
Abstract
Objective:
Various indices have been introduced for estimating sonographic gestational age and have demonstrated varied diagnostic accuracy. The aim of this study was to evaluate the correlation of fetal kidney length (FKL) with some other traditional measurement parameters in determining an accurate gestational age.
Materials and Methods:
In this prospective study, healthy pregnant women, who had completed a scheduled and routine obstetrical sonogram, were included. During the sonogram, the measurement indices, biparietal diameter (BPD), abdominal circumference (AC), crown rump length (CRL), head circumference (HC), femur length (FL), and FKL were analyzed. The obstetrical measurements had been taken every 4 weeks from the 20th week of the pregnancy, until the end of the pregnancy (e.g., 20th, 24th, 28th, 32nd, 36th, 40th weeks). After data collection, the measurement data were analyzed with SPSS software.
Results:
There were significant (P < .05) high strength of associations between FKL and the routine measurements of BPD (r = 0.668), AC (r = 0.770), CRL (r = 0.792), HC (r = 0.791), and FL (r = 0.803).
Conclusion:
These results suggest possible significant positive relationships between FKL and BPD, AC, CRL, HC, and FL. It can be assumed that FKL might be a suitable index for determining gestational age especially in the late second and third trimester, when other measurement indices are less accurate.
One of the most important duties of an obstetrician is to calculate the gestational age (GA) precisely which makes the essential maternal care possible. 1 Failing in this duty can be associated with perinatal morbidity and mortality caused by pre-maturity or post-maturity. The accurate calculation of gestational age is even more crucial in the case of a high-risk pregnancy, where termination may be considered, in order to prevent maternal complications. 2 Conversely, proper interpretation of specific diagnostic tests such as a serum assay, amniotic fluid assay, and chorionic villus sampling would only be possible, given the proper gestational age. 3 The traditional method of expected date of delivery (EDD) calculation, using the date of the last menstrual period (LMP), can be associated drawbacks, especially in cases where the LMP is unsure, there were irregular menstrual cycles, or first trimester bleeding. 4 Sonography has made tremendous improvements in establishing GA, over the last two decades. There are a number of different biometric measurements which are used in sonographic gestational age calculation such as measuring the biparietal diameter (BPD), abdominal circumference (AC), crown rump length (CRL), head circumference (HC), and the femur length (FL). All of these gestational age measurements can be limited by conditions such as a breech fetal presentation, oligo/polyhydramnios, intrauterine growth restriction (IUGR), and multiple gestation.5,6 In addition, in later stages of pregnancy these parameters are no longer reliable because of the biological variability of size in relation to age, which makes it difficult to determine an accurate GA, in the second and third trimesters. This is mostly important in cases where the women are referred later for maternal-fetal care or are not sure of their LMP. These types of situations make the need for obtaining accurate sonographic gestational indices very important.7,8
The fetal kidneys become more and more hypoechoic after 9 weeks of gestation, and it is reported that in 80% of patients it can be seen at 11 weeks of gestation, while in 93% of patients, the fetal kidneys were observed at 13 weeks of GA. 9 Despite the fact that the growth of fetal kidneys can be affected by genetic variations, as well as other organs, and can alter the transverse and anteroposterior renal diameters, while leaving the fetal kidney length (FKL) unaffected. Therefore, the FKL may be an optimal measurement parameter for evaluating gestational age, even among fetuses that are deemed small for gestational age (SGA). 10 The aim of this study was to evaluate the correlation of FKL with other traditional obstetrical measurement parameters, to determine an accurate GA.
Materials and Methods
This prospective study was done after being confirmed by the ethics committee of Zahedan University of the Medical Sciences, at Bou Ali Hospital. This study included healthy pregnant women, who had completed a scheduled and routine obstetrical sonogram, during their pregnancy. Fifty pregnant women were chosen by consecutive sampling, according to the study’s inclusion criteria. The study’s inclusion criteria were as follows: the subjects were certain of their LMP, scheduled a sonogram during their first trimester, GA was between the 20th and 40th weeks, and provided an informed written consent. The exclusion criteria for this study were as follows: any detected fetal congenital anomalies, IUGR, SGA, a fetal renal function disorder, twining or multiple fetuses, and maternal complications, such as preeclampsia and gestational diabetes.
