
Abstract
This case study examines a patient with severe hydronephrosis caused by ureteral obstruction, secondary to ovarian serous carcinoma. Gynecologic malignancies, especially advanced ovarian carcinoma, are common extrinsic causes of obstructive hydronephrosis. Sonography is a valuable modality to visualize the kidneys, diagnose hydronephrosis, and determine the grade of hydronephrosis. The treatment of hydronephrosis aims to remove the build-up of urine, prevent permanent kidney damage, and treat the underlying cause. Prolonged or severe cases of hydronephrosis can lead to acute kidney injury.
Hydronephrosis is a condition in which the kidney becomes enlarged, and its collecting system dilates. It is due to urine build-up from a failure of the excretion process and is caused by an obstructive or nonobstructive process. 1 Extrinsic causes of obstructive hydronephrosis include gynecologic malignancies and notably advanced ovarian carcinoma. There are approximately 42,000 newly diagnosed cases of hydronephrosis yearly, with a male-to-female prevalence of two-to-one. 2 Sonography is the imaging modality of choice when evaluating the kidney for pathology, such as hydronephrosis. 3 The presence and severity of hydronephrosis can be determined by evaluating the kidneys’ imaging features with renal sonography. This specific case study examines a patient with severe hydronephrosis caused by ureteral obstruction from an ovarian serous carcinoma. An ovarian mass can compress the ureter and prevent urine drainage from the kidney into the bladder. This results in urine building up in the renal collecting system. Ovarian cancer is rarely noted as the cause of obstruction, even though an ovarian mass is a common diagnostic finding, in the female population. 4 This type of urinary obstruction is underappreciated due to the unilateral nature of the ureteral obstruction. 4
Case Report
A 38-year-old female presented with a progressively worsening, nonproductive cough, and shortness of breath for the past month, as well as 2 days of hemoptysis. A physical examination of the patient prompted concern for a large mass extending from the pelvic floor to the level of the xiphoid process. The patient reported a decreased appetite in the past month but denied abdomen pain and distention. Her last menstrual period was 5 months prior with episodes of menorrhagia. She denied any urinary symptoms, including dysuria, hematuria, flank pain, changes in urine output, or appearance.
On the day the patient presented, an abdomen and pelvis computed tomogram (CT), without intravenous (IV) contrast, showed an intraabdominal/pelvic tumor measuring 30.3 cm x 24.5 cm x 17.3 cm. Additionally, the CT demonstrated severe bilateral hydronephrosis (See Figures 1 and 2). Extensive mediastinal lymphadenopathy, right lung atelectasis with a large pleural effusion, and bilateral obstructive hydronephrosis were seen. Due to the mass effect of the tumor occupying much of the abdomen and pelvis, as well as limited evaluation by single-phase CT and lack of IV contrast, the reproductive organs were not well visualized. It was suspected, at the time, that the tumor likely arose from the uterus and differential diagnoses included uterine malignancies, such as a leiomyosarcoma or malignant mixed Mullerian tumor.
