
Abstract
Bilateral tubal pregnancy (BTP) is a very rare form of ectopic twin gestation. Many times, they occur after the use of assisted reproductive therapy. Most cases of BTP are diagnosed during laparoscopy. This case report demonstrates a rare preoperative, sonography diagnosis of a spontaneous BTP which occurred after a tubal ligation. The sonogram revealed two corpus luteal cysts, both located on the right ovary, which suggests that the left tubal pregnancy most likely occurred as a result of ovum transmigration. This case demonstrates the important role that sonography plays in the early diagnosis of ectopic pregnancies as well as the importance of thoroughly examining the entire pelvis during a pelvic sonogram.
Keywords
The incidence of ectopic pregnancies in the United States is approximately 2% of all pregnancies.1-3 The fallopian tubes are the most common location for ectopic pregnancy, and while it is extremely rare, they can be the site of more than one pregnancy. Bilateral tubal pregnancy (BTP) is a rare form of ectopic twin gestation and occurs significantly less common than a unilateral tubal pregnancy.1,2 Risk factors for ectopic pregnancy are the use of assisted reproductive technologies (ARTs), ovulation-inducing medications, tubal ligation, and damage to the fallopian tubes.1,2,4,5
This case report presents a sonographic diagnosis of spontaneous BTPs after a tubal ligation. It also demonstrates two corpus luteal cysts on the same ovary, and therefore presumed ovum transmigration of one ovum to the contralateral fallopian tube.
Case Report
A 36-year-old female presented to the emergency department with complaint of pelvic pain associated with an early pregnancy. The patient reported regular menstrual cycles and a history of a bilateral tubal ligation. The first day of the patient’s last menstrual period was 6 weeks prior and pregnancy was