All of the consented patients had undergone a first trimester sonogram and the data regarding the fetal CRL was available. The true GA was calculated based on the LMP and the first trimester sonogram, given that the CRL is considered the measurement gold standard. All the sonograms were performed by an experienced radiologist, using a real-time ultrasound equipment system and a curvilinear transducer, which had a bandwidth frequency of 3.5 to 5MHz.
During the fetal biometry, the indices of BPD, AC, CRL, HC, FL, and FKL were analyzed. All of the ultrasound equipment systems, used to conduct fetal biometry, had quality control verified as well as the transducers checked and electronic calipers verified. The study scanning protocol began with imaging the fetus in the transverse plane. Next the transducer was rotated into a longitudinal axis once the fetal kidney was observed (see Figure 1A–C). The FKL was measured from the outer edge of the upper pole to the outer edge of the lower pole. 11 The obstetrical measurements were taken every 4 weeks from the 20th week of the pregnancy, until the end of the pregnancy (eg, 20th, 24th, 28th, 32nd, 36th, 40th weeks).
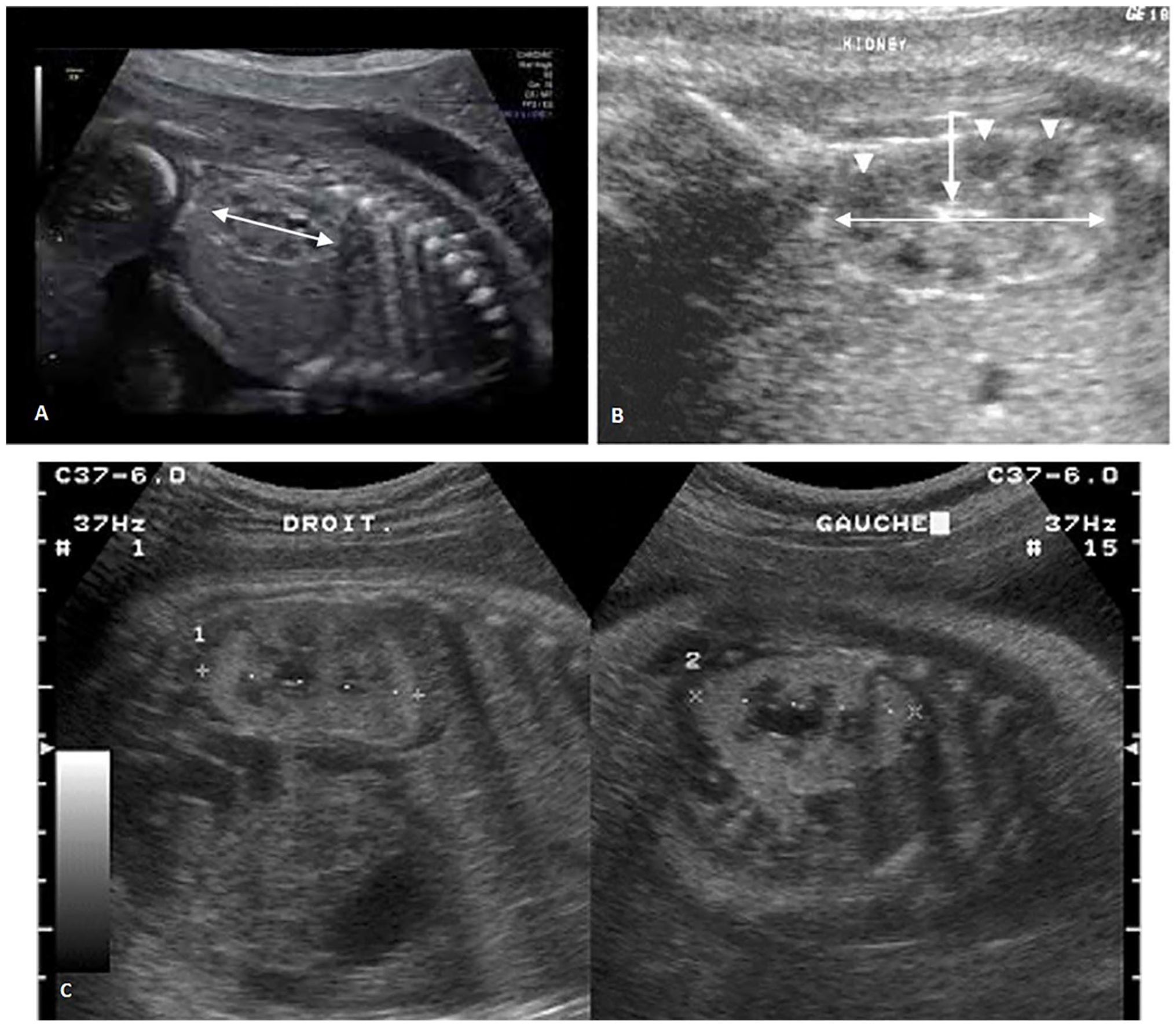
(A) Sonographic longitudinal view of a fetal kidney measuring 35 mm, at 30 weeks gestational age. The well-outlined border of the fetal kidney and the normal renal pelvis can be visualized. (B) Sonographic longitudinal view of a fetal kidney measuring 30 mm at 36 weeks gestational age (arrow: sinus fat and arrowhead: medulla). (C) Sagittal view of a fetus’s right and left kidneys at 24 weeks gestational age.
Different Gestational Measurement Parameters
Each of study variable was measured three consecutive times and the average of the three measurements was considered as the final measurement. The BPD was measured in the axial plane, which transverses the thalami, and cavum septum pellucidum. 5 Measurement of the AC was made by rotating around the axis of the bifurcation locus of the portal vein and stomach. 5 The CRL was determined as the longest direct measurement from the cephalic end to the rump region. The technique of obtaining various measurement and obtaining an average was done to add to the reliability of the results. 