
Abstract
Objectives
Empirical determination of phenylalanine (Phe) tolerance in patients with phenylketonuria (PKU) relies on frequent assessment of blood Phe concentrations in relation to Phe intake from detailed meal records. This study aimed to determine Phe tolerance in twin pregnancies.
Methods
The reviewed cases included three women with PKU who each had a singleton and twin pregnancy (i.e., they were pregnant twice). All patients were under regular supervision to maintain Phe concentrations in a steady state and determine safe Phe intake. Restriction of Phe in the patient’s diet was determined depending on the amount of Phe intake, which allowed for stable blood Phe concentrations within the target range.
Results
In all three patients with PKU, the ratio of Phe tolerance during the course of the twin and singleton pregnancies was <1 for most of the pregnancy. The ratio of the increase in Phe tolerance between 29 and 34 weeks of gestation and that between 15 and 28 weeks of gestation was 0.66 and 1.17, 0.51 and 0.14, and 0.76 and 1.42 in the twin and singleton pairs of pregnancies, respectively.
Conclusions
Our study shows that Phe tolerance in a twin pregnancy is not greater than that in a singleton pregnancy.
Keywords
Introduction
Pregnant women with classic phenylketonuria (PKU, OMIM 261600) need appropriate management to avoid the teratogenic properties of elevated phenylalanine (Phe) levels. 1 A low-Phe diet is challenging for female patients of childbearing age, and they need a lot of support and education on treatment of PKU in pregnancy. Phe tolerance (mg/day) is defined as the amount of Phe in the diet that maintains blood Phe levels within the acceptable range. 1 , 2 Clinical determination of Phe tolerance relies on frequent assessment of blood Phe levels in relation to Phe intake from detailed daily food intake records. For optimal pre-conception care, stable blood Phe control within the therapeutic range of 120 to 360 µmol/L should be maintained before women with PKU conceive. 1 , 2 Phe intake should provide the minimum requirement for this essential amino acid needed to maintain physiological protein turnover for the current body mass of the mother and fetus. Notably, the guidelines for predicting changes in Phe tolerance during the course of pregnancy are not clear.
Twin pregnancies are becoming increasingly common in Poland and other Western countries. The lower birth weight and gestational age of twins compared with singletons are major factors contributing to twins’ relatively poorer early outcomes, as well as possible health complications in adult life. 3 Despite awareness of the possible coexistence of multiple gravidas and PKU in pregnant women, there have been few studies on twin pregnancies in women with PKU. 4 , 5 More precise data are required to document what may be considered as the “normal” range for Phe tolerance in twin and multiple pregnancies. Therefore, this study aimed to determine changes in Phe tolerance during the course of singleton and twin pregnancies in women with PKU.
Materials and methods
A retrospective review of singleton and twin pregnancies of patients with PKU was performed by examining dietary and medical records in the PKU Polyclinic in Warsaw. Inclusion criteria for the study were a medical diagnosis of classic PKU based on newborn screening, absence of comorbidities (e.g., hypertension, diabetes), and a full medical history of twin pregnancy on a low-Phe diet (see below) initiated before conception or during the first trimester. Gestational age is expressed as the number of weeks after the last menstrual period. Fasting blood Phe concentrations were measured from whole blood spots on filter paper cards by using tandem mass spectrometry (Sciex, Concord, Ontario, Canada). The blood target range for this amino acid was set at 120 to 360 µmol/L, according to national recommendations (Polish PKU Consensus, 2006). Phe concentrations, as well as written daily dietary records, were assessed at least twice weekly during pregnancy, with at least bimonthly clinic visits. Food records were analyzed to calculate the intake of Phe (mg/day). Body mass index (BMI, kg/m2) was defined as the individual’s body weight divided by the square of their height.
We implemented a diet restricting natural protein and supplemented it with Phe-free amino acid substitutes (Milupa PKU3 Tempora/Advanta, XP Maxamum, and PKU Lophlex LQ/Nutricia North America, Gaithersburg, MD, USA; PKU Cooler/Vitaflo International, Alexandria, VA, USA; Phenyl-free 2HP/Mead-Johnson, Chicago, IL, USA).
