
Abstract
This case series is presented to illustrate the clinical value of identifying, sonographically, the type of cesarean scar ectopic pregnancy that may present, as this has become more frequently encountered. The choice of surgical treatment appears to be dependent on the sonographic typing, of this specific type of ectopic pregnancy. This case study illustrates the importance of this topic, given the rising incidence of cesarean deliveries coupled with the increase in first trimester sonograms being more commonly performed. The value of proper diagnostic detection is important, given the contemporary management of this new type of ectopic pregnancy.
Keywords
The standard of providing first trimester sonography in pregnancy and the rising incidence of cesarean delivery has led to the more commonly recognized cesarean scar pregnancy (CSP). It can occur as the result of implantation of a gestational sac (GS) within a cesarean scar defect or adjacent to it. This represents a new type of ectopic pregnancy (EP), representing 4.2% of all EPs. An ectopic pregnancy occurs in approximately 1% of all pregnancies, 1 and it is known to be associated with significant maternal morbidity (e.g. tubal rupture, hemorrhage, and subsequent infertility). 2 The sonographic recognition of the type of such a cesarean scar defect implantation and its consequential surgical treatment has now led to the accumulation of data regarding the optimal treatment of CSP, according to the classification as to its type. 3 Rather than from case-control studies, much of the current information has resulted from the publication of case series. A type I (CSP-I) is caused by implantation of the GS on a previous cesarean scar with progression toward either the cervico-isthmic space or the uterine cavity. A type II (CSP-II) is caused by deep implantation of the GS into a previous cesarean scar defect with infiltrating growth, into the uterine myometrium, and bulging from the uterine serosal surface. Uterine rupture and severe intrauterine and vaginal bleeding can therefore possibly occur during the first trimester of this pregnancy. When recognized, its treatment can potentially prevent this from occurring. A variety of surgical treatments for this have been described and updated to avoid the predicted risks which can occur.4,5 Surgical treatments may sometimes be necessary, in addition to methotrexate (MTX) administration, which is commonly prescribed for medical management of EP.6,7
Recent clinical experience with cases of CSP has caused the authors to describe the sonographic identification and surgical treatment of this relatively new phenomenon and to share it with other interested specialists.
Case Series
Case Report 1
The patient was a 33-year-old G5P2032 female, with 2 previous cesarean sections done because of a history of an open myomectomy. A hemicolectomy had been previously performed secondary to appendiceal carcinoid. Patient denied any vaginal bleeding or pelvic pain. Quantitative human chorionic gonadotropin (hCG) was 10 818 mIU. A live CSP-Type II (cardiac motion detected) was confirmed via sonography. A robotic resection of the CSP with lysis of adhesions was performed. The patient also received MTX and her postoperative course was uneventful (see Figures 1 and 2).
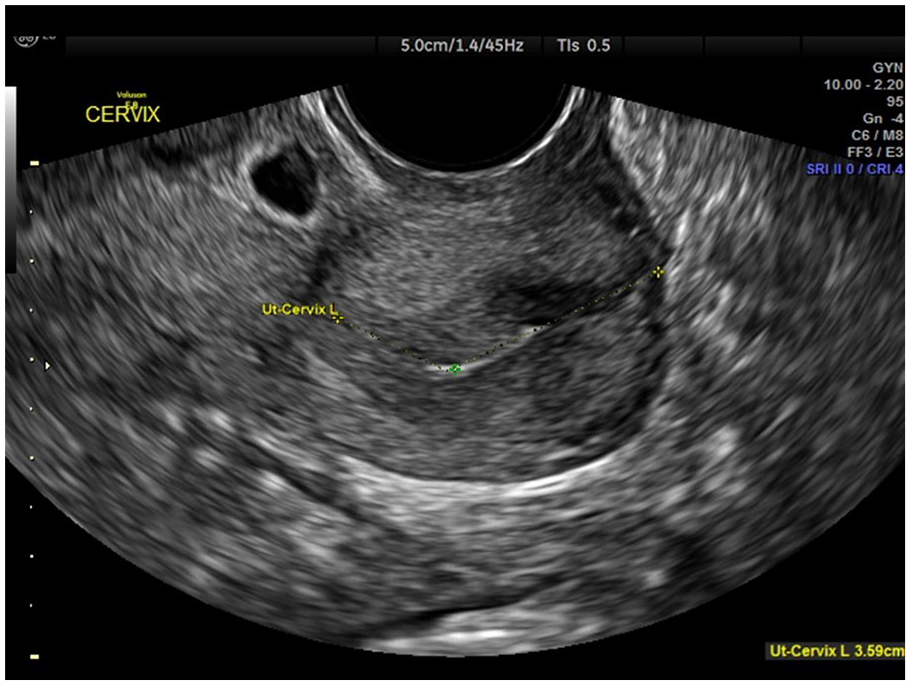
Transvaginal sonography completed in case report 1 that demonstrated a cesarean scar pregnancy with an empty endocervical canal.