5 The HC was measured at the point where the fetal head had its largest area. The electronic calipers were placed at the external proximal edge of the fetal skull and extended to the internal edge, for all fetal head measurements. 5 The length of fetal femur was measured from the juncture point of femur bone as well as the cartilage and the bony part was measured. 5 After scanning the fetal kidneys in the transverse plane, the longitudinal axis of the kidneys was defined with the transducer rotated to their longest lengths. 12 All the gestational measurements were ultimately analyzed with IBM’s Statistical Package for the Social Sciences (SPSS) software. The qualitative data were expressed via percentages, and the quantitative data were expressed with means and ±standard deviations. For determining the correlations of the variables, a Pearson’s correlation coefficient was utilized. The level of statistical significance was set at an alpha of P < .05, which was considered significant.
Results
Fifty healthy pregnant women, who had completed a scheduled and routine obstetrical sonogram, were included. In this prospective study, the true GA was determined according to the LMP and the first trimester sonogram, in which the CRL is considered the measurement gold standard. The CRL was only measured during the first trimester. During fetal biometry, the indices of BPD, AC, HC, FL, and FKL were evaluated. The average age of the pregnant women was 26/96 ± 5/2. This study was done in order to consider the relationships between FKL and BPD, AC, CRL, HC, and FL, in this cohort of pregnant women. The strength of measurement relationships was determined with a Pearson’s correlation coefficient (the quantitative and normal data). The results of this statistical test are provided in Table 1. The results of Pearson’s correlation demonstrated that there were statistically significant and a strength of association between FKL and BPD, AC, CRL, HC, and FL. There was a positive and direct relationship which indicates that the longer the fetal kidney, the greater the measurement for BPD, AC, CRL, HC, and FL.
