
Abstract
Traditionally, large bowel obstruction (LBO) can be due to a neoplasm, most often colorectal cancer. Also, fecal impaction (FI) is a common disease, which occurs in a variety of ages and is significantly increased in the elderly. This case report is of LBO caused by FI, in which ultrasonography (US) proved to be useful for diagnosis and follow-up. A 60-year-old female had abdominal pain after taking a laxative as part of bowel preparation for colonoscopy. The US diagnostic findings were a marked dilation of the bowel, due to watery stool, in the ascending colon, and a clear FI, in the descending colon. Computed tomography showed similar findings to the US. There was a large amount of defecation after treatment and US demonstrated an improvement in the ileus. Ten days after admission, a colonoscopy revealed no stenosis or tumor, as a cause for the ileus.
A fecal impaction (FI) has been defined as a large mass of compacted feces, at any intestinal level, which cannot be evacuated spontaneously. 1 A FI can cause bleeding and perforation due to compression of the colon wall and the common result is a large bowel obstruction (LBO). 2 Those at risk for presenting with a FI are children, incapacitated patients, and the institutionalized elderly, which are considered to most affected population. 3 A FI can have serious consequences from a healthcare, socioeconomic, and quality of life standpoint. Thus, treatment and management of a FI are required as part of daily medical care. This case report is provided to demonstrate that transabdominal ultrasonography (US) was useful for the diagnosis and follow-up of a LBO caused by a FI.
Case Report
A 60-year-old female was admitted to the emergency department with sudden epigastric pain, and nausea. Her blood test results (white blood cells, C-reactive protein) were within normal limits. On physical examination, the patient did not have a distended abdomen or signs of peritonitis. Abdominal plain radiographs revealed stool and gas retention, from the ascending colon to the descending colon (see Figure 1A). A plain computed tomogram (CT) was performed on the abdomen and pelvis, with CT images demonstrating fecal retention, in the ascending colon (see Figure 1B). However, the patient had no history of constipation. The day after admission, the patient had improved abdominal pain and nausea. Three days after admission, a colonoscopy was scheduled to determine the cause of her abdominal pain. On the day of the examination, the patient experienced abdominal pain after taking a laxative (1.5 L, polyethylene glycol electrolyte solution), which was a bowel preparation for colonoscopy. Immediately, US was performed to determine the source of the abdominal pain. The US findings were marked dilatation of the entire ascending colon to about 5 cm, due to watery stool (see Figure 2A) and a discernable FI, in the descending colon (see Figure 2C). The US documented normal bowel peristalsis (a lack of fluid or hard stool retention) and the colon had a flattened outer boundary wall without acoustic shadows. The bowel lumen demonstrated uniform hyperechoic areas within the ascending and descending colon (see Figures 2B and 2D). The CT examination, performed immediately after the US, provided a coronal image showed similar diagnostic findings (see Figure 3). The patient was diagnosed fecal ileus caused by laxative preparation for colonoscopy and discontinued colonoscopy. A defecation treatment by bisacodyl suppository was conducted. The next day, there was a large amount of defecation and improvement of the ileus, which was sonographically confirmed (see Figure 4). On the 10th day after admission, a colonoscope revealed no stenosis or tumor which could have caused the ileus.