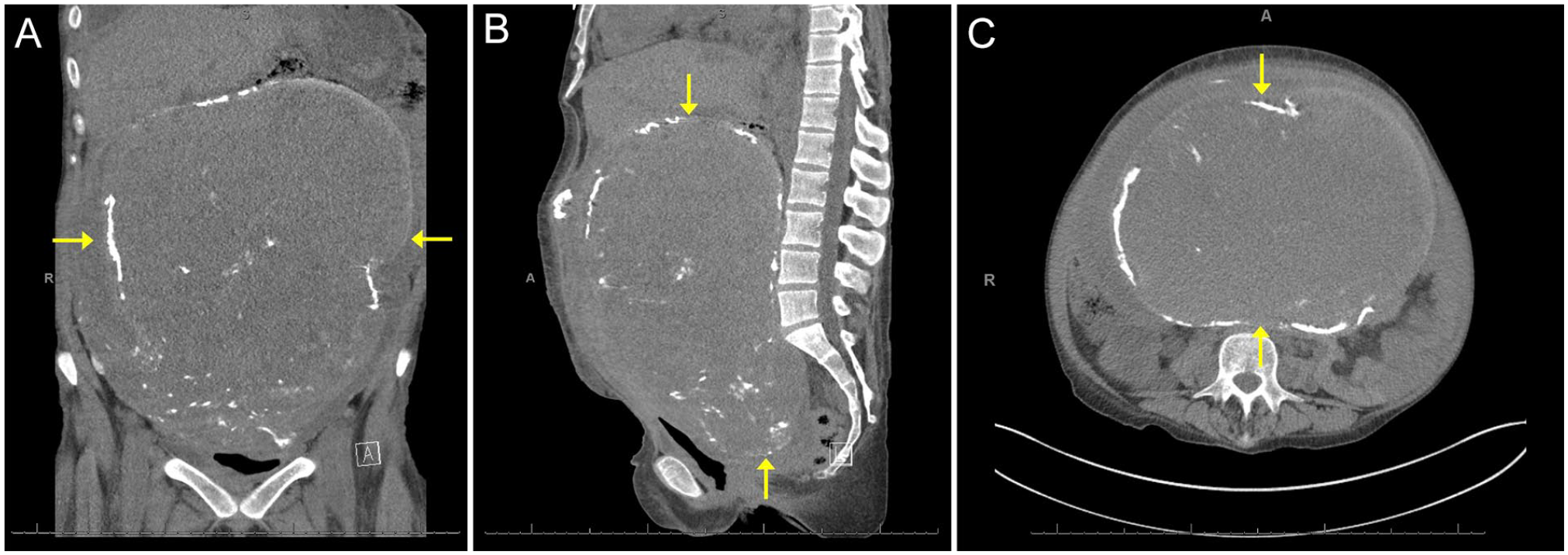
(A) Coronal computed tomographic (CT) image showing the ovarian serous carcinoma originating from the right ovary, (B) sagittal CT imaging showing the ovarian serous carcinoma, and (C) transverse CT image showing the ovarian serous carcinoma.

Coronal computed tomographic (CT) image showing bilateral kidneys with severe hydronephrosis and parenchymal atrophy, consistent with chronic obstructive uropathy.
Upon hospital admission, her potassium level was slightly elevated, creatinine was elevated, and sodium bicarbonate was depressed. These biomarkers were indicative of acute renal failure and mild hyperkalemia. A renal sonogram was performed the same day as the CT to further evaluate the hydronephrosis. The sonogram was completed using a Philips EPIQ 7 (Philips Medical, Bothell, WA) ultrasound equipment system and a 5-1 MHz curved linear transducer. The right kidney measured 13.1 cm x 4.1 cm x 7.0 cm and the left kidney measured 10.7 cm x 4.4 cm x 6.7 cm. The collecting systems, including the renal calyces, pelvises, and ureters, were severely dilated and the parenchymas were thinned. Both kidneys demonstrated severe hydronephrosis, parenchymal atrophy, and dilated ureters, which was consistent with chronic obstructive uropathy (see Figure 3). The urinary bladder was completely decompressed and suboptimally visualized.
