
Abstract
Penile fracture is a rare urological emergency requiring prompt diagnosis and management. The role of high-resolution ultrasonography is established in detecting a tear, in the tunica albuginea. The late complications of penile fracture are distressing and may manifest as asymmetrical and insufficient penile tumescence, penile ischemia, and sometimes urethral stenosis. The current case series demonstrates the combined role of post-papaverine penile Doppler duplex ultrasonography and sonourethrography techniques in assessing the late presenting cases of penile fractures. The combination of these two techniques was found to be a useful comprehensive imaging tool. This combination can be employed in clinical practice to define the extent of trauma and penile insufficiency, in an efficient manner.
Keywords
Penile injuries are relatively uncommon and are usually related to sexual activity with the injury occurring due to application of axial forces on an erect penis. 1 The injury manifests as acute loss of penile tumescence and sometimes bleeding from urethra. The diagnosis is clinical and is based on patient’s history and physical examination; however, the chronic cases manifesting with impotence and painful erection require sonographic and Doppler evaluation.
Sonourethrography (SUG) is a method which is commonly employed to diagnose anterior urethral strictures, length of the stricture, and degree of spongiofibrosis.2–7 This technique can be employed effectively in cases of penile trauma for the evaluation of urethral tear and its complications such as mural hematoma, fibrosis, or stricture. In the current case series, the radiologist’s experience of combining SUG and penile Doppler technique, in three cases of penile fractures, presenting in their late stages, is shared.
Imaging Methodology
All patient cases were completed with high-resolution ultrasonography (HRUS) of the penis, by the same radiologist. The examinations were all conducted using an Acuson S2000 diagnostic ultrasound system (Siemens Healthcare, Erlangen, Germany) with linear array high-frequency transducer (5–14 MHz). It was done before SUG and post-papaverine penile Doppler duplex ultrasonography (PPDU), where a slow sweep was made through the dorsal surface of the penile shaft. The examination was performed in both transverse and longitudinal planes beginning from the level of the glans and moving toward the base of the penis. The corporal anatomy and any distortion were identified. Preinjection spectral Doppler of the cavernosal arteries was recorded as baseline data.
After taking informed consent and under strict aseptic conditions, anesthetic gel (2% lignocaine hydrochloride) was applied to the external urethral orifice and gel was instilled slowly. The adequate distention was monitored under sonographic guidance. Then the tip of the penis was occluded manually to prevent outflow of the gel and to maintain urethral distention. High-resolution ultrasonography was done to visualize the urethral mucosa and echotexture of the corpora cavernosa.
This was followed by PPDU using intra-cavernosal injection of 60 mg (2 ml) papaverine with 30G needle in one of the corpus cavernosum under ultrasound guidance. Postinjection spectral waveforms were recorded for 30 minutes at every 5 minutes interval.
Because the cases were performed based on the patient’s and urologist’s decision rather than forming part of a clinical trial, they were not subjected to Declaration of Helsinki and ethical approval was not necessary. Informed written consent was taken from each patient.
Cases Reports
The protocol was applied in all three cases of penile trauma which came to the radiology department for penile Doppler study with complaints of inadequate penile tumescence, abnormal penile curvature, and penile insufficiency.
Case 1
A patient of 40 years of age was advised penile Doppler for complaint of asymmetrical and inadequate penile tumescence. There was history of fall followed by bleeding from urethra. Penile bandaging was done and the symptoms relieved without any surgical intervention.
High-resolution ultrasonography of the penis showed ill-defined hyperechoic area representing old hematoma in right corpus cavernosum with focal anterior bulge and discontinuity in the tunica albuginea (Figure 1A). This was followed by SUG which confirmed the findings and provided better anatomical delineation of the lesion and its extent. In addition to it, the SUG showed the site of focal thinning in the urethral mucosa which was sealed by the intracavernosal hematoma (Figure 1B).