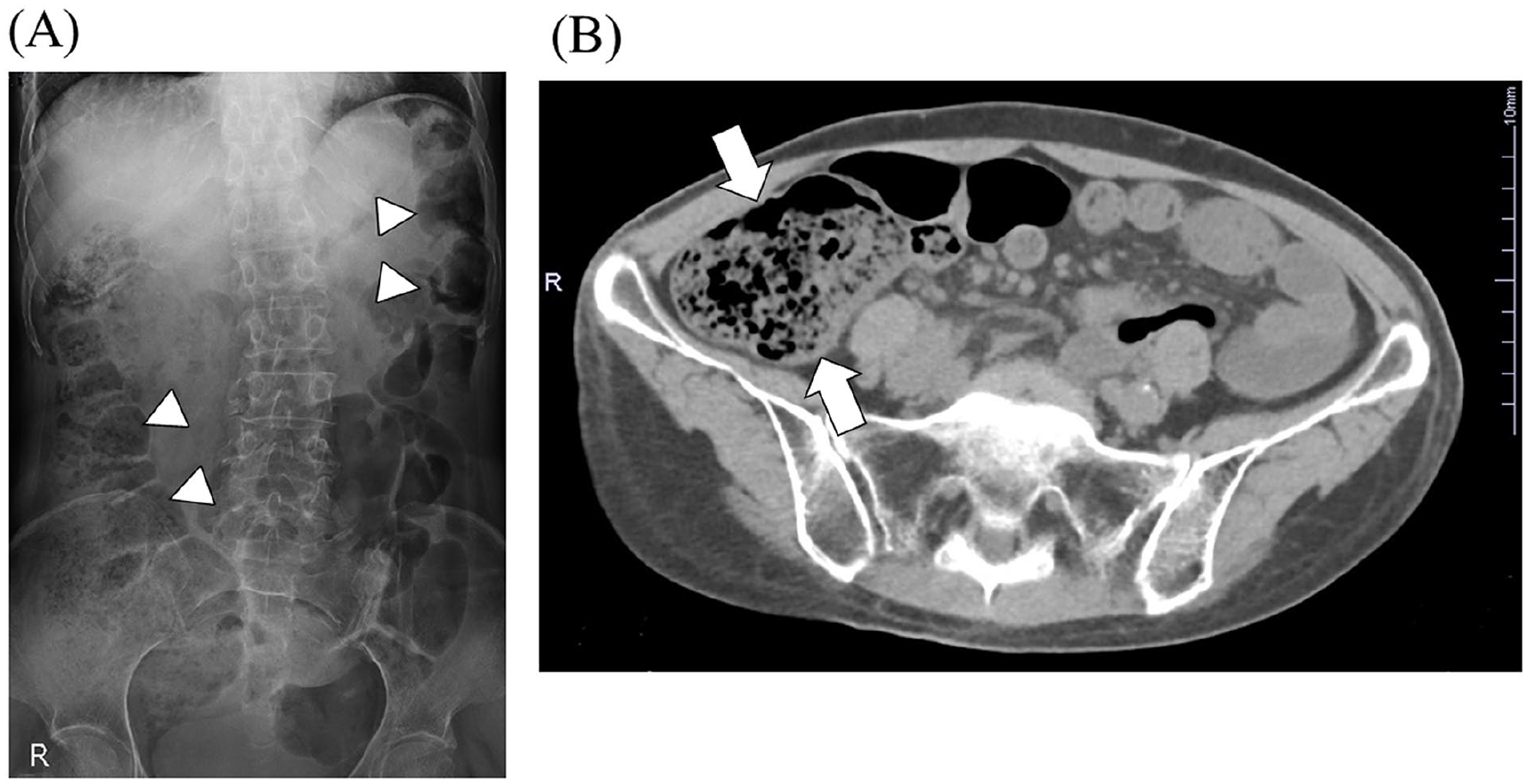
The diagnostic imaging findings from a 60-year-old woman, upon hospital admission. (A) An abdominal radiographic image demonstrated stool and gas retention from the ascending colon to the descending colon (See arrows). (B) A computed tomographic image demonstrated fecal retention, in the ascending colon (see arrows).
