
Abstract
Fetal head and neck masses, when present, may cause neonatal airway obstruction at birth and associated morbidity and mortality. Escalated maternal treatment intensity such as surgical laryngoscopist/airway surgeon attended delivery and ex utero intrapartum treatment can mitigate the neonatal risk, however, increase maternal risk for complications. Accordingly, accurate prediction of the potential neonatal benefit and maternal risk is essential. Serial third-trimester sonographic features suggestive of more severe airway obstruction may justify more aggressive intervention in the right patient. This case study presents a 23-year-old G1P0 with a fetus predicted to have reduced perinatal airway risk based upon serial third-trimester ultrasound findings. Treatment was de-escalated, and the patient was successfully managed. Collaborative data collection aimed at treatment rightsizing across neonatal, maternal, and systematic domains will support ideal allocation.
Fetal neck masses, including goiter, may cause airway obstruction at delivery with associated complications.1–3 Life-saving and function-preserving airway management strategies are available (see Table 1), but routine delivery presents a limited window for intervention.4,5 Accordingly, preplanning for delivery strategies such as surgical laryngoscopist/airway surgeon attended delivery (AD) and ex utero intrapartum treatment (EXIT) reduces the time from delivery to intervention and prolongs the window for airway intervention, respectively.5,6
Listing of Various Airway Management Techniques.
The simultaneous treatment of mother and baby during delivery greatly increases the decision-making complexity. Vaginal delivery carries with it the risk of birth prior to full team mobilization/preparation and dystocia in cases of neck masses. 6 Cesarean delivery, in contrast, increases maternal risk for blood loss, thromboembolism, and infection as well as uterine rupture, placenta accreta spectrum, subsequent cesarean deliveries, and hysterectomy in the next pregnancy. 7 In addition, EXIT requires general anesthesia, extensive resources, and risks to the mother, such as placental abruption and uterine hemorrhage.8–11 Therefore, an accurate prediction of neonatal viability (independent of the airway) and probability of birth plan alteration to benefit the neonate IS critical to weigh against maternal risks.7,12
Neonatal viability independent of the airway is inferred from adjunct imaging studies such as magnetic resonance imaging (MRI), serial ultrasonography, and echocardiography, as well as genetic testing. These are recommended prior to undertaking an intervention that may risk undue harm to the mother and fetus.2,5
The probability of a change in delivery strategy to benefit the neonate is arguably the most important and difficult variable to predict accurately. Risk factors for airway intervention at birth include anatomic compression, elevated amniotic fluid index (AFI)/polyhydramnios, and solid mass/teratoma etiology. These, along with neck vascular compression, neck extension due to mass, size >5 cm, and floor of mouth location, are criteria sufficient to justify consideration of EXIT for some providers.5,13–15 Others reserve compression, defined by the tracheoesophageal displacement index (TEDI) >12 mm, as the most important decision criterion and select AD for less severe cases.5,14 While these are valuable metrics, the optimal data will permit prediction modification of maternal and neonatal outcomes based on various decision points. In evaluation for EXIT, the risks and benefits to both fetus and mother should be considered an essential part of surgical decision-making.
The case report highlights a fetal goiter sufficient to justify AD or EXIT depending upon preferred criteria that was managed by vaginal delivery with otolaryngologist attendance. The role of serial ultrasonography to support treatment de-escalation and imaging features that may support vaginal delivery is discussed. The need for data collection across neonatal, maternal, and systematic domains to support treatment rightsizing according to maternal values is emphasized.
Case Report
A multidisciplinary team cared for a 23-year-old G1P0 carrying a fetus with an antenatal diagnosis of a goiter, identified at 19 6/7 weeks on ultrasonography (US). On subsequent US imaging, the thyroid measured up to 5.6 cm long with a volume of 71.3 cm3, significantly elevated from the gestational age controlled mean of 0.42 ± 0.21 cm3. 16 The AFI values were within normal limits. A fetal MRI study (see Figure 1A and B) demonstrated a T1 hyperintense, T2 hypointense bilobed anterior neck mass expanding the visceral space with circumferential tracheal narrowing. There was anterior airway and posterior esophageal displacement. The cervical vessels were mildly displaced without luminal irregularity.