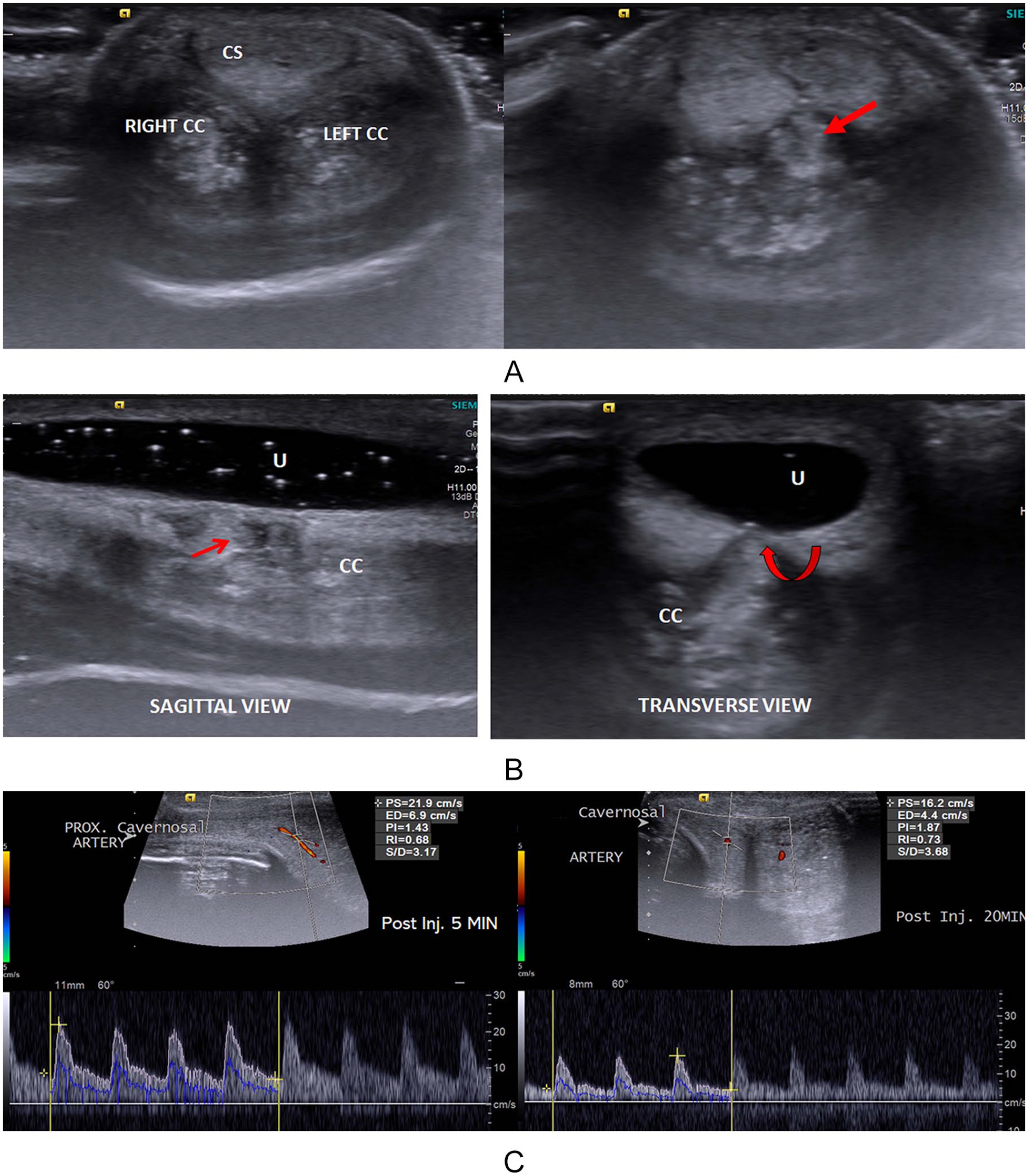
(A) Transverse sonogram of the penile shaft showing echogenic hematoma in both corpora cavernosa (CC) (right more than left) with extension toward the corpus spongiosum (CS) (red arrow). (B) Sagittal and transverse sonourethrography (SUG) images showing focal anterior bulge of the cavernosal hematoma (straight and curved red arrows) with thinning of the urethral (U) mucosa. (C) Post-papaverine penile Doppler duplex ultrasonography images at 5- and 20-minute postinjection phase showing low peak velocity flow and the persistence of the diastolic flow indicating borderline arterial and venous insufficiency.