The Pearson Correlation Coefficients and P Values for Comparing Fetal Kidney Length to BPD, AC, CRL, HC, and FL.
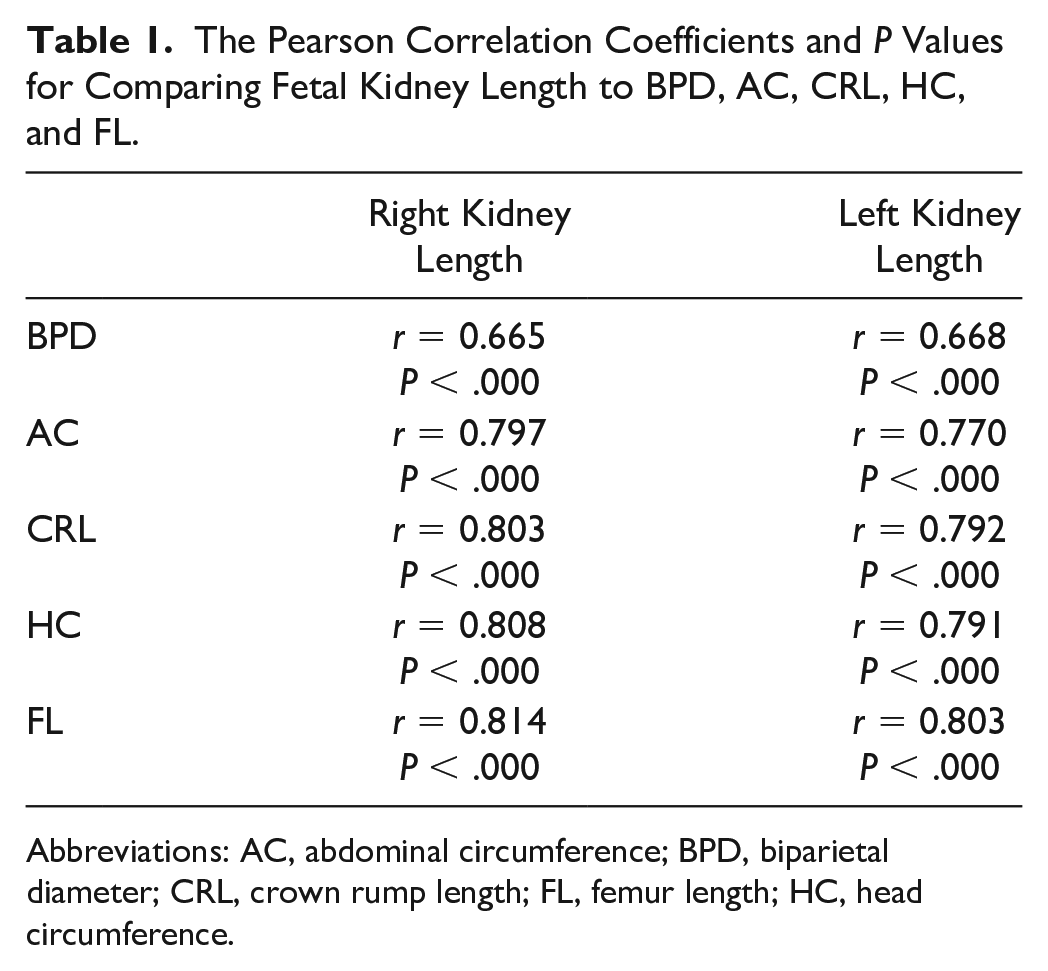
Abbreviations: AC, abdominal circumference; BPD, biparietal diameter; CRL, crown rump length; FL, femur length; HC, head circumference.