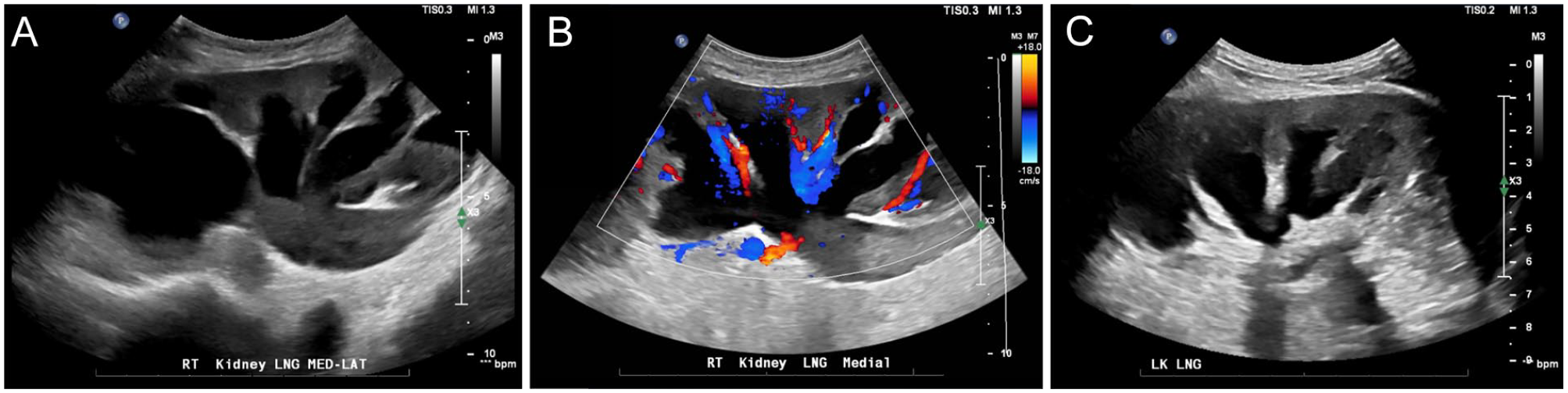
(A) Longitudinal sonographic image showing the right kidney with severe hydronephrosis and parenchymal atrophy, consistent with chronic obstructive uropathy, (B) longitudinal sonographic image showing the right kidney with color Doppler, and (C) longitudinal sonographic image showing the left kidney with severe hydronephrosis and parenchymal atrophy, consistent with chronic obstructive uropathy.
The day following the renal sonogram, bilateral percutaneous nephrostomy tubes were placed, leading to improved urinary output. Additional treatment included blood pressure maintenance to promote adequate renal perfusion, administration of 1300 mg of sodium bicarbonate twice a day for acidosis, and adherence to a renal specific diet. In the days following initial treatment, the patient had adequate urinary output from both nephrostomies and potassium, creatine, bicarbonate, phosphorus, and blood urea nitrogen (BUN) improved. Ten days after admission, surgical excision of the ovarian mass was performed along with a total hysterectomy and bilateral salpingo-oophorectomy. The mass originated from the right ovary and was found by pathology to be a low-grade serous carcinoma and was 31 cm x 29 cm x 25 cm in size, at the time of removal.
Postoperatively, the patient was counseled about an increased risk of acute kidney injury (AKI) due to acute blood loss anemia from surgery, hypotension, and postoperative non-steroidal anti-inflammatory drugs (NSAIDs) usage. Prior to discharge, the patient’s potassium, creatine, and sodium bicarbonate improved, compared to admission. A 1-month follow-up renal sonogram showed markedly improved hydronephrosis bilaterally, compared to the initial renal sonogram, with areas of mild caliectasis remaining. An antegrade nephrostogram of the bilateral percutaneous nephrostomy tubes was also performed, which showed appropriately draining ureters. Mild pelviectasis and upstream dilation of the ureters were also visualized, with no focal filling defect or obstruction. Two months after treatment, the stents were removed. Sonography showed only mild fluid distention in both renal collecting systems, most significantly in the upper poles, likely related to patulous collecting systems from prior chronic obstruction (see Figure 4).
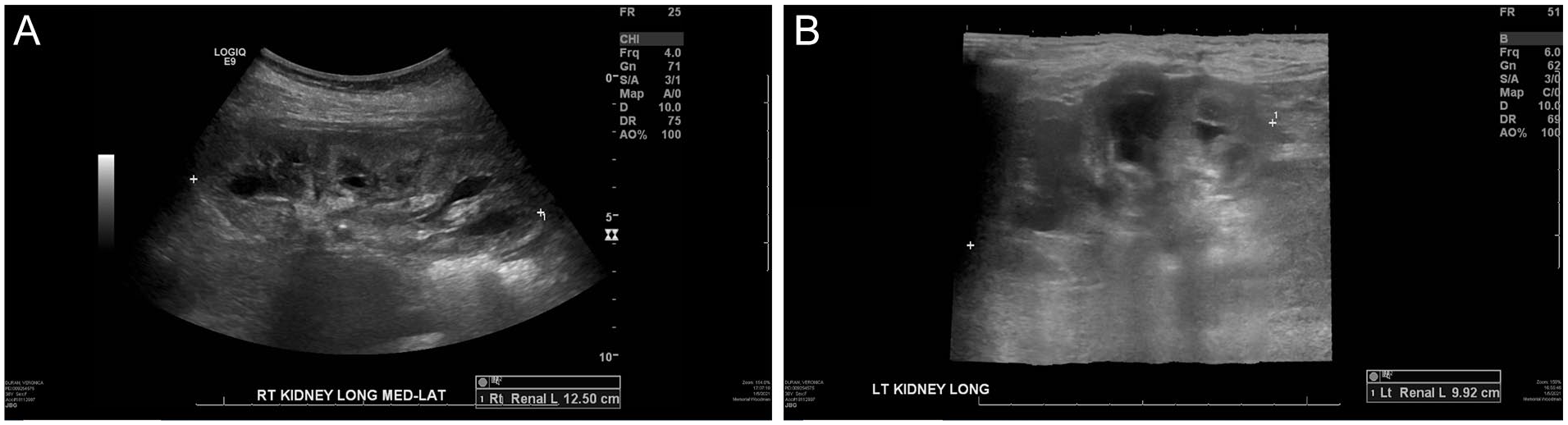
(A) Longitudinal sonographic image showing the right kidney after treatment with trace amounts of hydronephrosis and (B) longitudinal sonographic image showing the left kidney after treatment with trace amounts of hydronephrosis.