Post-papaverine penile Doppler duplex ultrasonography was performed which lead to asymmetrical penile tumescence with rigidity in the proximal penile shaft. Cavernosal arteries showed caliber and flow augmentation with maximum peak systolic velocity (PSV) reaching 16.2 cm/s after 20 minutes of injection (Figure 1C). There was no incidence of diastolic flow reversal during the Doppler study with persistent end-diastolic flow of 4 to 6 cm/s. There features were suggestive of borderline arterial insufficiency and primary venous insufficiency due to cavernosal injury and hematoma formation.
Case 2
A young male patient of 25 years of age presented with abnormal penile curvature during erection. There was history of sudden pain and click sound during sexual intercourse 3 months back without any urethral bleed. Pain subsided in few days which later followed by asymmetrical penile tumescence.
High-resolution ultrasonography of the penile shaft revealed small heteroechoic area in the intercavernosal region, more on left side with inconclusive diagnosis (Figure 2A). Subsequent SUG helped in localization of the penile fracture with clear visualization in the tear in tunica albuginea and small focal hematoma in the medial aspect of left corpus cavernosum (Figure 2B). Urethral mucosal outline was maintained.
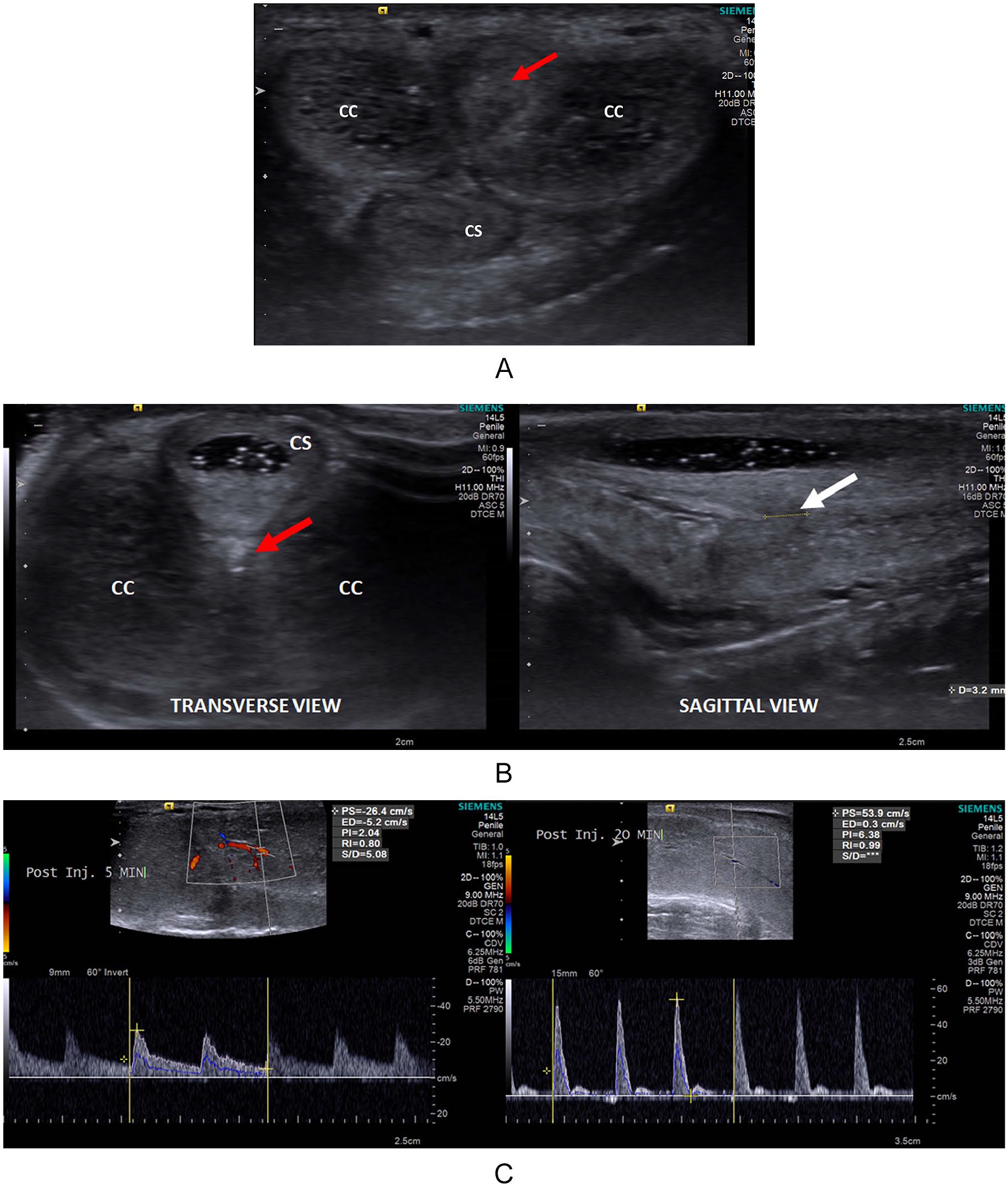
(A) Transverse sonogram of the penile shaft showing heteroechoic area in the inter-cavernosal region (red arrow). (B) Transverse and sagittal SUG images showing a small heteroechoic area (red arrow) with small tear in the tunica albuginea (white arrow). (C) PPDU images at 5- and 20-minute postinjection showing normal peak systolic velocity with diastolic notch suggesting normal color flow. CC, corpora cavernosa; CS, corpus spongiosum; PPDU, post-papaverine penile Doppler duplex ultrasonography; SUG, sonourethrography.