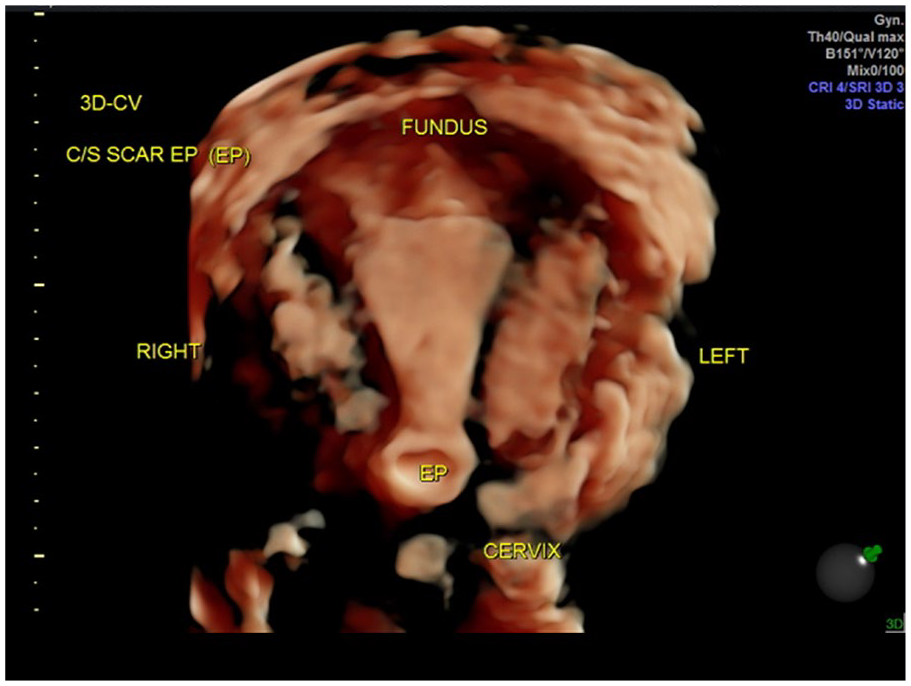
Three-dimensional high-definition live rendering of case report 1 that demonstrated a cesarean scar pregnancy with an empty endometrial cavity and an empty endocervical canal.
Case Report 2
The patient was a 33-year-old G5P3013 female, with a past vaginal delivery and 2 previous cesarean section deliveries, having complaints of vaginal bleeding. A live CSP-Type II (cardiac motion detected) was confirmed via sonography. Laparoscopy with resection of CSP and repair of isthmocele was performed. The patient’s postoperative course was uneventful (see Figures 3–5).
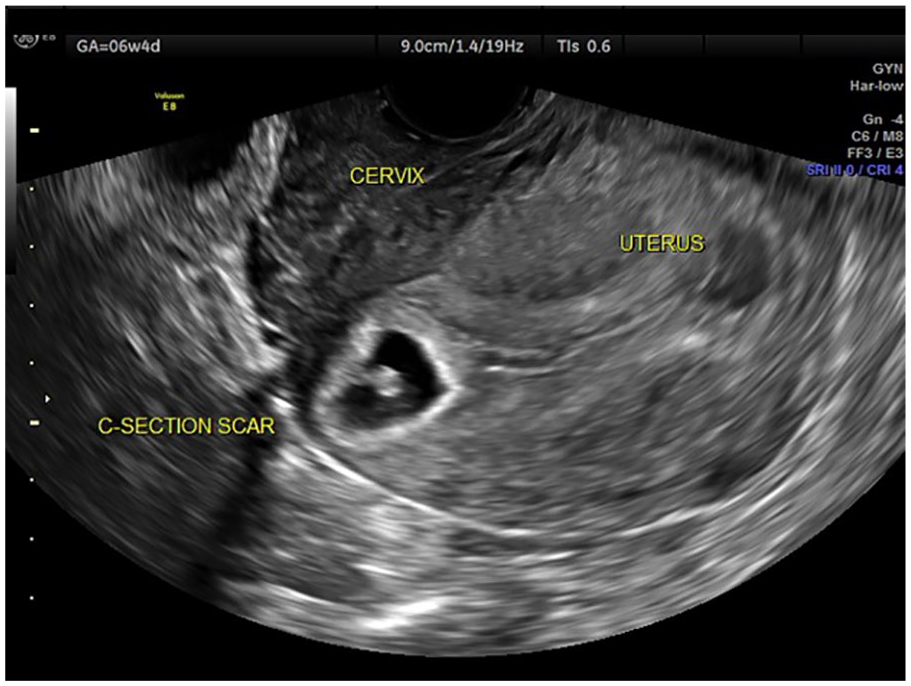
Transvaginal sonography in case report 2 that demonstrated a cesarean scar pregnancy with an empty endometrial cavity and endocervical canal.
