
Abstract
This article discusses the importance of conducting a longitudinal data collection concerning well-being and the risk for work-related musculoskeletal injuries (WRMSI) among sonographers and vascular technologists. There is a need for changes in the manner that sonographic work is done, but this should be nested in empirical evidence. This gives the rational for conducting the study titled Documenting the overall wellness of ultrasound users and the risk of progressive WRMSI: A national longitudinal study. The objective of this longitudinal work is to better understand collective practice patterns and examine the relationship of sonographic work conditions and performance to the user’s health and well-being. This symposium provides the foundational understanding of the strength of this type of study and how it may help to influence behavior and organizational change.
Carlos’s experience: “I first noticed that I had a work-related injury when I was attempting to do a renal sonogram on a comatose intensive care (ICU) patient. I had been doing portable sonographic examinations in our ICU since I was a student sonographer. The patient and examination did not seem out of the ordinary until I attempted to lean over the bed and patient, to complete the left kidney scan. I struggled to keep my footing and also center the image on the screen. I was intently staring at what looked like a severely obstructed left urinary system, when my arm went numb. The image disappeared from the screen and I looked at the patient and noticed that I had dropped the transducer into the bedding. I could not feel my arm, while my wrist and fingers were stinging. I tried shaking my hand repeatedly to regain feeling and then ran around to the other side of the bed, to retrieve the transducer. I was so self-conscious about this event and worried that I had damaged the transducer. I remember thinking, I hope nobody in the ICU saw me drop the transducer. Looking back on this incident, I should have been concerned about the damage to my arm and wrist, not just potential damage to the transducer!!”
Abby’s experience: “When I first became a sonographer/vascular technologist I was aware that work-related injuries occurred in our field. However, as a new technologist, my biggest concerns were image quality, patient comfort, exam time and keeping up with my coworkers. I was not focused on how my body was positioned or how I was holding the transducer. As time went on, I found that I was experiencing lower back pain during exams, along with wrist and thumb discomfort, but I told myself I only needed to put up with a couple more seconds of pain, in order to get the images needed. Repeatedly working in awkward positions during exams has caused lower back pain to now occur after exams are finished and throughout my day. During certain exams, my thumb and wrist will cramp and spasm. I am now trying to correct years of continuous strain during exams from twisting, turning, and putting my body into awkward and uncomfortable positions. I now understand why my instructors were so adamant about taking the time to set up exams properly and seek out help regarding exercises, strengthening, room set up and proper equipment to prevent injury!”
In July 2018, the American Registry of Diagnostic Medical Sonography (ARDMS)-Inteleos, Inc., hosted a community engagement group (CEG), which brought together the chief operating officers, presidents, and representatives from the following organizations: American Institute of Ultrasound in Medicine (AIUM), American Society of Echocardiography (ASE), the Intersocietal Accreditation Commission (IAC), the Joint Review Committee for Cardiovascular Technology (JRC-CVT), the Joint Review Committee for Diagnostic Medical Sonography (JRC-DMS), the Society of Diagnostic Medical Sonography (SDMS), and the Society of Vascular Ultrasound (SVU). Individually, these professional organizations deal with the specific issues and programming needs of their constituents. Prior to this meeting, these organizations were dealing with the concerns expressed by their members about work-related musculoskeletal injuries (WRMSI).
At this landmark meeting, the organizations and their leaders provided updates on their activities and ways to potentially collaborate. In addition, a professional facilitator helped the representatives to generate some of the major challenges facing the community of physicians, sonographers, and vascular technologists (“ultrasound users”). At the end of the session, the CEG attendees were able to post many constituent challenges and then prioritize the most important ones for the group to tackle. Through a process of voting, the members overwhelmingly chose the risk of WRMSI threatening sonography workers.1,2 The outgrowth of the CEG meeting was a commitment to work together to tackle this very important issue and this was the birth of the WRMSD Alliance. The follow-up meeting for the newly formed WRMSD Alliance was in September 2019, where representatives convened to design methods for evaluating and improving the impact, metrics, coordination, funding, and communication that would be needed to properly deal with the sustained risk of WRMSI. 3 This design summit of organizations and leaders was the start of harnessing the collective power of the community to address this threat to all ultrasound workers. Unfortunately, the pandemic stymied a lot of the synergy that these meetings had created. Nevertheless, the WRMSD Alliance held virtual meetings to form action committees and begin detailing the work needed. One such committee that was formed was called the Metrics Group. The Metrics Group began meeting to discuss how a more current survey of the problem of WRMSI could be executed and what kinds of questions might be important for assessing the risk for injury. Besides the Metrics Group meeting virtually, the WRMSD Alliance also hosted a Hack-a-Thon (early 2020). The virtual student solution Hack-a-Thon consisted of four teams of students from a variety of educational backgrounds and universities, and they competed to provide innovative solution concepts to address the risk of WRMSI among ultrasound users. 3 This forward momentum was temporarily suspended due to the increasing burden of the pandemic on the organizations, the leadership, and the volunteers themselves responding to surges of infected patients across the United States. The Metrics Group was able to complete their work and provided the WRMSD Alliance with a bank of potential survey questions but advocated for this to be more than just one more survey of the prevalence of work-related musculoskeletal disorders (WRMSDs) in sonographers; rather they wanted an ongoing data collection effort to document the progression of acute injuries (WRMSI) to more chronic conditions (WRMSD).
