
Abstract
Malakoplakia, a rare acquired granulomatous disease, affects many systems, including the urogenital tract. The literature describes malakoplakia of different viscera, and satisfactory results have been obtained after treatment. We reported a 48-year-old patient with diabetes who received multiple treatments in our hospital for bladder malakoplakia near the ureteral orifice. Despite aggressive treatment, the patient had recurrent bladder malakoplakia and even developed right ureteral orifice stenosis, which resulted in urinary obstruction and hydronephrosis. We believe that malakoplakia in the bladder near ureteral orifice should receive more attention. Satisfactory results may not be obtained through antibiotic treatment alone, and early antibiotic therapy combined with full surgical excision may be a better choice.
Keywords
Introduction
Originally defined by Michaelis and Gutmann, 1 the etiology of malakoplakia is believed to be related to macrophage dysfunction. As an extremely rare granulomatous disease with an infectious etiology, malakoplakia can manifest as nodules, plaques, or ulcers. 2 With a variety of clinical manifestations, malakoplakia can easily be mistaken for a malignant tumor of the corresponding organ depending on the location of the disease, and it can affect any part of the body. Regarding urinary system involvement, the most common location is the bladder, followed by the renal parenchyma and rarely the ureters. 3 Malakoplakia often affects people with low immune function, resulting a difficult clinical diagnosis. The imaging characteristics of the disease are similar to those of malignant tumors. The diagnosis of malakoplakia mainly depends on histopathological examination. At present, malakoplakia has been widely reported globally, and satisfactory are achieved results after treatment.4,5 We have reported a 48-year-old man with a histopathological diagnosis of bladder malakoplakia as a particularly rare case of malakoplakia in China that invaded both the bladder near ureteral orifice and the ureter.
Case report
In 2015, the patient visited to our hospital for frequent and urgent urination, right lumbago swelling pain, and lower abdominal discomfort. The patient had a 2-year history of diabetes, no history of other diseases, and no travel history in the epidemic area. The results of laboratory analysis were as follows: erythrocyte sedimentation rate, 98.00 mm/hour; creatinine, 123 µmol/L; leukocyte, 3+; and urine occult blood, 3+. A urinary bacterial culture revealed extensive growth of Escherichia coli. Computed tomography (CT) revealed severe hydronephrosis of the right kidney with new organisms on the right lateral wall of the bladder and invasion of the right ureteral orifice. Magnetic resonance imaging revealed a slightly higher signal of the mass in the T1 fat suppression sequence (Figure 1). The diagnosis was a bladder mass (Figure 2). After providing informed consent, the patient underwent histopathological biopsy. Histopathological examination of the excised tissue revealed a large number of eosinophils and foam cells containing the Michaelis–Gutmann body. Then, the patient underwent the transurethral bladder mass resection and right ureteroscopy (Figure 3). To prevent right ureteral stenosis, a right ureteral stent was inserted. During the operation, we observed obvious congestive edema on the right wall of the trigonometric region of the bladder and multiple granulosa protrusions on the mucosal surface of the bladder, and the right ureteral orifice was extremely difficult to find (Figure 4). The results of drug susceptibility testing illustrated that the bacteria were resistant to macrolides, quinolones, and most penicillins. Routine anti-infective treatment was applied using the only effective antibiotic tazobactam. One month after the operation, the patient recovered, and the right ureteral stent was successfully removed. However, 6 months later, the patient return to our hospital for frequent urination, urgent urination, lumbago, and abdominal swelling pain and discomfort. CT examination of the abdomen revealed severe hydronephrosis of the right kidney and space-occupying lesions of the right lateral wall of the trigonometric region of the bladder. Considering the possibility of recurrence of the patient’s bladder lesion, the patient again underwent transurethral bladder mass resection and right ureteral stent insertion. Thereafter, the patient underwent the transurethral bladder malakoplakia resection and right ureteral stent replacement almost every 3 to 6 months. In August 2019, considering the recurrence of malakoplakia, we performed a wider and deeper excision of the mass during the operation, which was apparently effective. To date, the patient has experienced no recurrence of malakoplakia, and he has undergone transurethral right ureteral stent replacement every 6 to 12 months.