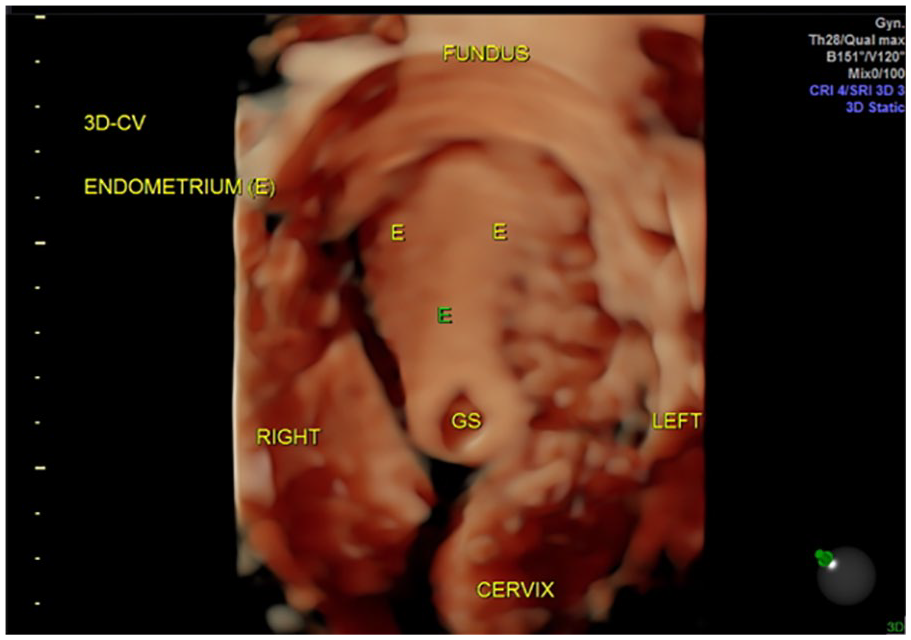
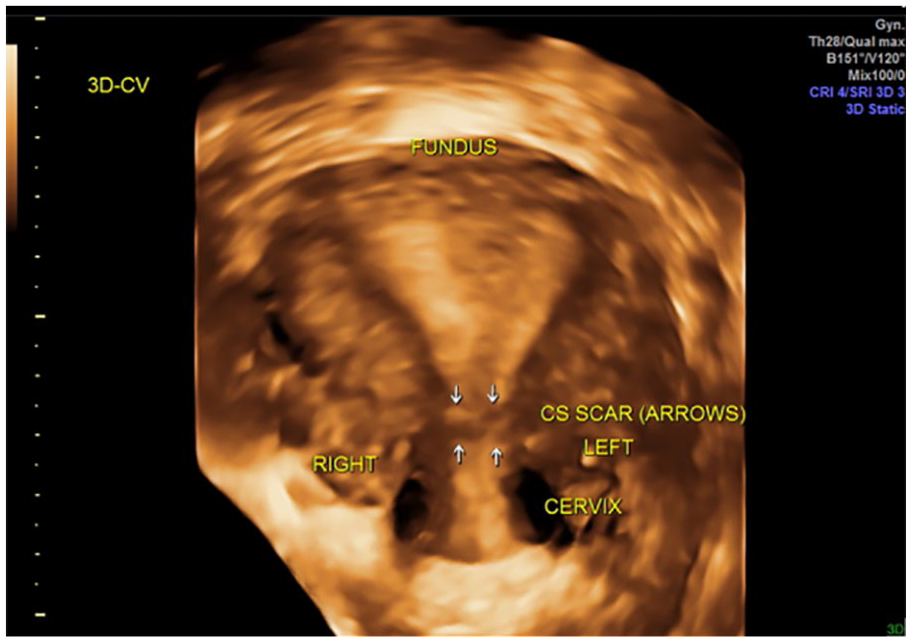
Three-dimensional rendering image in case report 2 that demonstrated a cesarean scar pregnancy with an empty endometrial cavity and endocervical canal.