In June 2020, the WRMSD Alliance began to review the product of the Metrics Group and determined that a rigorous survey was needed and that the development of a “registry” or longitudinal data collection of ultrasound workers would be a novel and worthwhile undertaking. The announcement was made that the work of the Metrics Group would be handed off to the research team at the Ohio State University so that a true longitudinal research effort could be executed.3,4
With seed funding from the WRMSD Alliance, the Ohio State University OSU research team begin sifting through the work completed by the Metrics Group and looking at the proper research methodology needed to execute a longitudinal survey research study that would document the health and wellness, over time, of those ultrasound users who would participate in the study.
Research Methodology—A Longitudinal Data Collection
One of the key advantages of developing a longitudinal study approach is that researchers may have the ability to detect developments or changes in the characteristics of the sample population, at both the collective and the individual levels. Certainly, an offset is the challenge of keeping the participants responding to the data collection and attempting to capture the sequencing of causal events.5–7 This typology is different than a cross-sectional study of participants, which is an effort that only gathers information in a one-shot fashion, at one point in time. The level of scientific evidence generated by a longitudinal study approach is considered unfiltered and increasing in strength (see Figure 1).
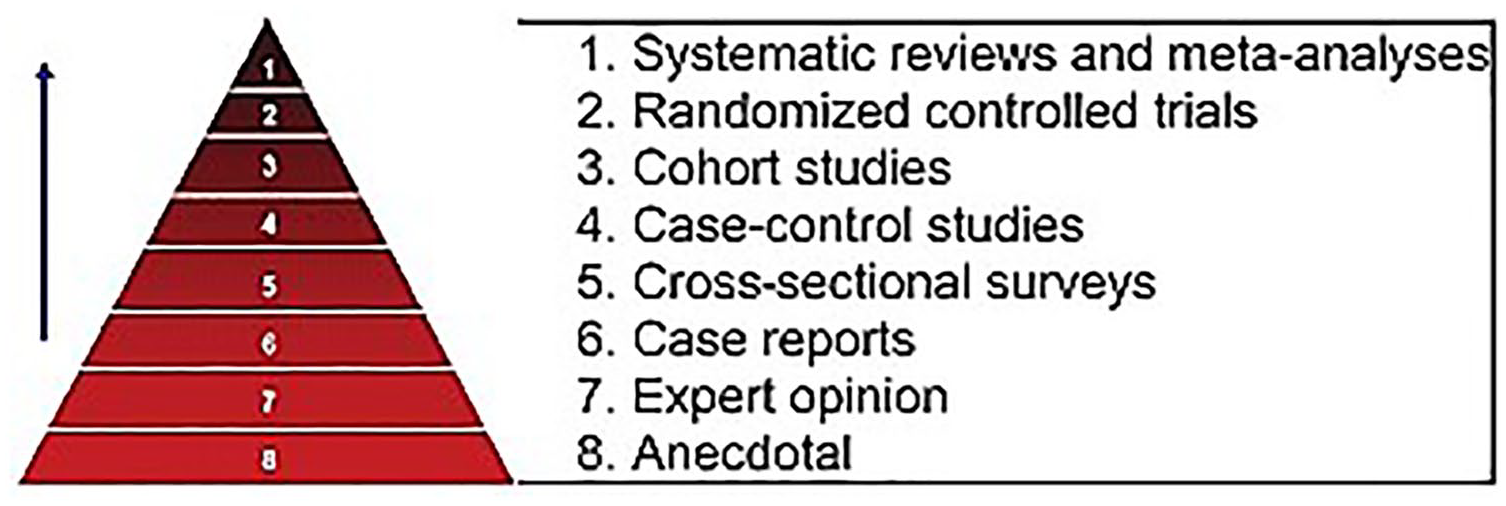
The scientific strength of evidence pyramid. 8
It is important to acknowledge the cross-sectional studies that have provided important information and alerts about the prevalence and risk of WRMSD in the sonography community. Without these prior studies of self-reported injuries of sonographers and vascular technologists, the current longitudinal work would not have begun with such a firm foundation. Of these, our survey report 9 of 2963 sonographers, published in 2009, and three secondary analyses of those existing data10–12 are the largest and most cited studies on discomfort and the disorders among sonographers. That research not only highlights the extreme prevalence but also provides specific details regarding awkward work postures, inadequate training in ergonomics, and organizational pressures that contribute to injuries. In addition to the studies just mentioned, other cross-sectional surveys as well as experimental research studies have