For this study, the IRB issued a waiver because the study was retrospective, and only anonymized data were used. Some data regarding the patients in the current study have been previously published in Polish. 6
Results
Three women with PKU (1.Q383X/R408W, 2.EX3DEL/EX3DEL, 3.R281L/R408W) had one singleton and one (dizygotic) twin pregnancy each (i.e., they were pregnant twice) and fulfilled the inclusion criteria. All patients were Caucasians of Polish origin. Table 1 includes descriptive characteristics of the pregnancies, birth measurements, and Phe concentrations. The mean age at conception was 27 ± 3 years. Only half of the pregnancies had a low-Phe diet initiated pre-conceptionally. The course of the pregnancies was normal in all six and they lasted at least 35 weeks. Patient 3 had severe nausea in both pregnancies between weeks 6 and 10. Patient 1 suffered from acute urinary infection in week 26 of her singleton pregnancy and viral gastroenterocolitis in week 19 of her twin pregnancy. Neonates had a normal birth weight. Only one neonate from the singleton pregnancy of patient 2 in whom a low-Phe diet was initiated in the second trimester had a relatively small head circumference. One of the twins of patient 3 was affected by hypospadias. Generally, the frequency of fetal abnormality in dizygotic twins is comparable with that of singleton pregnancies, and hypospadias does not belong to the clinical picture of so-called maternal PKU syndrome. 1 None of the neonates had PKU or any degree of persistent hyperphenylalaninemia.
Characteristics of pregnancies and offspring.

BMI, body mass index; Phe, phenylalanine; SD, standard deviation; F, female; M, male.
In five of the six pregnancies, there was high rate of Phe values above the recommended range during trimester 1 (Table 1). In all pregnancies, the mean Phe concentrations in the second and third trimesters were <360 µmol/L. In the second and third trimesters, the mean rate of undesirable low Phe concentrations (<120 µmol/L) was 44% and 17% respectively. Phe concentrations were below the reference range for healthy pregnant women (9% of Phe values) only in the third trimester of the twin pregnancy in patient 1. 7
All patients were under the regular supervision of the same metabolic dietitian (J.Ż.) to stabilize Phe levels and determine Phe tolerance. None of the pregnant patients was hospitalized in the first and second trimesters. General vitamins, including folic acid and mineral supplementation, were provided before and during pregnancy. A diet-restricting natural protein, which was supplemented with special low-protein foods and tyrosine-augmented Phe-free amino acid substitutes, was implemented. Synthetic protein was consumed at least three times daily because it is absorbed and oxidized more rapidly than intact protein sources. Fruit and vegetable consumption was restricted. The mean daily protein intake from amino acid supplement(s) and energy intake are shown in Table 2. High protein products of animal origin were introduced to the diet in singleton and twin pregnancies in weeks 13 and 12, 25 and 24, and 18 and 20 in patients 1, 2, and 3, respectively. When expanding the diet, the daily supply of Phe was calculated as 320 and 375 mg, 800 and 350 mg, and 540 and 420 mg, respectively. Whether energy requirements were met was assessed by monitoring weight gain.
Protein and energy intake.
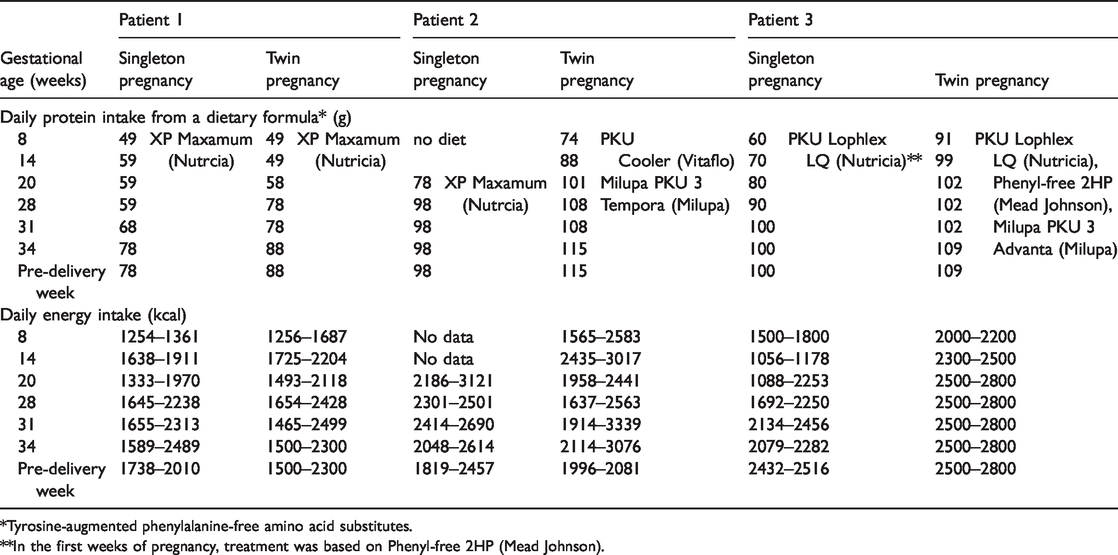
*Tyrosine-augmented phenylalanine-free amino acid substitutes.