Three-dimensional image of the uterus in case report 2 that demonstrated a well-healed lower uterine segment with no evidence of isthmocele, 4 months after the removal of cesarean scar pregnancy.
Case Report 3
The patient was a 35-year-old G7P3033 female, with a history of 3 previous cesarean section deliveries. At 9 weeks and 5 days of gestation by last mensural period (LMP), she had complaints of vaginal bleeding but no abdominal pain. She vocalized having a strong desire for fertility preservation. The quantitative hCG was 44 283. A live CSP-Type II (cardiac motion detected) was confirmed sonographically. The patient underwent a laparoscopy with resection of CSP and repair of isthmocele. The patient was not given MTX. Her postoperative course was uneventful (see Figures 6–8).

Sagittal view of the uterus in case report 3, which demonstrated a cesarean scar pregnancy with collection of blood, within the endometrial cavity.
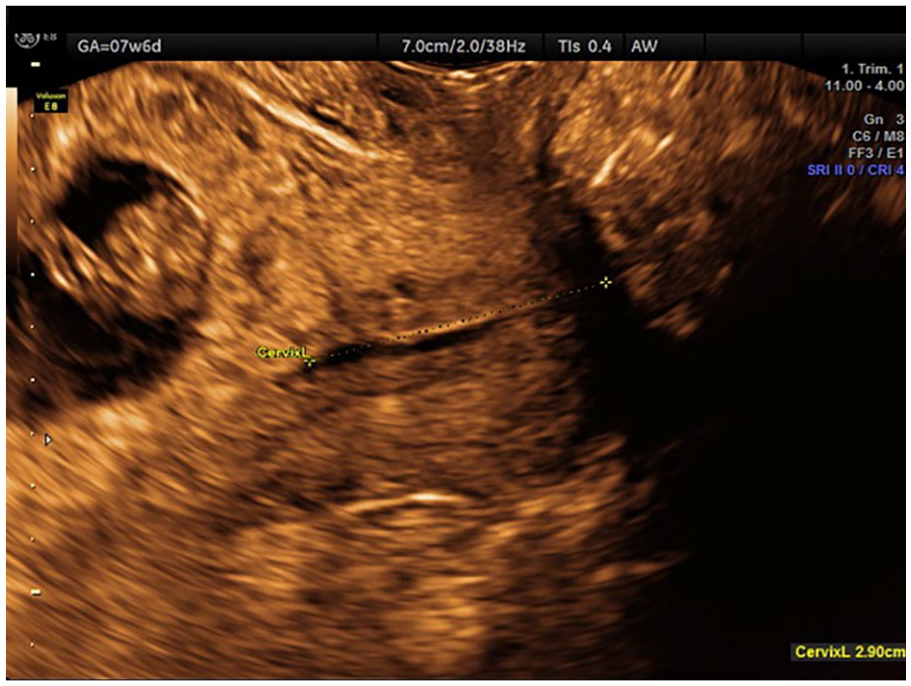
Sagittal view of the cervix in case report 3, which demonstrated a cesarean scar pregnancy, with an empty endocervical canal.