Computed tomography features of malakoplakia. Arrows denote the right bladder lesion.
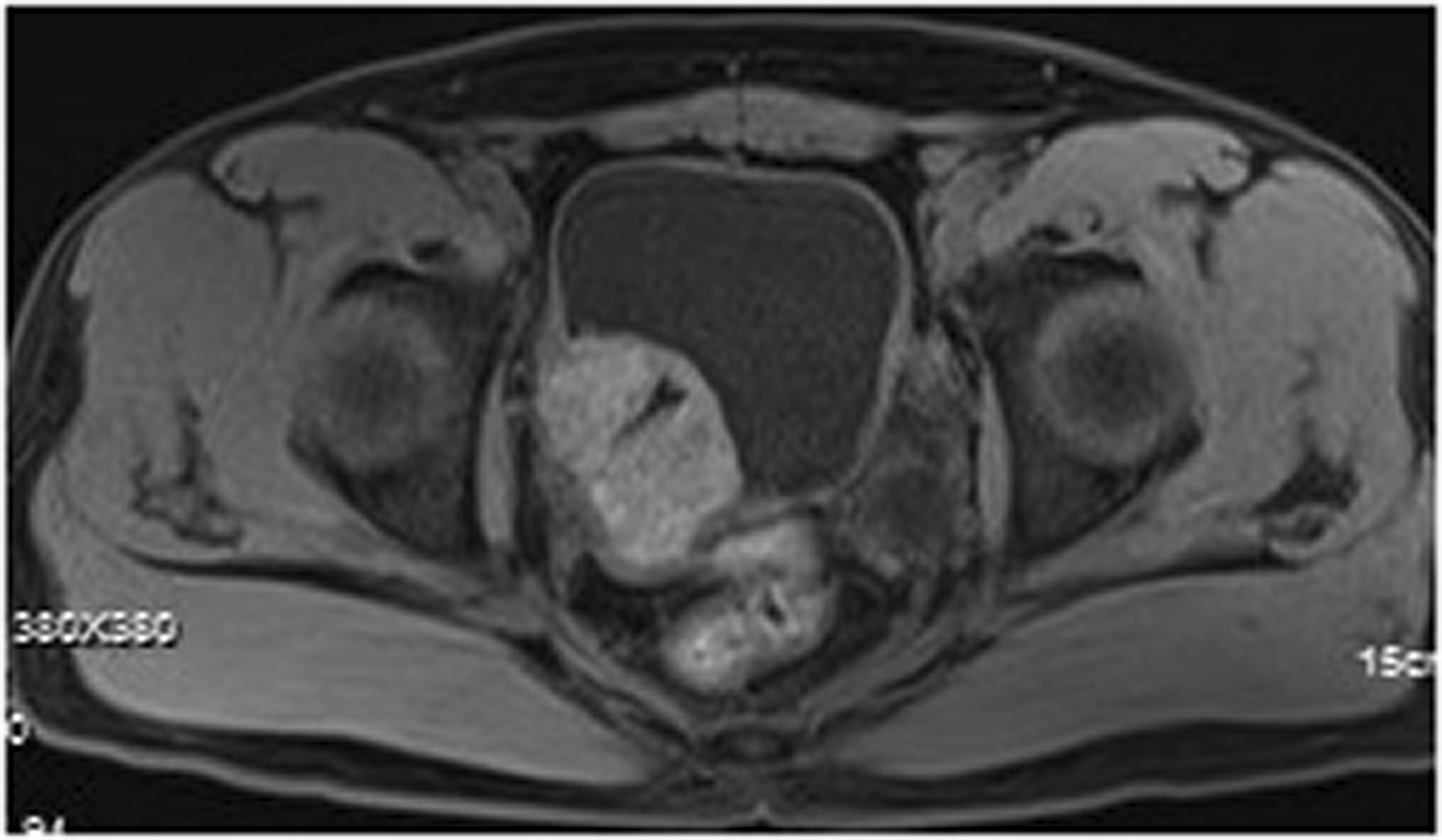
Magnetic resonance imaging features of malakoplakia. Arrows denote the slightly higher signal of malakoplakia in the T1 fat suppression sequence. The ureteral stent tube was completely encapsulated by malakoplakia tissue.

Histologic features of the surgical specimen. Arrows denote eosinophils and foam cells contained Michaelis–Gutmann bodies.

Appearance under a cystoscope. Arrows denote the granular tissue protruding from the mucosal surface of the bladder.
The reporting of this study conforms to the CARE guidelines. 6 Ethics Committee approval was not necessary because this was a case report and specific information about the patient was not included in the report. This study was based on a clinical case, and the patient provided verbal consent for publication of the examination images.
Discussion
This paper reports a case of bladder malakoplakia near the ureteral orifice in a patient in China. Imaging and histopathological examination confirmed the diagnosis.
Malakoplakia, a rare form of granulomatous inflammation, affects several organs in the body, most commonly the bladder. 7 The clinical manifestations and imaging findings of malakoplakia of the bladder are similar to those of bladder tumors. The diagnosis mainly depends on pathology, 8 with lesions being mostly located under the mucosa. Microscopically, in the background of chronic inflammation, there were many tissue cells and abundant cytoplasm and eosinophils, among which the Michaelis–Gutmann corpuscles scattered about the target or owl’s eye had a low value-added index. Special staining revealed positivity for Periodic acid–Schiff staining (glycogen staining) and fecal staining, and this patient was diagnosed with malakoplakia according to the histopathological findings.
Currently, there are no clear guidelines for the treatment of malakoplakia. According to the literature, the prognosis of malakoplakia in all organs after treatment is good. The main treatment method is anti-bacterial treatment, and the treatment effect of compound sulfamethoxazole and quinolone therapy or combined trimoxazole and rifampicin is better. When conventional drug treatment is ineffective, surgical treatment may be recommended, together with postoperative anti-infective treatment. In addition, another treatment strategy is immunotherapy. Cholinergic drugs (chlorocholine, aminoacylcholine) and vitamin C (improves the function of phagocytosis) are more effective when combined with antibiotics. However, for this patient, we immediately performed aggressive surgical treatment and sensitive antibiotic treatment after diagnosis, but the patient soon experienced relapse. Considering that our patient’s bladder malakoplakia invaded the right ureteral orifice, treatment was relatively more difficult. To avoid severe ureteral opening stenosis and injury, the scope of our surgery was limited, leading to repeated recurrence of bladder malakoplakia. In August 2019, we conducted a more thorough resection of the lesion, the scope of resection was wider, and the depth of resection reached the lamina propria of the bladder. Combined with antibiotic treatment, the patient did not experience relapse. Regarding the stenosis of the right ureteral orifice in the patient, which was irreversible, we chose ureteral stent placement to relieve hydronephrosis and prevent renal dysfunction. The stent should be replaced every 6 months.
In summary, the diagnosis of bladder malakoplakia is not difficult in combination with typical histopathological features. Attention should be paid to its differentiation from bladder tumors. In addition, as we have reported, bladder malakoplakia near the ureteral orifices should be of more concern to clinicians. Satisfactory results may not be obtained through antibiotic treatment alone. Early antibiotic therapy combined with full surgical excision and ureteral stent placement may represent a better choice.
Footnotes
Acknowledgement
We thank the patient for granting permission to publish this information.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.