**In the first weeks of pregnancy, treatment was based on Phenyl-free 2HP (Mead Johnson).
Table 3 shows Phe tolerance in singleton and twin pregnancies. The highest mean Phe tolerance in singleton and twin pregnancies was 1245 ± 230 mg and 989 ±294 mg, respectively. Figures 1–3 show Phe tolerance and energy intake plotted by gestational age in the three patients. In all three patients with PKU, the ratio of daily Phe tolerance during the course of twin to singleton pregnancies was <1 for most of pregnancy (Figure 4). In two mothers with PKU, who started on a low-Phe diet before conception or early post-conception, the ratio of the increase in Phe tolerance between 29 and 34 weeks of pregnancy to that in the second trimester was nearly two times higher in singleton pregnancies compared with twin pregnancies, despite the ratio of total birth weight of offspring between singleton and twin pregnancies ranging from 0.48 to 0.78 (Table 1). In patient 3, the highest third trimester Phe tolerance in twin pregnancy reached only 67% of the highest value in the singleton pregnancy. However, pre-conception Phe tolerance was the same for the singleton and twin pregnancies in patient 3 (Table 3). The ratio of increase in Phe tolerance in the third trimester to the birth weight of offspring (mg/g) ranged from 0.11 to 0.42 in singleton pregnancies and from 0.01 to 0.12 in twin pregnancies (Table 3).
Changes in phenylalanine tolerance.

Phe, phenylalanine; SD, standard deviation.
*The mean value was from 13 to 19 weeks of pregnancy according to Ennis et al. 13 who proposed intervals called early and late pregnancy. We adopted these intervals because of late implementation of a low-Phe diet from 15 to 19 weeks in the singleton pregnancy of patient 2.
**The mean value was from 33 to 39 weeks of pregnancy according to Ennis et al.’s 13 pregnancy intervals. This range was chosen because of different gestational ages at delivery from 33 to 38 weeks and from 33 to 35 weeks in the singleton and twin pregnancies of patient 1, respectively, from 33 to 37 weeks in the twin pregnancy of patient 2, and from 33 to 38 weeks and from 33 to 34 weeks in the singleton and twin pregnancies of patient 3, respectively.

Phenylalanine tolerance and energy supply in patient 1. (a) Singleton pregnancy and (b) twin pregnancy.

Phenylalanine tolerance and energy supply in patient 2. (a) Singleton pregnancy and (b) twin pregnancy.

Phenylalanine tolerance and energy supply in patient 3. (a) Singleton pregnancy and (b) twin pregnancy.