Post-papaverine penile Doppler duplex ultrasonography revealed normal spectral Doppler pattern in cavernosal arteries with preinjection PSV of 12 cm/s and 15 minutes postinjection PSV of 31.6 cm/s associated with early diastolic reversal excluding vascular insufficiency (Figure 2C).
Case 3
A 30-year-old male presented with occasional episode of painful penile tumescence and micturition. There was a previous history of pelvic trauma with bleeding per urethra 6 months back. Combination of the HRUS and SUG revealed small corporal hematoma and urethral spongiofibrosis leading to partial urethral stricture (Figure 3A and B). Post-papaverine penile Doppler duplex ultrasonography was found within normal limits.
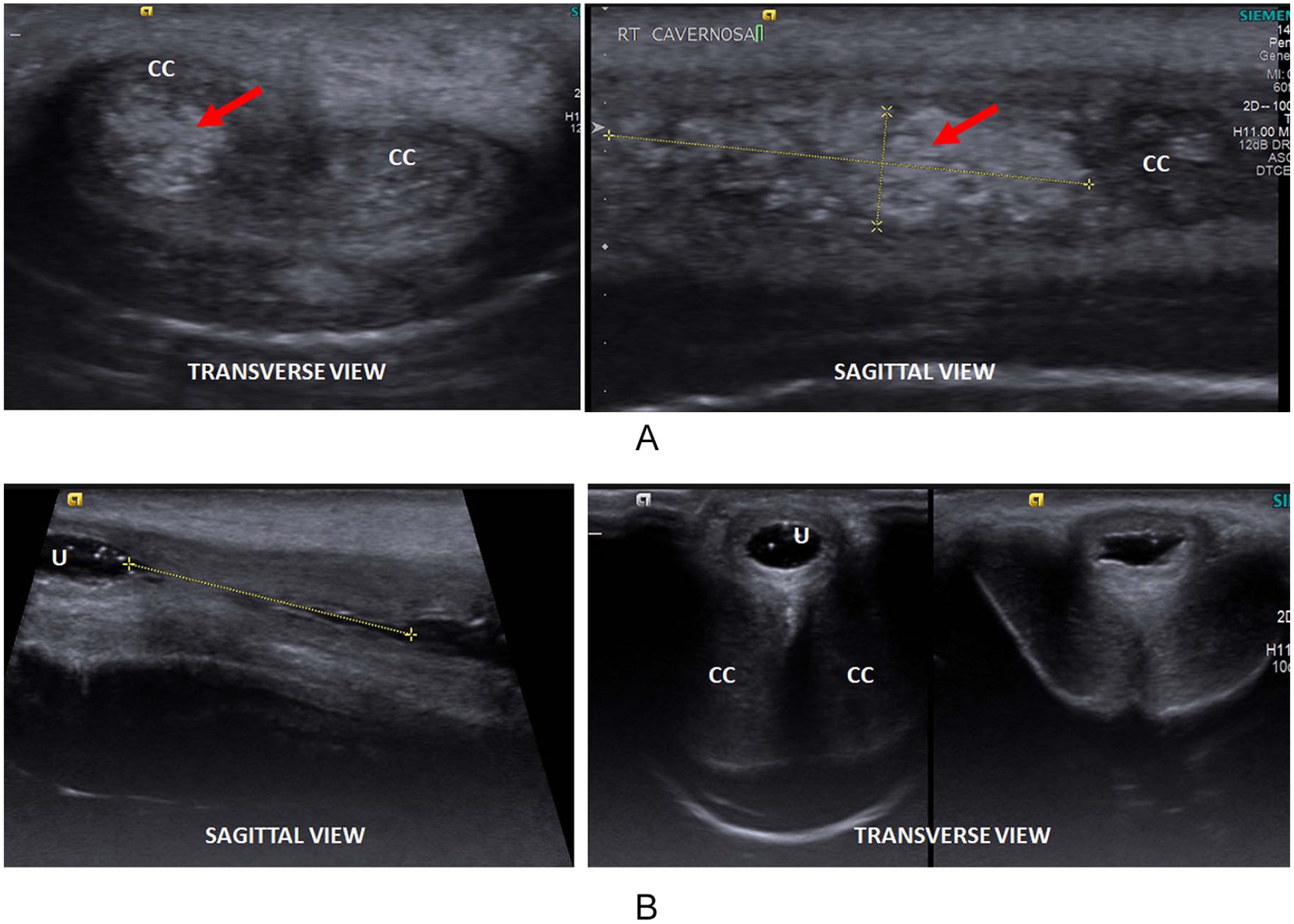
(A) Transverse and sagittal HRUS images of penile shaft showing echogenic area in right corpora cavernosa indicating hematoma (red arrow). (B) Sagittal and transverse SUG images showing irregular outline of the urethral (U) mucosa with narrow lumen suggesting spongiofibrosis. CC, corpora cavernosa; HRUS, high-resolution ultrasonography; SUG, sonourethrography.
Discussion
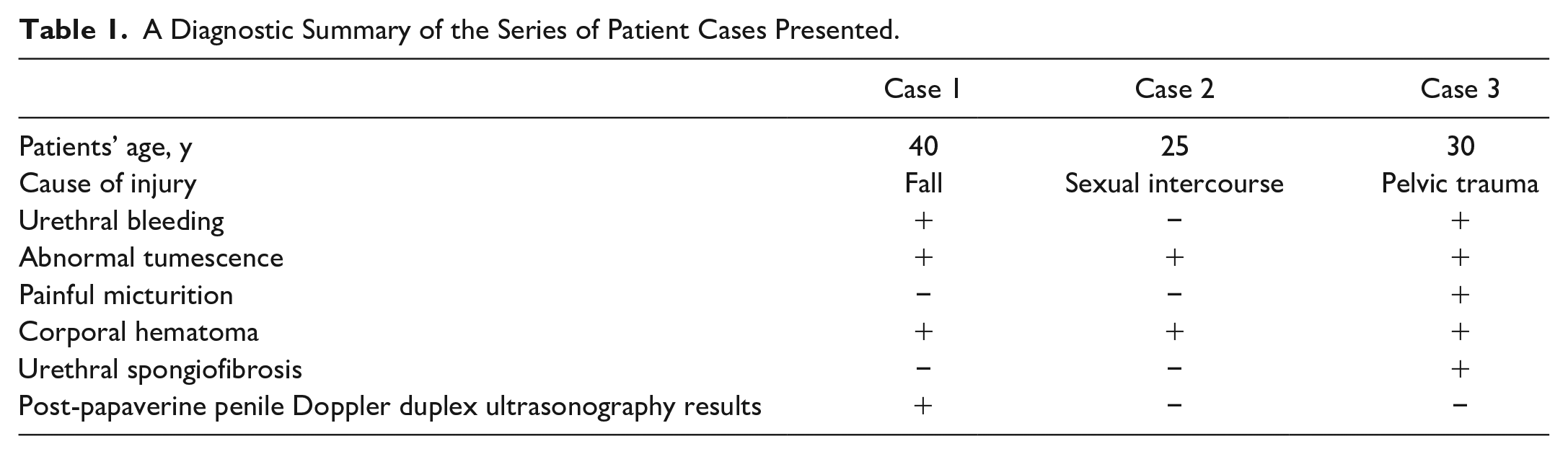
This case series reported on three patients presenting with late complications after penile injuries. Table 1 summarizes the cases. The etiology was direct injury to penis after pelvic trauma in two cases while secondary to sexual intercourse in a single patient case. There was pain and abnormal penile tumescence in all cases with absence of bleeding in only one. This may be attributed to the intact mucosal outline in Case 2. Painful micturition was seen in only one of the cases due to partial urethral stricture. Both HRUS and SUG were able to detect the abnormality in all the three cases. Post-papaverine penile Doppler duplex ultrasonography further added to the diagnostic information in terms of any potential vascular insufficiency.