provided valuable information about self-reported discomfort and injuries in sonographers throughout the world, while experimental and observational studies have evaluated postures, kinematics, and muscle activation patterns during scanning, through use of observational, electromyographic, and video analysis techniques.12–51 Regardless of the awareness that has been raised about this persistent problem among ultrasound users, no longitudinal study has been conducted to document effects of risk factors or interventions over time. This is an important knowledge gap that the current research aims to address. Importantly, this effort will generate a higher level of scientific evidence that is so important and critical in contributing to the WRMSD Alliance’s Grand Challenge to stop the development of WRMSD in ultrasound users.
Theoretical Framework for Collecting Longitudinal Data on WRMSD
As has been described in Sommerich’s editorial, using a sociotechnical systems framework can help identify factors that contribute to the problem of WRMSD for ultrasound users, as well as make progress on developing solutions. 52 Evans and Sommerich have both proposed the use of a framework similar to the Systems Engineering Initiative for Patient Safety (SEIPS) model 53 as a means to ground the selection of variables for gauging risk for WRMSD (see Figure. 2).
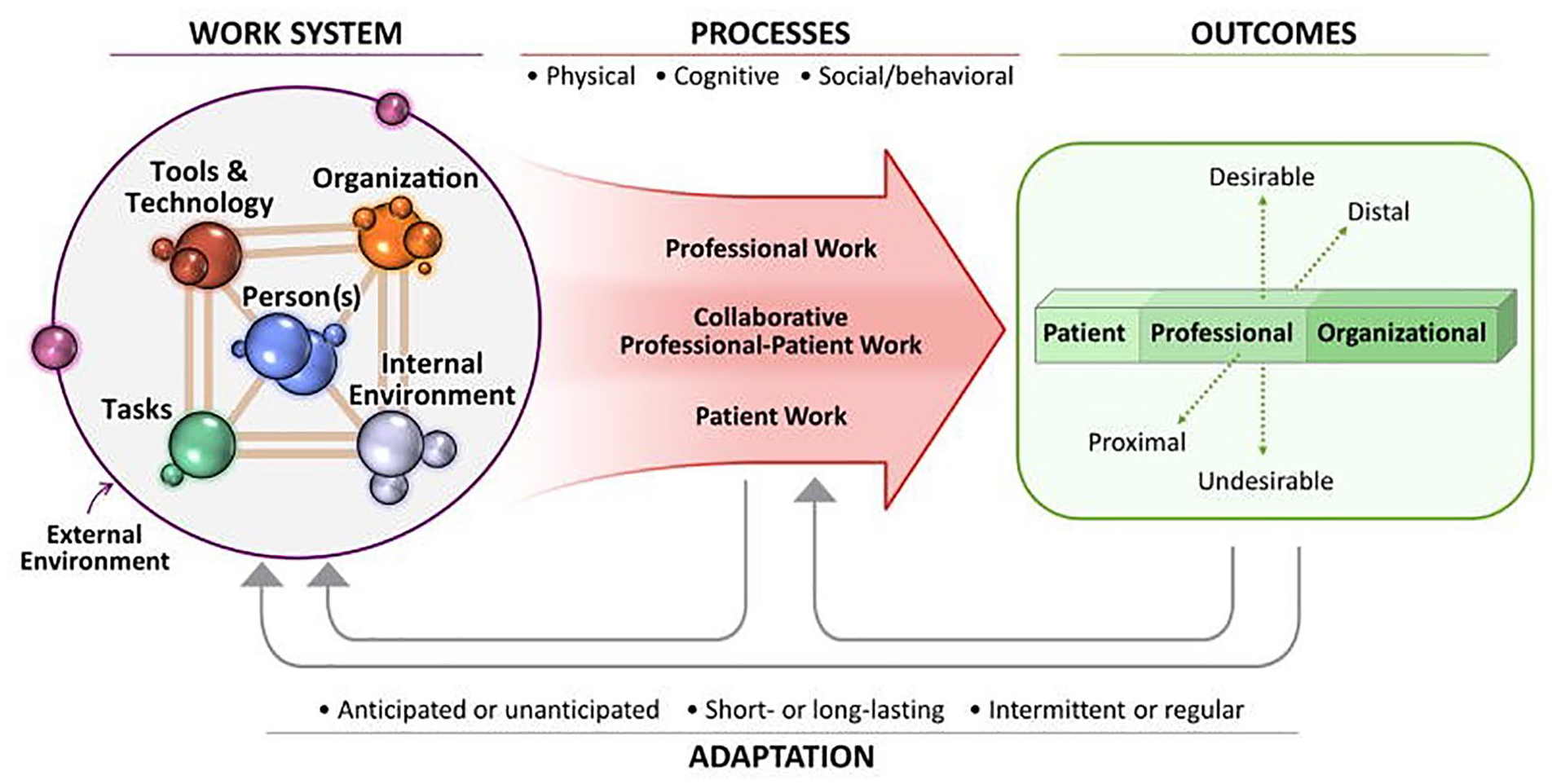
The Systems Engineering Initiative for Patient Safety (SEIPS) model. 53
The SEIPS model displays the broad spheres of potential influence impacting the persons in the work system (we are particularly focused on ultrasound users), as well as impacts on work processes and outcomes. These work system domains were a major influence for the research team to determine what kinds of longitudinal survey questions would be needed. This theoretical framework not only helped with survey organization but also guided the survey item selection and editing process, from the pool of items created by the former Metrics Group. Once the pool of survey questions was edited and organized, it was much easier to select those items that would be used to build the first surveys in the series (Surveys 1 and 2). A primary objective is to collect longitudinal data, specific to each of the variable categories outlined in the SEIPS model, to better understand the patterns of risk and outcomes Musculoskeletal (MSK discomfort) over time. This data may also be used to detect developments or changes in various groups of ultrasound users, defined by practice specialty, for example, provided the number of study participants is sufficient and sustained over time. This anticipated association of tasks, organization, environment, technology, and tools will be a focus of the data analysis.