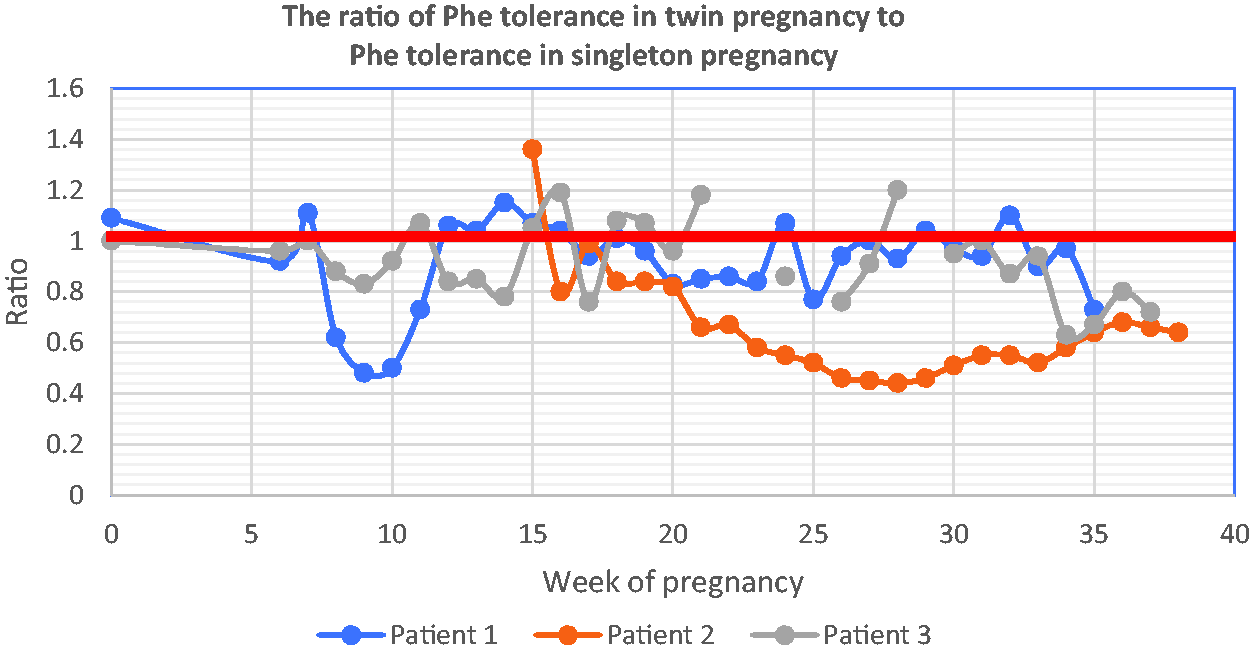
Ratio of phenylalanine tolerance in singleton to twin pregnancies. Phe, phenylalanine.
Discussion
In Caucasians, the highest population-based evaluation of the prevalence of PKU is up to 3 per 1000 births. 8 Pregnancy in women with PKU can be viewed as a successful outcome of survival and transition into adulthood, achieving as normal a life as possible. 9
Physiologically, in the first two trimesters of pregnancy, maternal anabolism predominates, while from approximately 30 weeks’ gestation, maternal catabolism with an accelerated breakdown of fat deposits is favored because of placental hormones and adipocytokines. 9 , 10 Anabolism is associated with increased Phe requirements. 1 With the exception of one twin pregnancy (patient 2), the lowest mean Phe concentrations were observed in the second trimester. However, mean Phe concentrations in the second and third trimesters were acceptable. In one pregnancy, blood Phe concentrations never rose >360 µmol/L (singleton pregnancy of patient 1). Interestingly, most Phe values <120 µmol/L were above the gestational age-dependent upper reference limits of Phe in whole blood for singleton pregnancies in healthy women, as recently analyzed by tandem mass spectrometry. 7 McBride and colleagues 7 showed that Phe levels declined from the first to the second trimesters and then remained relatively stable to the end of the singleton pregnancy. The optimal range of Phe concentrations of 120 to 360 µmol/L remains unknown. 11 , 12 There is sufficient evidence to warrant further investigation of phenylalanine concentrations and gestational age-specific phenylalanine reference ranges in twin pregnancies in healthy women to better understand homeostasis in multiple gestations in patients with PKU.
Recently, minimum daily Phe requirements per kg of body weight in the presence of excess tyrosine, which is in line with the treatment concept of our PKU cases, was experimentally determined using the direct amino acid oxidation technique in healthy women with singleton pregnancies by Ennis et al. 13 These authors showed that the minimum daily Phe requirement was 15 mg (95% confidence interval: 10.4–19.9 mg) in early pregnancy (13–19 weeks’ gestation) and 21 mg (95% confidence interval: 17.4–24.7 mg) in late pregnancy (33–39 weeks’ gestation). In early pregnancy, as well as in late pregnancy, our Phe tolerance estimates are consistent with data by Ennis and colleagues 13 only in patient 1. In the other patients, the estimated Phe tolerance was less than the minimum demand as calculated by direct amino acid oxidation.