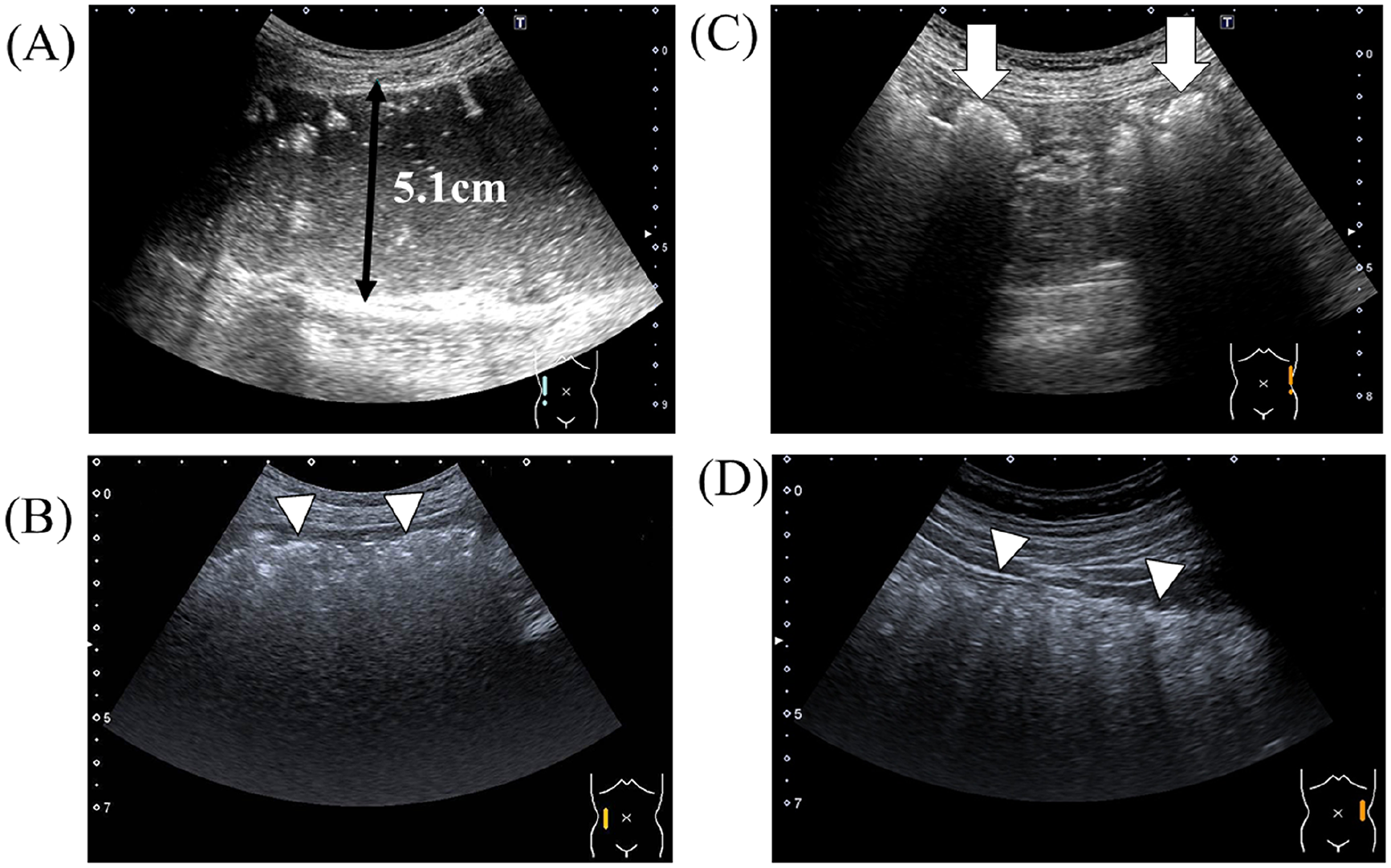
The sonographic examination preformed after the administration of a laxative bowel preparation for colonoscopy. (A) A longitudinal sonographic view shows strong dilation due to watery stool in the ascending colon (lumen diameter: 5.1cm). (B and D) Normal bowel peristalsis is documented with sonography (No fluid or hard stool retention). The bowel had a flattened outer boundary wall without acoustic shadows and hyperechoic area with uniform inside of the ascending and descending colon wall (See arrows). (C) A longitudinal sonographic view shows clear fecal impaction in the descending colon (See arrow).