Discussion
The urinary system is composed of the kidneys, ureters, urinary bladder, and urethra. The kidney’s outer portion is the cortex, the inner portion is the medulla, and the medial portion is the renal hilum. The cortex contains nephrons, and the medulla contains collecting tubules that make up the pyramids. The urinary system’s primary function is to maintain body homeostasis by regulating blood volume, blood pressure, electrolyte balance, acid-base balance, and excretion of metabolic products and wastes. The nephrons carry out these functions; blood is filtered through the corpuscle, and water, waste, and urea continue to pass through the nephrons to form urine. Approximately 114 to 142 L of blood are filtered by the kidneys per day and produce approximately 1 to 2 L of urine. 5
Hydronephrosis is a condition in which the kidney’s pelvicalyceal system dilates when urine fails to drain normally into the bladder, building up in the renal collecting system. Failure of the urine excretion process is caused by an obstructive or nonobstructive process due to a functional or structural change of the urinary system. 1 The presentation of hydronephrosis can be unilateral or bilateral, physiologic or pathologic, and acute or chronic. 6
Each year, approximately 42,000 new cases of hydronephrosis are diagnosed with a two-to-one male-to-female prevalence. 2 Hydronephrosis occurs in all age groups and is the most common prenatal urologic condition. 7 It is more common in women in the age group of 20 to 60 due to pregnancy and gynecologic malignancy and is more common in men in the age group over 60 due to prostate disease.
There are many causes of obstructive hydronephrosis, which can be broadly classified as intrinsic or extrinsic. Causes of intrinsic obstruction include renal stones, renal cysts, ureteropelvic junction stenosis, ureter strictures, posterior urethral valves, neurogenic bladder, benign prostatic hyperplasia, and urologic malignancy. 6 Causes of extrinsic obstruction include peripelvic cysts, retrocaval ureter, trauma, retroperitoneal fibrosis, pregnancy, prostate abscess, and malignancy. 6 The majority of pediatric cases arise from anatomic abnormalities, including urethral valves or stricture and stenosis at the ureteropelvic or ureterovesical junction. 6 In adult cases, obstructive hydronephrosis is more common in males due to prostatic hypertrophy or malignancy. 6 In females, obstructive hydronephrosis is most often caused by pregnancy and gynecologic malignancy. 6 It is seen in up to 80% of pregnant women. 8
Hydronephrosis is a common complication of gynecologic malignancies, especially advanced ovarian carcinoma; however, the incidence is not known. 4 Ovarian serous carcinoma is the most common histologic type of tumor of the extrauterine female genital tract. 9 However, ovarian cancer is rarely seen as the cause of hydronephrosis because even though ovarian masses are common findings in the female population, obstruction is underappreciated due to the unilateral nature of the ovarian obstruction. 4 When the obstruction is due to ovarian masses, the patient may not become symptomatic until the disease advances to cause bilateral obstruction, which may be the first sign of progressive disease. 4
Hydronephrosis typically presents with acute urine retention. 10 In addition, clinical symptoms include urinary urgency, frequent urination, incomplete urination, change in urinary voiding, enuresis, hematuria, dysuria, as well as flank, abdominal, or groin pain, fever, infection, nausea, and vomiting.11,12 In general, symptom severity is dependent on the type, cause, and severity of the blockage. 13 However, some patients may remain asymptomatic. 14 The most common symptom is constant, dull flank pain due to stretching of the renal capsule; intermittent episodes of severe pain accompany this due to increased pressure from transient genitourinary peristalsis.