Commitment to Continue Data Collection for Determining Cause and Effect
One of the main advantages of executing a longitudinal study is to better establish the correct sequence of events (exposure prior to outcome), identify changes over time, and provide insight into the factors that might be contributing to the development of WRMSD. Collecting repeated information from the same participants is critical to being able to determine cause and effect relationships. This is why we are grateful to the cohort of current participants and why we so strongly encourage each of you to remain engaged in this effort by participating in the future surveys as well as other participation opportunities (e.g., interviews). We also invite those who have not previously participated to consider joining this investigation that will benefit the ultrasound user community. To find out more, please visit this webpage: https://u.osu.edu/sonographywellbeing/
Examples from other health care domains demonstrate some of the benefits that can be gained from conducting longitudinal research. One such study examined the relationship between baseline information, personal factors, working characteristics, and job performance among Taiwanese nurses working in an emergency department. 54 In that study, a survey was administered to the emergency department nurses at three different time points. The objective was to isolate some of the key factors that might contribute to retention and bolster quality of nursing service for this cohort. A questionnaire was developed that used Likert scales to capture the nurses’ perceptions about their work in the emergency department. Of the specific domains investigated, researchers found that biological protection and a climate of safety were significantly related to task performance. 54 They also noted that nursing skill performance was strongly linked to the feeling of a work climate of safety. 54 It was interesting to note that the repeated measures, due to survey administration, showed some increase in job performance and task performance over time. 54 This kind of data was important to share with hospital administration in this locale to assist them in improving the work environment and administrative support for these employees. This feedback demonstrates how longitudinal survey work can uncover patterns of association in the data and inform stakeholders in ways that can lead to meaningful change.