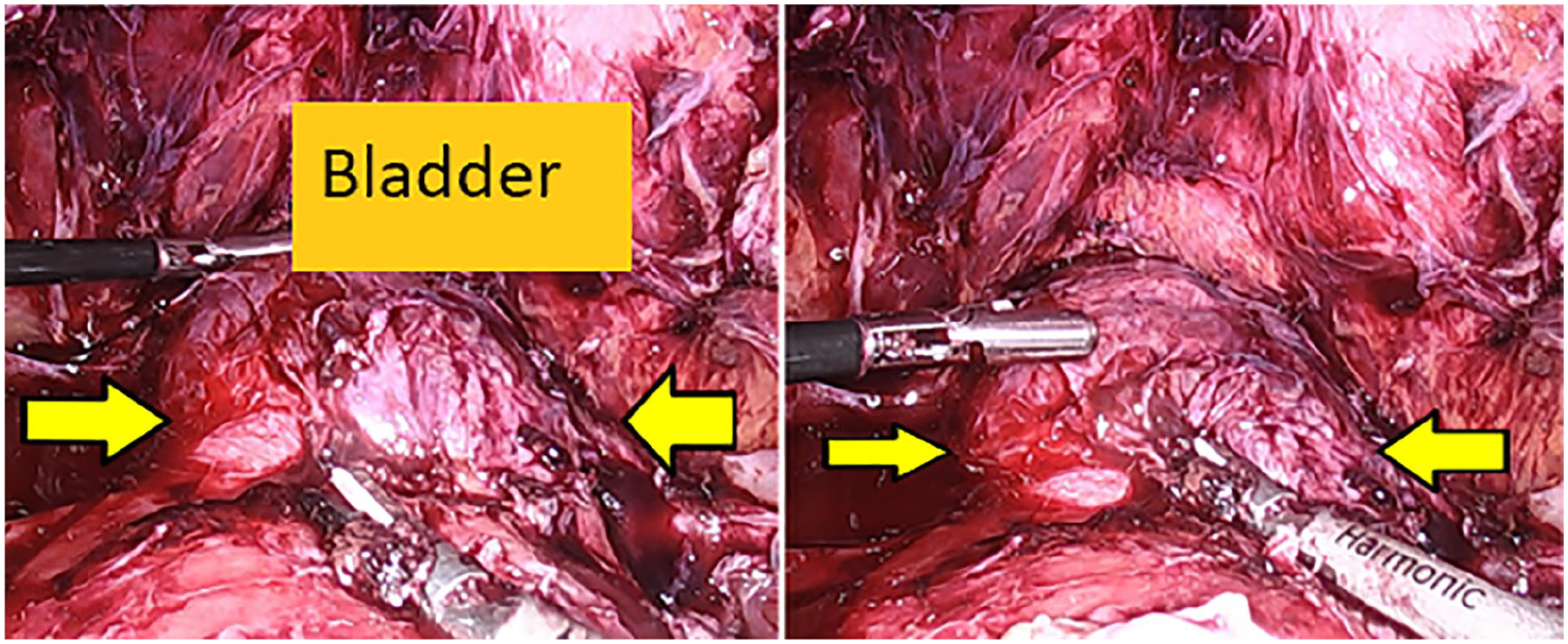
Laparoscopy findings demonstrating a 4 × 4 cm bulging of the cesarean scar pregnancy (seen between the arrows).
Discussion
The epidemic of cesarean deliveries in this country is well-known to practicing obstetrician/gynecologists. This includes its consequence of placenta accreta spectrum (PAS), and now CSP. The sonographic features of the first trimester CSP is less well-known and documented, however, and the treatment dependence of the type of CSP that is identified may be essential for its management. No proper consensus exists as to the ideal management of CSP, though it is well-recognized that transvaginal sonography (TVS) is the best first-line diagnostic tool for CSP.8,9 Its first trimester use for its diagnosis has been encouraged to avoid early hemorrhage associated with the diagnosis. 10 Magnetic resonance imaging (MRI) can be reserved for cases for which there may be a diagnostic uncertainty. The use of color Doppler may enhance its diagnostic acuity. 11 The identification of the type of CSP with first trimester sonography may also be pertinent to patient counseling, as the sort of subsequent surgical treatment may be dependent on the findings. 12 Determining the type of CSP by virtue of recognizing the site of ectopic trophoblast implantation and its relative position with the surrounding tissue is particularly useful in this context. This is especially true when identifying the GS and comparing its position relative to the endometrial cavity and the uterine serosa, if they can be identified. A variety of case series descriptions have been reported in the medical literature, detailing the associated management of CSP.13–15 It appears that the literature continues to evolve on this subject and future reports will likely be forthcoming. The case series presented here represents another practical manner for the identification of the type of CSP (I or II).
Conclusion
When sonography confirms the type of a CSP that is present, its laparoscopic removal may be indicated, which can allow subsequent wound repair to effectively occur when it is encountered. Laparoscopy can become an effective treatment alternative for CSP-II, as is demonstrated by the sonographic and operative expertise of the case series authors.
Footnotes
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.