Sonography is a valuable imaging modality to visualize the kidneys, diagnose hydronephrosis, and determine the grade of hydronephrosis. The renal cortex, medulla, and collecting system of normal, healthy kidneys have different sonographic characteristics and can be differentiated on a renal sonogram. The cortex is isoechoic to the liver, and the medulla is hyperechoic compared to the cortex. The collecting system is not typically visualized. Sonographically, dilation of the collecting system is seen as distended, anechoic areas branching from the renal sinus to the renal cortex.15,16
Hydronephrosis is graded on a scale from 0 to 4, 4 being the most severe, indicating increased renal cortex damage and decreased renal function.1,7 The severity of hydronephrosis can be determined by evaluating the kidneys’ sonographic features on a renal sonogram. Grade 0 is an absence of hydronephrosis in the collecting system and is visualized as normal-appearing kidneys. 17 Grade 1 is characterized by a mildly dilated area solely within the renal pelvis and is visualized as anechoic branching in the renal pelvis. 17 Grade 2 is more extensive with pelvic and partial calyceal dilation and is visualized by moderate dilation of the renal pelvis, the pelvicalyceal pattern is retained, and the cortex remains unaffected. 17 Grade 3 contains dilated renal pelvis and all calyces and is visualized when the pyramids become flattened and the calyces out-pouch into the parenchyma, but the appearance and thickness of the renal cortex remain within normal limits. 17 Grade 4 hydronephrosis is characterized by severe dilatation of the renal pelvis and all calyces and is characterized by a ballooning appearance of the renal pelvis and calyces, thinning of the renal parenchyma, and loss of cortico-medullary differentiation. 17
Differential diagnoses include an extrarenal pelvis, parapelvic cyst, and prominent renal vasculature. An extrarenal pelvis is an anatomic variant where the majority of the renal pelvis is located outside the renal sinus and is larger than an intrarenal pelvis. Sonography will show an anechoic area adjacent to the renal sinus. It can be differentiated from hydronephrosis because the fluid does not extend into the calyces. A parapelvic cyst is a fluid collection in the renal sinus which does not communicate with the renal collecting system. It appears as an anechoic mass with well-defined borders within the renal sinus. It can be differentiated from hydronephrosis because the fluid within the parapelvic cyst does not communicate with the fluid in the collecting system and it has a more spherical shape. Prominent renal vasculature appears as dilated, anechoic areas within and adjacent to the renal sinus. It can be differentiated from hydronephrosis by utilizing color Doppler to demonstrate blood flow.
