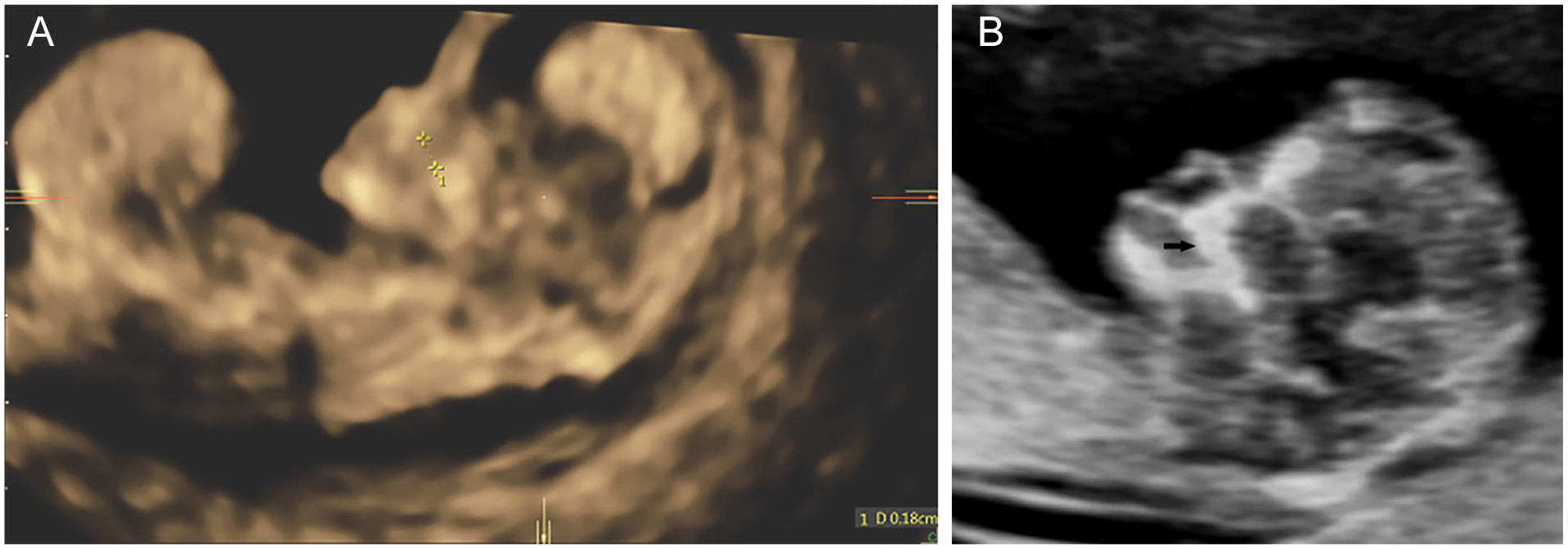
An example of a maxillary gap. (A) The gap (between the calipers) in the midsagittal sonographic view of the fetal faces and (B) Normal maxilla (arrow).
The patient was referred to the obstetrician after the sonographic examination. She opted for surgical termination of pregnancy after counseling of the diagnosis, and prognosis. The products of conception were sent for chromosomal microarray analysis. The result indicated a normal male karyotype.
Discussion
An omphalocele and EC are the pathognomonic anomalies of POC. 3 The current case displays a mass that is enclosed in a membranous sac. It contains abdominal organs and protrudes through the ventral abdominal wall and lower thorax. These sonographic findings are consistent with the diagnosis of omphalocele. Ectopia cordis is defined as partial or complete displacement of the heart outside of the thoracic cavity. 6 In this case, the cardiac activity is detected within the omphalocele, therefore it is EC. Since the current case comprises both omphalocele and EC anomalies, the diagnosis of POC can be established. Comparing with many POC cases, which are detected in the second or third trimesters, this case and associated anomalies were identified at the end of the first trimester, during a systemic sonogram. Therefore, it is worth emphasizing the importance for fetal anatomy assessment in the first trimester. It may provide an opportunity to detect gross fetal abnormalities at the end of the first trimester.