The dominant view on Phe tolerance in the third trimester in treated maternal PKU is that its increase parallels accelerated fetal growth and uptake of Phe, as well as an increase in phenylalanine hydroxylase activity in the fetal liver. 1 , 2 , 9 Intriguingly, there was an unexpected comparable Phe tolerance in singleton and twin pregnancies in our study. Our dizygotic twin pregnancies are a powerful clinical model because in each patient the fetuses had similar birth weights without intrauterine growth retardation, while each twin had a distinct placenta in a similar maternal environment. Physiologically, there is little discordance in biometry between singletons and twins in the second trimester, but in the third trimester, growth in twins is consistently slower than that in singletons. 3 Phe tolerance may vary significantly, even between singleton pregnancies in the same patient, possibly at least in association with currently unrecognized maternal anthropometric factors and diet modalities. 1 , 14 , 15 In our cases, this hinders interpretation of the comparability of Phe tolerance between the singleton and twin pregnancies. Pre-pregnancy BMIs were different in the singleton and twin pregnancies of patients 2 and 3.
The European PKU Guidelines, 1 as well as the previous American College of Medical Genetics guidelines on PKU, 2 state that treatment should commence at pre-conception for maternal PKU. These guidelines also emphasize that considerable effort should be made to avoid any unplanned pregnancies, with precautionary advice taking into account individual cultural and religious backgrounds. Ford and colleagues 16 showed that women with PKU of childbearing age had anxieties about sex and may have had problems with religious or moral beliefs. All patients need to feel comfortable discussing pregnancy and their choices regarding contraception. 16 In our study, patient 2 had decided not to use contraceptives. In a recent Italian study by Caletti and colleagues 14 on Phe tolerance in women with PKU, 6 of 10 conceptions were unplanned. Therefore, in the future, we will develop two algorithms of care in maternal PKU. One algorithm will be preferred and supported by the evidence-based recommendation of a low-Phe diet introduced pre-conceptionally. 1 , 2 The other algorithm will be optional, with rapid and restricted dietary treatment introduced in early unplanned pregnancies, and will use daily care in outpatient clinics or hospitalization. Homeostasis of Phe changes in a twin pregnancy, with a low Phe diet beginning after conception appearing to be, to some extent, different compared with twin pregnancies with a diet introduced pre-conceptionally. Notably, among our patients, the highest rate of Phe values exceeding the upper limit of the ideal target range in the first trimester was observed in a twin pregnancy with a low-Phe diet that was not initiated pre-conceptionally (patient 2). Medical professionals should attempt to close the gap between women with PKU of childbearing age of different religious beliefs, which affect pregnancy planning, and the programs of care that are available. 16
The current study has notable strengths. The patients with PKU were ethnically homogeneous and under regular supervision of the same metabolic dietician. The study also has certain limitations that need to be taken into account. In twin pregnancies, the incidence of preterm delivery before 38 weeks can be up to 50%. In our study, the number of pregnancies was limited and the length of pregnancy varied (35–40 weeks). A low-Phe diet was introduced pre-conceptionally in only half of the patients. The sex of the offspring in every pair of singleton and twin pregnancies was not concordant. A further limitation to be taken into account in this study is its retrospective design. Diet compliance in twin pregnancies may be affected by the need to care for the children from the preceding singleton pregnancies and the transition of support networks. 17 , 18 We also cannot rule out the effect of other factors, such as viral infections and other stressors. Moreover, birth data were used as a surrogate for the lack of placental data.
There are still many gaps in our knowledge regarding normal and abnormal physiological changes and effective interventions in multi-fetal pregnancies. The physiology of a twin pregnancy appears to be fundamentally different from that of a singleton pregnancy. Several reports have shown surprisingly different effects of disturbances in metabolism (e.g., gestational diabetes mellitus) on singleton and twin pregnancies. 3 , 19 A study by Wang and colleagues 20 showed disruption of the Phe and tyrosine biochemical pathways in twins with intrauterine growth retardation. Multiple gestations are increasing in frequency because of a number of factors, including assisted reproductive techniques and increasing maternal age. Therefore, medical providers dealing with PKU need to develop a detailed appreciation of the pathophysiological differences and subsequent challenges of managing maternal PKU in multi-fetal pregnancies.
Footnotes
Acknowledgments
This paper is dedicated to the memory of our inspirational teacher Professor M. Barbara Cabalska (19 October 1927 to 5 February 2020), who was the first clinician in Poland to care for pregnant patients with PKU, and the supervisor of the first medical thesis devoted to maternal PKU syndrome, which was defended 25 years previously.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.