Sonography is the imaging modality of choice when evaluating the kidneys for pathology. 3 Renal sonography can evaluate the kidneys and renal collecting system, including renal vasculature and ureteral jets. 18 Sonography is inexpensive, noninvasive, uses non-ionizing radiation, requires little preparation, dynamic, and time-efficient. 11 In addition, it is instrumental in diagnosing radiosensitive patients, such as children and pregnant women. 19 Compared with CT, renal sonography performed by emergency physicians had a sensitivity of 80%, a specificity of 83%, and overall accuracy of 81%. 20 Therefore, sonography is a valuable modality for detecting hydronephrosis, but image quality is very operator-dependent. 20
The urinary tract can also be examined with CT urography. 3 This method examines the kidneys, ureters, and bladder with IV contrast administration. 3 The upper urinary tract is assessed first with the enhancement of the parenchyma during the parenchymal phase; the lower urinary tract is assessed second as the contrast is excreted through the collection system during the excretory phase. 3 Non-contrast CT can also assess the kidneys and is especially useful in detecting renal tract calculi or calcifications. 3 CT provides high-quality image resolution, a short examination time, and excellent visualization of structures, with contrast. 3
Blood and urine tests may also be utilized to support the diagnosis of hydronephrosis, discover the cause, and determine its effect on renal function. Renal function, complicated by severe hydronephrosis, deteriorates, and complicates the management of fluids, electrolytes, and acid-base mechanisms. 10 The kidneys may fail to complete their essential functions, which will result in anuria, uremia, metabolic acidosis, as well as hyperkalemia and elevated creatinine, as seen in the case report. 10
The prognosis of hydronephrosis depends on how quickly the obstruction is relieved. 6 When hydronephrosis is acute, renal function can completely recover if the obstruction is relieved. 6 When the obstruction is not relieved for an extended period, ischemic and inflammatory factors can permanently damage the kidney through cortical atrophy, intense fibrosis, and scarring, resulting in renal function loss. 6 Prolonged or severe cases of hydronephrosis can lead to AKI. 21 AKI secondary to obstructive hydronephrosis accounts for approximately 5% to 10% of all AKI cases. 21 When renal function is lost, there is an accumulation of waste products, impairment of sodium reabsorption, and disruption of acid-base balance leading to metabolic acidosis. 6
There are two main treatment options for removing the build-up of urine, including antegrade ureteric stent insertion and percutaneous nephrostomy tube placement. 22 Both options treat hydronephrosis and prevent deterioration of renal function. 22 The etiology of the obstruction determines which method should be utilized. 22 When the obstruction is due to malignant or benign etiologies, it is often challenging to determine the ideal option for urinary decompression. 22 In malignant disease cases, urinary drainage is performed for symptomatic relief and maintenance of renal function, facilitating systemic therapy initiation. 22 Other general treatment measures are used to promote renal function, including volume support, prevention of hyperkalemia and metabolic acidosis, and medication adjustments.
It is essential to evaluate and correct the underlying cause of hydronephrosis to prevent ongoing obstruction and progressive decline in renal function.7,23 Early surgical intervention is preferred for patients with severe hydronephrosis, especially when the obstruction is malignant in origin.7,23 When the treatment aims to relieve urinary obstruction, the pressure is alleviated in the pelvicalyceal system, and AKI can be reverted simply by unblocking the obstruction of urine flow. 10
Hydronephrosis can resolve independently; however, treatment is often required to prevent progressive renal damage and failure. Without treatment, the obstruction, and thus the hydronephrosis, may resolve on its own. However, when the obstruction is due to a malignant mass, hydronephrosis cannot resolve without intervention and increases in severity. When hydronephrosis is unilateral, patients typically are asymptomatic and do not require immediate treatment as a result of a compensatory response from the unaffected kidney.
AKI is characterized by an acute decrease in renal function.24,25 Intervention is important to promote immediate renal recovery as this is associated with rapid reversal of AKI. 26 Delayed or ineffective treatment and AKI is associated with progression to chronic kidney disease, cardiovascular events, and long-term morbidities. 27 AKI is typically managed with renal replacement therapies, aiming to maintain volume, electrolytes, acid-base, and uremic solute homeostasis. 28 Treatment options include dialysis or renal transplant.
When hydronephrosis is the only consideration, patients may have a complete recovery when treated with a urinary decompression technique. However, in cases of obstruction secondary to advanced malignancies, patients often have poor life expectancy despite urinary obstruction relief. 22 Urinary decompression may only be indicated if improvement in renal function will alleviate symptoms and facilitate systemic therapy. 22 Following treatment with ureteral stents or percutaneous nephrostomy tubes, quality of life can be affected due to irritative and urinary symptoms, pain, and frequent tube changes. 22 Ultimately, all treatment decisions should be made on an individual basis with a multidisciplinary approach involving the patient, their family, and their treatment team. 22
Conclusion
Hydronephrosis is a common complication in gynecologic malignancies, especially advanced ovarian carcinoma. Sonography is a valuable modality to visualize the kidneys and diagnose hydronephrosis and determine the grade of hydronephrosis. The grade of hydronephrosis is determined by the degree of dilation of the collecting system and parenchymal atrophy. Assessment of the severity of hydronephrosis and identifying obstructive pathologies, including ovarian carcinomas, can aid in determining the correct treatment plans.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.