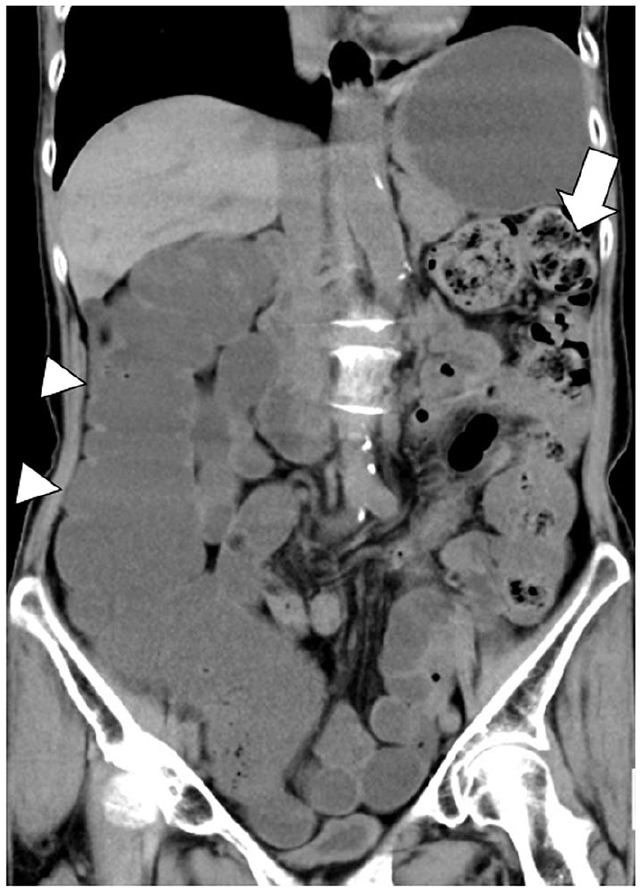
A coronal computed tomographic (CT) image was completed after taking laxative bowel preparation for colonoscopy and showed similar findings to the sonogram. The CT findings demonstrated a marked dilatation of the entire ascending colon (See arrow), and a clear fecal impaction, in the descending colon (See arrow).
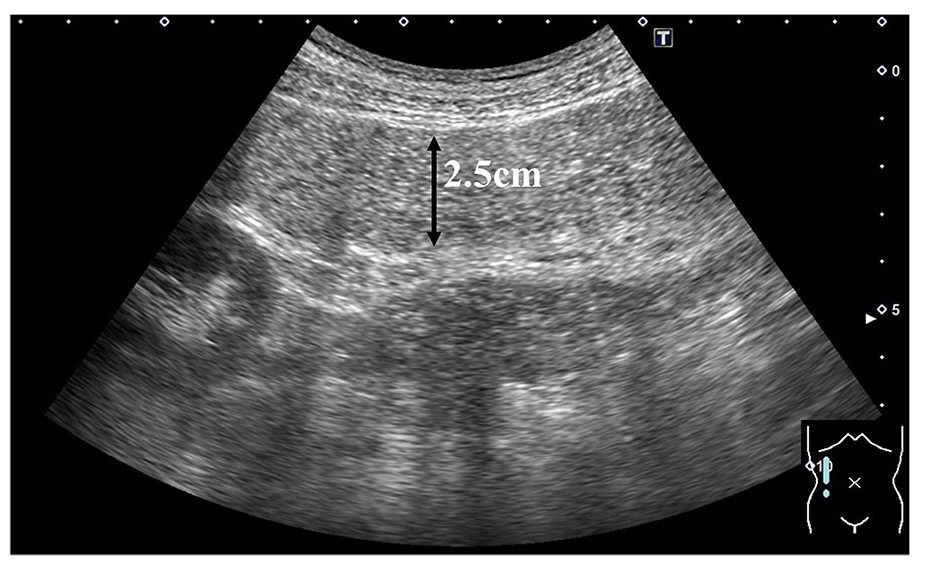
The day following defecation care, with a bisacodyl suppository, the sonogram showed improved dilatation of the ascending colon (lumen diameter: 2.5 cm).