In general, 2D is sufficient to demonstrate the omphalocele, but the application of 3D, 4D, or HD live sonogram is useful for enhancing clinical confidence. It is understood that a 4D sonogram is a combination of 3D with a time axis. It produces images with a live 3D video effect. An HD live is a high-definition live technology that improves the 3D/4D sonographic images. Its images are similar to 4D but are more natural and realistic than those acquired by 4D technology. 7 In this case, the images of the omphalocele and the umbilical cord obtained by HD live technique display clear and detailed surface anatomy of these structures. It is helpful for the diagnosis accuracy. Furthermore, HD live can also be utilized as an essential teaching tool and facilitate the genetic counseling process.
The pathogenesis of POC is not entirely understood. The hypothesis widely accepted is the defective development of the septum transversum (ST). Septum transversum plays an important role in diaphragm formation. It is a mesenchymal layer that develops within the caudal part of the ventral foregut. The myoblasts originating from the ST invade the pleuroperitoneal folds and form the muscular diaphragm. 8 In addition to the defected diaphragm, POC may also result from the developmental failure of the differentiation of the lateral mesoderm between 14 and 18 days after conception. Omphelocele or gastroschisis may occur if the failure results in defect in the midline of the abdomen. 9 In the present case, it can be assumed that the fetal heart descended from the defected ST and protruded together with the visceral organs into the omphalocele, which was caused by the failure of midline fusion.
In recent years, the cause of POC has been explored at the molecular level. The alteration of the Aldehyde Dehydrogenase 1 Family Member A2 (ALDH1A2) gene located on chromosome 15q21.3, whic may play a role in the development of POC. Aldehyde Dehydrogenase 1 Family Member A2 codes for the enzyme retinaldehyde dehydrogenase 2 is a major enzyme involved in early embryonic and cardiac development. 10 The presence of molecularly confirmed Goltz-Gorlin syndrome and POC in a single patient has been reported. This finding highlights that X-linked Porcupine O-Acyltransferase (PORCN) mutation in Goltz-Gorlin, a disorder of meso-ectodermal origin may be a genetic cause of POC. 11 A whole exotic sequencing of 11 families with the diagnosis of POC reveals that Myosin Heavy Chain 10 (Myh10), the encoding gene of Nonmuscle myosin II-B (NM II-B) heavy chains, may be linked to the pathogenesis of POC. 12
Apart from the 5 characterized defects, POC can be associated with various anomalies including exencephaly, large encephalocele scoliosis, spina bifida, intralobar pulmonary sequestration, gallbladder agenesis, polysplenia, cloacal exstrophy, genitourinary anomalies, limb defects, and CH. 13 The CH in the present case is well demonstrated as the extra anomaly in POC. Although strongly associated with abnormal karyotypes, CH can be an isolated finding, which may ameliorate or disappear spontaneously. 14 Cleft lip and palate is another abnormality that has been reported in POC cases. 13 It is a multifactorial congenital defect with relatively high prevalence. In general, the incidence of CLP is about 1 in 600 to 800 newborns and an isolated cleft palate exists roughly in 1 in 2000 live births. 15 However, there are no statistics on CLP in POC cases due to the rarity and heterogeneity of this syndrome. Most CLP cases are detected in the second trimester during the fetal anatomy scan. However, MG as a new marker for possible CLP, has been suggested that it should be larger than 1.5 mm to indicate a possible CLP in the first trimester. 5 A MG less than 1.5 mm is considered a normal finding due to incomplete ossification in some areas of the maxilla. 5 In the current case, the MG is clearly seen with a measurement of 1.8 mm, which suggests a possible CLP. To date, this is the first known case of POC coexisting with a MG. Although the CLP is not possible to be confirmed due to the early gestational age and surgical termination of pregnancy, the diagnostic value of MG should be considered.
The survival rates correlate with the heterogeneity and severity of this syndrome. The prognosis is poor in patients with EC and associated anomalies. In a series of 13 POC cases with EC, the mortality rate was 84.6%, with a mean age at death of 3.6 months. 16 The current case belongs to the category of the above-reported cases. In addition, this case has more associated anomalies. The prognosis might be worse if the early pregnancy termination were not executed.
Conclusion
Ectopia cordis and omphalocele are pathognomonic anomalies of POC. They can be associated with a wide range of other anomalies. The MG, as a new marker for possible CLP, is a new anomaly found coexisting with POC. It not only indicates a possible CLP, but also makes the possible diagnosis earlier in the first trimester.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval was not sought for the present study because only anonymous information was used in this report.
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).