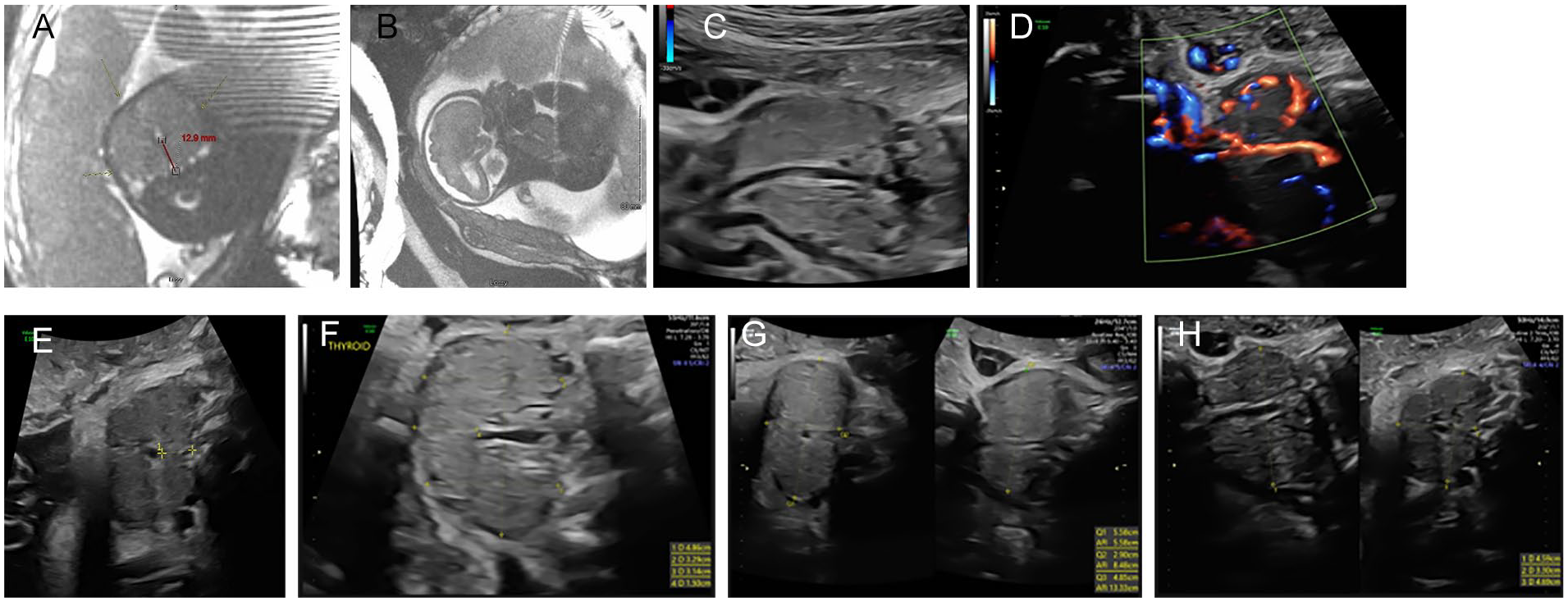
(A–H) A fetal magnetic resonance imaging performed at 30 weeks, 1 day gestation (A & B) and serial third-trimester fetal sonogram. (A) An axial view showing circumferential central neck compartment mass (arrows) resulting in tracheal displacement of >12 mm (red line) and mild vascular compression. (B) A sagittal view showing the mass (M) causing narrowing and partial obstruction of oropharyngeal airway (red arrow). (C) A sagittal view showing airway patency (*). (D) A demonstration of flow within the tracheal lumen. (E) An axial view showing the mass (M) causing anterior tracheal displacement (*) from cervical spine (C) of 11.5 mm. (F) A fetal thyroid with dimensions taken at 33 weeks. (G) A fetal thyroid with dimensions taken at 37 weeks. (H) A fetal thyroid with dimensions taken at 38 weeks.
Weekly third-trimester US showed a patent airway (flow of a continuous column of fluid through the larynx and trachea with fetal respirations) with minimal thyroid enlargement measured over time, adequate fetal neck flexion, and reduced tracheal displacement to less than 12 mm (see Figure 1C–H]. Multidisciplinary discussion with the mother, including more recent and favorable serial US data, led to a maternal decision for a vaginal AD (Figure 2A and B).