confirmed with a positive urine pregnancy test. On this initial presentation, the patient’s serum beta-human chorionic gonadotropin (βhCG) was 1019. The patient denied vaginal bleeding. Transabdominal and endovaginal pelvic sonograms were performed on a Philips IU-22 ultrasound system (Philips Medical, Bothell, WA, USA), using C5-1 MHz and C8-4v MHz transducers. The sonogram did not identify an intrauterine pregnancy or any findings suspicious for ectopic pregnancy. The patient chose to follow an expectant care plan of management. Due to her history of tubal ligation, this patient’s pregnancy was considered high risk for an ectopic implantation. The patient was instructed to come back in 2 days for follow-up care.
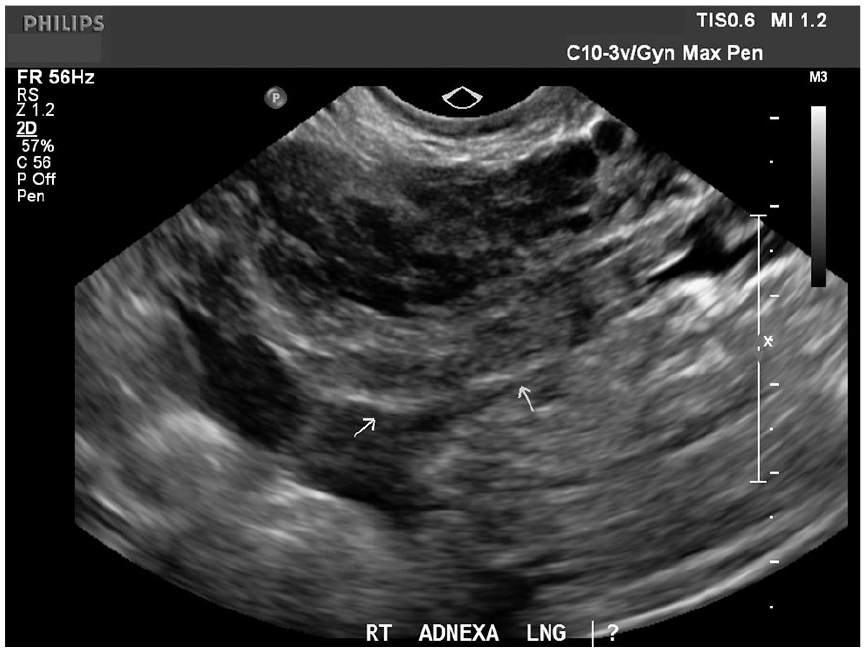
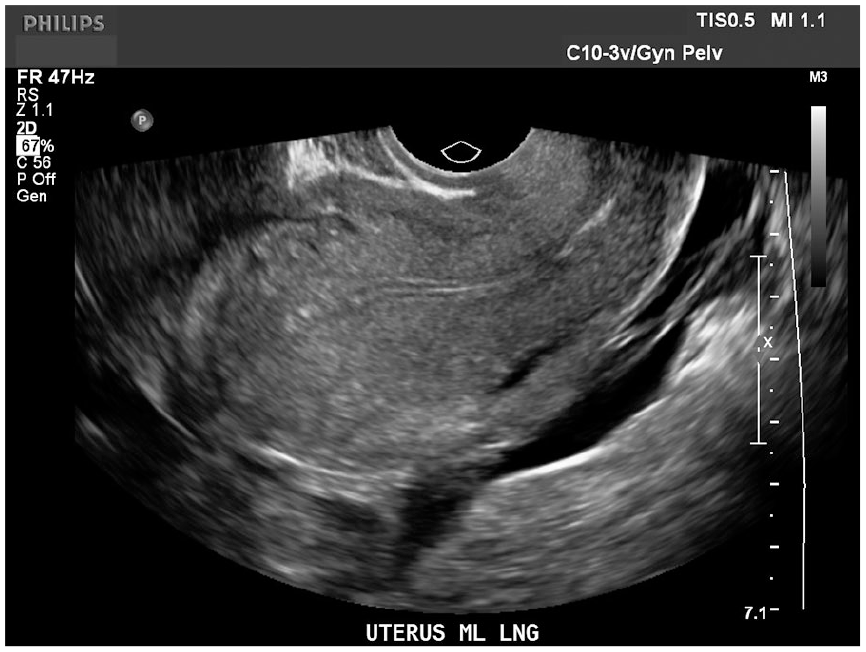
The patient presented 2 days later with persistent pelvic pain and a βhCG of 1077, which is much lower than would be expected. A repeat sonogram was performed to evaluate the pain and location of the pregnancy. Transabdominal and endovaginal pelvic sonograms were performed on a Philips IU-22 ultrasound system (Philips Medical), using C5-1 MHz and C10-3v MHz transducers. The sonogram revealed no evidence for an intrauterine pregnancy (Figure 1), the right ovary contained two corpus luteal cysts (Figure 2), and new bilateral adnexal masses which were separate from the ovaries (Figures 3 and 4). The bilateral adnexal masses were highly suspicious for BTPs. The patient was treated with methotrexate and instructed to follow up with serial βhCG levels.
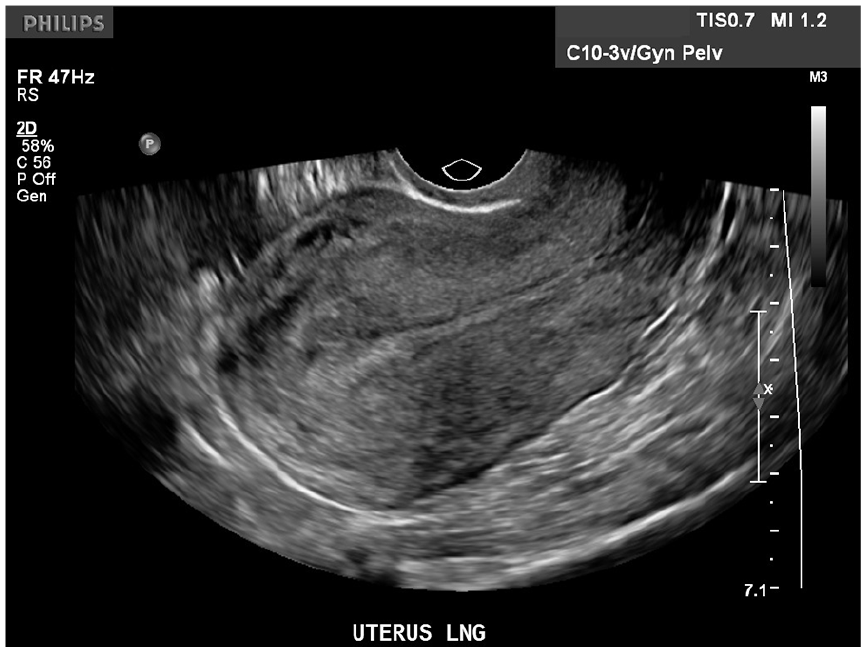
Longitudinal sonogram of the uterus demonstrates a thin endometrial lining with no sign of an intrauterine pregnancy.
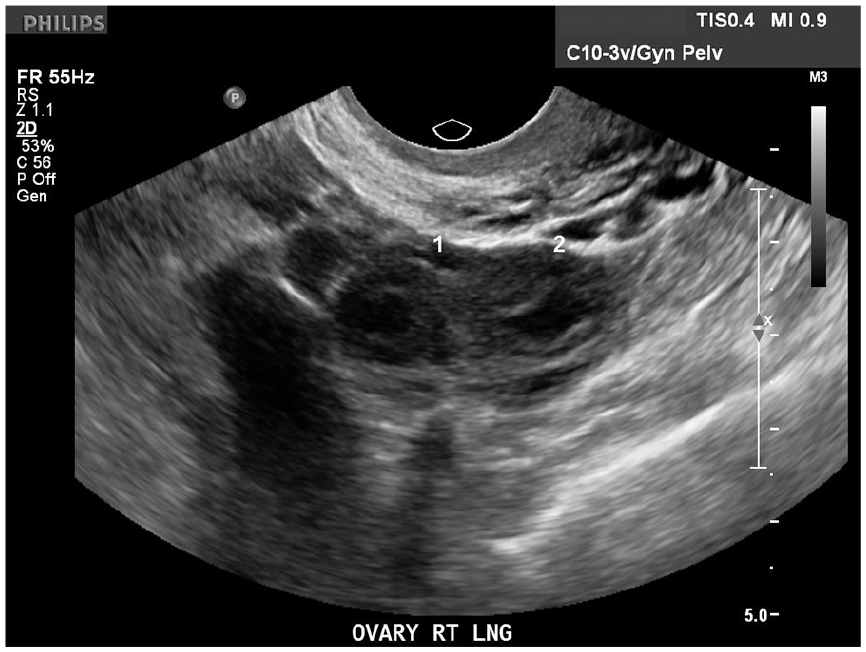
Longitudinal sonogram the right ovary demonstrating two rounded structures with thick rims consistent with a corpus luteal cyst.