Discussion
The results of this prospective study would suggest that the observed strength of association between FKL and the BPD, AC, CRL, HC, and FL, in pregnant women, was significant bilaterally. The findings published by Peter et al were consistent with the present study and indicated a significant correlation between the GA, based on the traditional biometric indices, and the GA predicted based on FKL. 13 Also, Dash et al confirmed that there was a linear correlation between the FKL and GA, as the pregnancy progressed. 14 In another study, Munthaian et al demonstrated a very high strength of association (0.926) between the FKL for predicting GA, compared with other biometric indices. 15 The results of the present study support this premise and additionally found that the highest correlation coefficient existed between the comparison of FKL and FL.
In India, Kumar et al evaluated the sonograms of 99 healthy fetuses, every 2 weeks, during the 18th to 38th gestational weeks. In their findings, the 18th week of pregnancy was described as the best time for observing the fetal kidneys. In that study, the FL, FKL, and BPD, respectively, resulted in 3.85, 8.04, and 8.75 days in error, for calculating GA. 16 These results were very much comparable to the results of the present study.
A study by Shivalingaiash et al analyzed 60 healthy fetuses, during the 24th to 36th weeks of pregnancy and reported that FKL had a strong and significant correlation with GA, as well as other biometric indices. 6
It must be considered that due to the improvements in sonographic resolution that imaging different fetal organs in utero, especially kidneys, has been significantly improved. Using real-time high-resolution sonography has made it possible to identify fetal kidneys, more easily. However, even studies conducted by older and less accurate ultrasound equipment systems, such as the study by Cohen et al, indicated a strong correlation between FKL and GA. 17 In addition, the Cohen et al study reported a significant consistency between the GA estimated by FKL, compared with those estimated by other biometric indices. 17
In another study, Meenakshi et al used FKL accuracy in estimating GA, during the late third trimester. They indicated that the accuracy of BPD prediction in the third trimester can be improved from ±8.7% to only ±3.08 % by combining it with FKL. 18 In their study, Akram et al demonstrated that the FKL increased and correlated with the GA, measured in weeks, in the third trimester. 19
The nonsignificant difference between the size of left and right kidney in the present study was consistent with the results of Akram et al and Meenakshi et al.18,19 However, Edevbie et al reported a significantly higher length for the left kidney. However, the measurements in that study were only done once due to the cross-sectional design of the study. 20
Konje et al reported that the best GA predictors were BPD, AC, HC, FL, and FKL. The combinations of the above-mentioned indices showed ±8.57 days of differences in their GA prediction, while FKL added at most 1 day of accuracy, to the GA measurements. 21
According to the results of the present study, BPD, AC, CRL, HC, and FL had a close relationship with FKL. As FKL was also representative of GA, then it can be suggested that FKL might also be a useful predictor, specifically when used in later trimesters, as well as in combination with other biometry indices. The present study results were completely consistent with the results of Abonyi et al indicating that FKL measurements strongly correlated with GA. 11 A more recent article conducted by Singh et al compared the correlation between GA, transcerebellar diameter, and FKL. They reported a positive linear relationship between GA and both FKL (r = 0.87) and transcerebellar diameter (r = 0.97). 22 They also indicated a good correlation between these two methods. Another study by Fattah et al reported a correlation coefficient between GA and transcerebellar diameter. 12
Limitations
The present study had several limitations due to the research design and a convenient sample of patients. The sample also was based on a rather small number of patients. The sample size may not be large enough to draw definitive conclusions; however, this cohort study does suggest that there may be a direct correlation of FKL and GA when compared with other standardized biometry measurements.
Conclusion
This prospective cohort study results suggested possible significant positive relationships when comparing FKL to BPD, AC, CRL, HC, and FL. It can be assumed that FKL might be a suitable biometric index for determining GA specifically, in the late second and third trimester, when other measurements are less accurate. Conversely, when evaluating FKL, along with other indices, it may improve the accuracy of predicting GA.
Footnotes
Author’s Note
Jafar Noori is now affiliated to Radiology Department, Zabol University of Medical Sciences.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.