Another example comes from a study of older workers at risk for WRMSD. This particular study was designed to investigate the association between physical work-related factors and injuries among US workers, and then compare the injured and uninjured workers with regard to consequences, including functional limitations and reduced working hours post-injury. 55 Risk of experiencing a work-related injury event was over two times greater among those whose job had work requirements for physical effort, lifting heavy loads, stooping, kneeling, and crouching, compared with those who did not. 55 Over time, the older injured workers compared with the uninjured had higher risks of functional limitations and working fewer hours. 55 This type of data has the potential to inform employers of older workers that accommodations need to be considered so that these employees can maintain their productivity. Longitudinal studies, like the one mentioned above, can demonstrate a pattern of events that could be detrimental to keeping this important part of the workforce contributing. Without this type of data provided to employers, the risk of losing older workers is high and providing the wrong accommodations is highly likely. These published results, from high-quality longitudinal studies, have provided empirical evidence that can be used to help in mitigating the risk for specific workers and improve employee and employer outcomes. These are the same kind of outcomes that are desired for the current longitudinal research involving ultrasound users.
Implementation of Scientific Evidence to Make Significant Change
As results from this longitudinal study are reported out to the community, it is important to begin thinking about how the evidence-based results can be implemented to reduce the risk of WRMSD. Typically, scientific evidence is used to improve patient outcomes, and therefore, it is appropriate to consider a similar model of implementation.
Sackett et al. posed that implementing evidence into practice required four critical components: (1) framing the clinical question, (2) finding the evidence, (3) assessing the evidence, and (4) using the evidence to make your clinical decision. 56 It is also important to mention another approach, which is grounded in creating interventions that are an outgrowth of this implementation science approach; this has been referred to as RE-AIM. 57 Goldenhar et al. also advocate the need to “re-aim” or refocus efforts to find solutions for occupational safety issues based on the evidence created. 58
In the case of mitigating the risk for WRMSD among our ultrasound users, the longitudinal study results will be provided to address questions concerning which factors appear to increase or reduce the risk of WRMSDs. Given the longitudinal nature of the data, the results will generally be of a higher quality of evidence that may persuade administrators, managers, supervisors, and individual ultrasound users to consider adopting evidence-based mitigation approaches to reduce injuries.
Conclusions
The ongoing contributions being made by over 3660 respondents are quickly adding to our understanding of WRMSI, WRMSD, burnout, numbers of examinations, COVID-related changes to work, and so on. The collection of this cohort’s responses should not be considered a static database, but rather a dynamic repository of valuable information. The hope is that the organizations that make up the Alliance will look to this database for tangible results of this research. The participants that make up the database represent a reliable large cohort interested in providing information to questions and future inquires. This unique database contains substantial representation of workers in Abdominal, Cardiac, OB/Gyn, and Vascular Technology, as well as a group of Doctors of Medicine (MDs). These groups have different needs and levels of exposure to risk factors for WRMSI. Results from data analysis will be organized in ways that each Alliance organization will be provided with information specific to their group of members, as well as results that generalize across the database. These results will be useful for making informed decisions on organizational priorities. Organizations could use results from this longitudinal research to directly address educational efforts to reduce the risk of WRMSD, spur workplace solutions that mitigate WRMSI, and other related initiatives. The database provides a means to document MSK health and gather information about expressed needs and experiences of individual ultrasound users. In addition, maintaining this group of respondents allows organizations to assess their specific solutions or educational programming and get feedback as to its usefulness and effectiveness. Supporting the database also allows for maintaining the infrastructure, as well as adding new participants into the system. Use of results from the data analysis will provide each organization with the ability to make data-driven decisions to address their group of members’ risks/concerns. I believe that additional activities, such as Hack-a-Thon, and working with safety consultants or safety-related agencies can be more targeted and informed, through support of ongoing data collection and analysis efforts and utilization of the results from the analyses of this unique database. Data-driven programming that it is developed to address responses from the dataset and that is informed by input from potential recipients of that programming is likely to be more effective and is likely to be well received by colleagues. More work is needed not only to report out the findings thus far but also to continue collecting additional relevant information in each of the work system areas (tasks, work organization, tools and technology, and environment) that will contribute to our developing understanding of well-being and WRMSD in ultrasound users, in terms of risk factors and effective mitigation strategies.
Footnotes
Acknowledgements
The authors would like to acknowledge the critical input of Loretta Damron, BS, RDCS (adult and pediatric); Yusef Sayeed, MD, MPH, MEng, CPH, CMRO, CME, COHC, MSKME, RMSK, DABPM, FAIUM; and Kate Sayeed, MD.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research team would like to thank the SDMS and SDMS Foundation for their financial support of this survey research.
Peer Reviewer Guarantee Statement
The Editor/Associate Editor of Journal of Diagnostic Medical Sonography (JDMS) is an author of this article; therefore, the peer review process was managed by alternative members of the Board, and the submitting Editor/Associate Editor had no involvement in the decision-making process.