The equipment used for the sonographic examination was an Aplio® ultrasound equipment system (Toshiba Medical, Ltd., Tokyo, Japan), with a 4 MHz curved-array transducer. The sonographic interrogation was based on a focal range and image-depth thickness of 5 to 9 cm, to determine the correct display range. The overall system gain was set at 70, the dynamic range at 65, and differential tissue harmonic imaging was 5.0.
Discussion
A FI is a common occurrence which occurs in all age groups but is significantly increased in the elderly. 3 A FI can simply manifest as an inconvenience, nuisance with bothersome symptoms of straining, and overflow incontinence, which could result in a surgical perforation and sepsis. 4 However, a uniform definition of FI has not been agreed upon by all medical, surgical, and nursing societies. 5
In general, the documentation of constipation is performed with an abdominal radiograph or abdominal CT. However, these procedures have to expose patients to ionizing radiation. Conversely, US could be a practical diagnostic test due to its rapidity, low cost, and noninvasive follow-up. 6 Several recent studies have reported on the use of US as a means to diagnose constipation, as an effective clinical tool.7-9 Tanaka reported that solid fecal material, in the colon, can be characterized sonographically, as crescent-shaped acoustic shadows with haustrations and strong hyperechoic area, within the colonic lumen. 9 In the present study, US demonstrated similar findings, in the descending colon and the ascending colon was dilated with water-soluble feces. Therefore, these diagnostic results strongly suggested a LBO, caused by a FI, in the descending colon.
The cause of the colonic obstruction was laxative pretreatment for colonoscopy, which was characterized by marked dilatation of the ascending colon lumen. Hywel reported that the maximum diameter of the lumen of the ascending colon, in normal patients, is on average 5 cm. 10 In the present case, US showed that the ascending colon was maximally dilated to maximum internal pressure, because the lumen diameter was more than 5 cm. One reason for this may be that physiologically, the hepatic flexure is bent as it runs from dorsal to ventral, and the transverse colon is potentially prone to gas retention. A curved-array ultrasound transducers was used in the present study to allow wide-angle observation in the colon lumen. It is important for the US images to not only display reflections from the anterior surface of the intestine but also within the entire colonic lumen. 11
The sigmoid colon, in the pelvic cavity, runs a complicated course and is frequently poorly visualized due to the presence of intestinal gas. In addition, the transverse colon is not easy to observe because of individual differences in the position of the colon. Conversely, the ascending colon can be easily detected by US because it is anchored to the retroperitoneum. Therefore, evaluation of the dilated lumen diameter of the ascending colon may be an indirect indicator of colonic obstruction. Furthermore, US is a very useful diagnostic tool and can be easily performed at the bedside, for follow-up observation, after treatment for constipation.
This case study highlighted several limitations of US for diagnosis of a fecal ileus. The major limitation was that constipation can lead to stagnation of gas in the intestinal tract, which can be difficult to observe. A second limitation was that, in US-detected dilated colon, it is necessary to consider stricture due to colorectal cancer since this is the most common cause of colorectal obstruction. A third limitation with US is its dependence on operator skill and technique. The standard treatment for a FI, is an enema and osmotic laxatives, as effective treatments. However, in severe cases, more invasive alternatives, such as surgery or endoscopy may be required. 12
Conclusion
In conclusion, this case report of a LBO, which was caused by a FI, was characterized by the use of sonography. The US images were helpful in documenting the presence of crescent-shaped acoustic shadows with haustrations and strong hyperechoic area, in the descending colon, and the ascending colon was dilated by water-soluble feces.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.