A Diagnostic Summary of the Series of Patient Cases Presented.
Penile injuries are relatively uncommon and involve penile fractures, cavernosal hematoma with and without fracture, urethral injuries, spongiosal, and vascular injuries. 1 High-resolution ultrasonography is a cost-effective, time-efficient, and nonionizing modality which is widely available with higher spatial resolution, compared with magnetic resonance imaging (MRI). 8 Also, MRI is an expensive modality with restricted availability, hence it cannot be considered as a part of the routine evaluation of penile trauma. 9
Color Doppler is helpful in evaluating the relationships between the hematoma and the vascular structures and also aid in evaluating the patients having posttrauma erectile dysfunction, to look for any vascular insufficiency, as seen in case 1 of the current case series. Color Doppler may also assist in the follow-up of patients after surgical or conservative treatment. 10
Sonourethrography is also an excellent technique to evaluate the anterior uretheral stricture which can be seen in cases of penile injuries and require evaluation.2,7 Based on the present cases, the following points highlight the merits of using SUG:
A better assessment of complete penile anatomy due to acoustic window provided by the distended urethra.
An assessment of the urethra and its mucosal lining which simulates urethroscopic findings, hence a technique of virtual urethroscopy.
Ability to assess the presence and extent of spongiofibrosis, as well as the length of urethral stricture, if present.
Lignocaine gel was the local anesthetic which eased the procedure of papaverine injection for PPDU and added to penile tumescence.