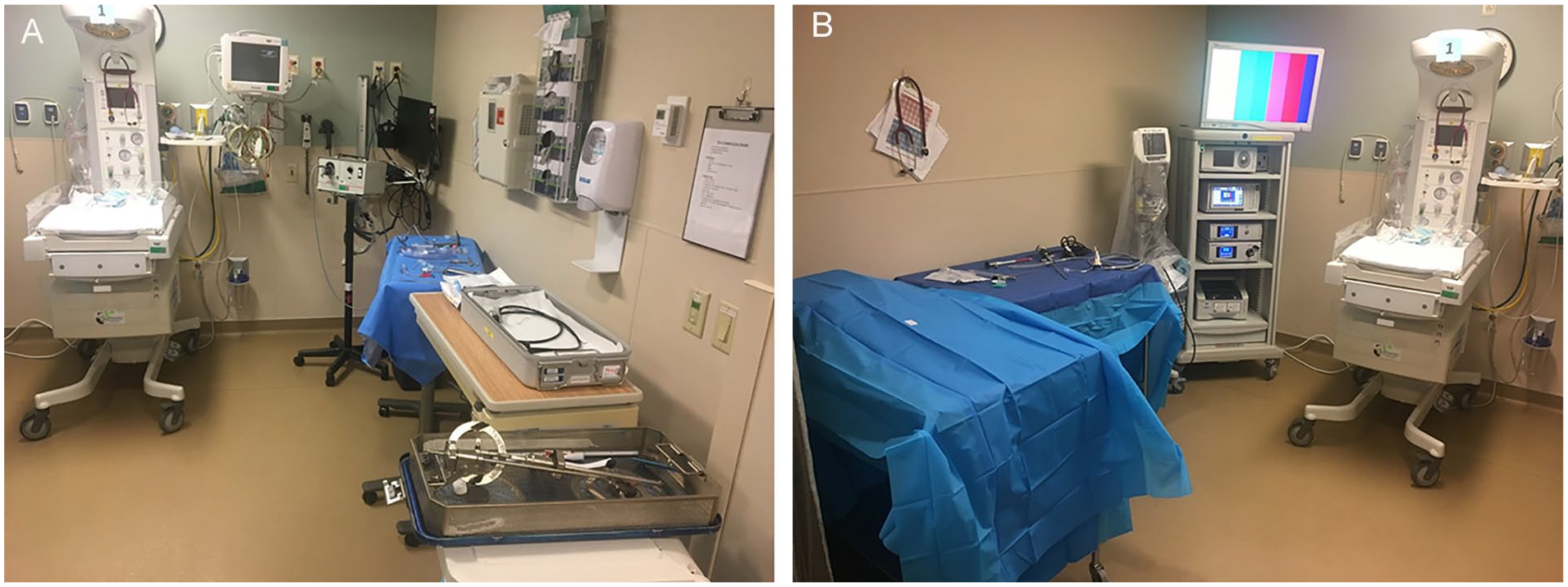
(A and B) An attended delivery set up in adjacent Post Anesthesia Care Unit (PACU) bay. (A & B) Equipment was prepared for resuscitation, video laryngoscopy, operative laryngoscopy, videotelescopic intubation, rigid ventilating bronchoscopy, transnasal fiberoptic intubation/intubation via laryngeal mask airway, tracheostomy, retrograde intubation, and mass decompression.
The male neonate was born via vaginal delivery at 38 2/7 weeks gestation with Apgar scores of 81 and 95. He did not require any respiratory intervention and was discharged to home on day of life 2 with recommended thyroid labs and endocrinology follow-up. Further assessment revealed hypothyroidism and two pathogenic mutations in the thyroperoxidase gene, one likely pathogenic mutation in the SLC26A4 gene, and mosaic Turner syndrome (45X0 and 46 XY). Thyroid hormone supplementation was initiated, and evaluation revealed no other systemic anomalies. The patient is growing well and making good developmental progress.
Discussion
Delivery with potential airway obstruction is a rare and uniquely high-stakes procedure requiring simultaneous management of multiple patients with conflicting medical needs. 5 Accordingly, a comprehensive and well-informed multidisciplinary team is paramount to successful management. Best practices incorporate the newest evidence, place technical experts at the bedside, appropriately weigh risks and benefits of intervention and nonintervention, and adapt to new information based upon the collective skillset to rightsize resources and facilitate optimal patient-centered outcomes. Accordingly, methodical predictive data are necessary across maternal, neonatal, and systematic domains to support individualized decision-making.
Fetal goiter is among the most common indications requiring an EXIT to airway procedure.1,2 In this case, anatomic compression represented by tracheal displacement of 12.9 mm, solid mass character, size >5 cm, and neck vessel compression as seen on fetal MRI and US at a similar gestational age predicted a more complicated course and could have justified an EXIT. As the pregnancy progressed, however, serial US demonstrated reduced tracheal displacement to 11.5 mm, maintained airway patency, and minimal neck vessel compression. Furthermore, the fetal thyroid volume changed minimally within the third trimester, compared with a typical developmental quadrupling, over the same time period. 16 Finally, adequate fetal neck flexion supported a more favorable airway. 15 While MRI provides comprehensive assessment of fetuses with head and neck masses, serial US offers readily accessible, fluid, and potentially more up-to-date data.2,5 When performed, serial US may be scheduled every 2 to 4 weeks. 2 Worsening findings such as polyhydramnios or fetal hydrops justified treatment escalation. 5 This case demonstrated that US was equally useful for treatment de-escalation; however, few data examine such an application.
In cases of severe obstruction and predicted intervention, time precludes performance of all potential interventions prior to hypoxic injury or death in the absence of delivery modification. EXIT offers the most flexibility with average uteroplacental support duration of 45 minutes and duration up to several hours.1,2,17–22 Incomplete variations in EXIT, sometimes termed operation on placental support, offer an estimated 1 to 20 minutes.2,21,23,24 Vaginal delivery with sustained placental support is reported, however, risks fetal to placental transfusion and unpredictable placental separation. 21 Excellent reviews of various techniques are available elsewhere.2,6
The providers in this case discussed the interventions available for airway distress as shown in Table 1. Techniques such as surgical approaches to the trachea through the goiter would be challenging, if possible, in the time window of an AD. The relative likelihood of such an intervention, however, was felt to be low based upon data in nine individuals with fetal goiter who underwent EXIT and the heterogeneous nature of fetal neck masses used to generate other predictive criteria. Among the nine cases of EXIT for goiter, intervention was performed in 78% of cases. Importantly, intubation was the definitive intervention in each delivery.25,26 These factors reinforced the parental decision for AD. Given adequate neck flexion, the dystocia risk was felt to be minimal and team mobilization was felt to be reliable. This led to the recommendation for a vaginal delivery.
Future research should include a greater level of specificity with the aim of supporting personalized medicine. Neck masses should be differentiated by etiology, severity characteristics, and anatomical site. Currently, fetal neck mass severity predictive data are derived largely from teratomas and lymphatic malformations, and future study should examine larger numbers of pathologically enlarged anatomic structures such as goiter and de novo lesions. 13 Data should identify patient groups by similar diagnosis and severity rather than intervention applied, and analysis should integrate multiple factors when possible. 14 The significance of laryngeal and/or tracheal displacement versus tracheoesophageal displacement remains to be clarified. In addition, the appropriateness of vaginal rather than cesarean delivery and differentiating criteria is needed in AD. The optimal timing of serial US and precise impact of imaging features on the risk/benefit profile of various management options should be explored. Improvement efforts will likely include health systems research to examine the personnel and equipment necessary by presentation and support efficient resource mobilization. At present, several lists of instruments/preparation checklists are available to facilitate AD mobilization.2,5,6 Qualitative investigations should be performed and used to drive future research according to patient priorities. The psychologic impact of prenatal airway diagnoses and treatment warrants examination including mental health intervention. To achieve such aims, in the face of infrequent and diverse presentations, multi-institutional, interdisciplinary teams should form to pool data that offer the opportunity to elucidate treatment variations and improve suboptimal outcomes.
Conclusion
Fetal neck masses including goiter are an indication for delivery plan modification in select cases to benefit the neonate. Delivery plan modification, however, may increase the risk of harm to the mother so careful consideration and thoughtful allocation are required. The ideal balance of potential fetal benefit and maternal risk is individualized according to maternal values, and the optimal intervention may be different for identical fetal presentations in different individuals. To support patient-centered treatment, robust information about all treatment variations and predicted outcomes is required and collaborative efforts are entertained.
Footnotes
Acknowledgements
The authors recognize the contributions of providers associated with the multidisciplinary UW Health Fetal Diagnosis and Treatment Center, including Drs Bauer, Brucker, Duffy, Kille, Kuner, Racine, Rhoades.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.