Therefore, inclusion of SUG with HRUS and PPDU in cases of penile trauma can greatly enhance diagnostic accuracy. This imaging technique will not only make it a single procedure for evaluating patients with penile injuries but is a cost-effective measure for patients.
This case series had a few design limitations. First, a small sample size of patients was included. This was attributed to the low incidence of penile injuries. Future studies with a higher number of patients will potentiate the results of combining the SUG with PPDU. Second, all cases presented late and there were no sonograms or data during acute phase of penile injuries of these cases. However, the diagnostic efficiency of sonography may be difficult due to edema and SUG might have not been possible due to chances of urethral bleeding. Third, in patient case 3, the primary abnormality detected was urethral stricture due to injury and there was no remarkable tear in tunica albuginea. This also presented an opportunity, as this case emphasizes the potential of SUG in detecting urethral spongiofibrosis which would have gone undetected by simple HRUS and PPDU.
Conclusion
Sonography is an ideal modality for evaluating the cases of penile injury. It can very well demonstrate the integrity of tunica albuginea along with the extent and location of tunical tear. Any associated urethral or vascular injuries can also be shown by using color Doppler and sono-urethrogram techniques. Therefore, it is recommended to use the combination of PPDU and SUG in evaluating the cases of chronic penile injury with abnormal penile curvature and insufficiency.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors certify that they have obtained all appropriate patient consent forms. In the form the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.