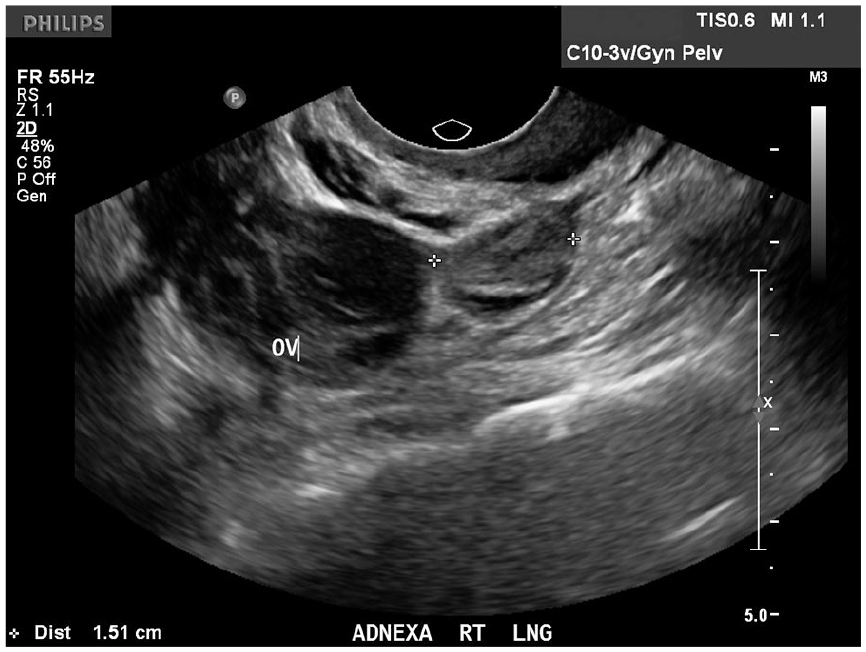
Longitudinal sonogram of the right adnexa demonstrates a round heterogeneous mass inferior to the right ovary. This adnexal mass is consistent with the right ectopic pregnancy.
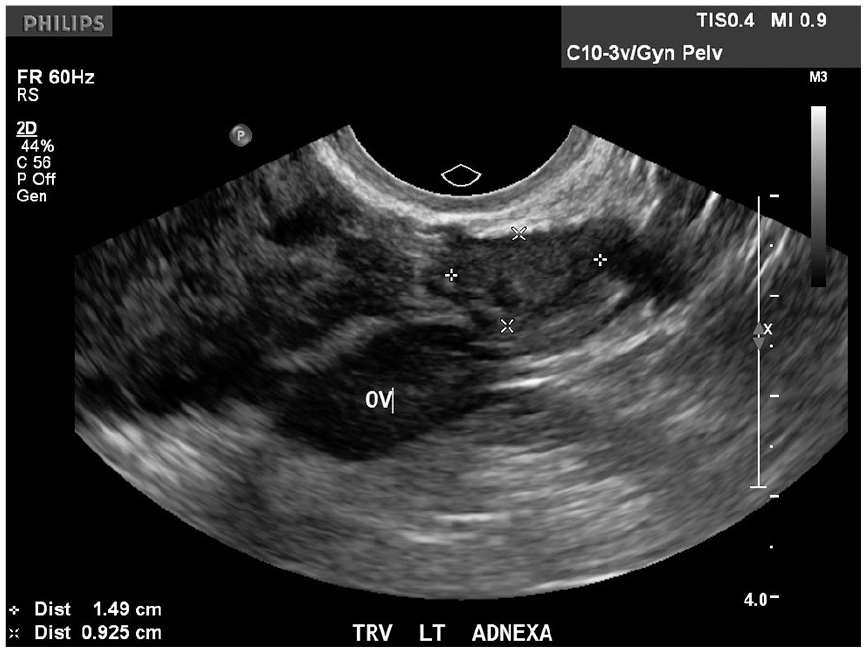
Transverse sonogram of the left adnexa demonstrates a round heterogeneous mass adjacent to the left ovary. This adnexal mass is consistent with the left ectopic pregnancy.
Over the next 2 weeks, the patient had serial βhCG levels that trended downward and then presented to the emergency department with acute onset of pelvic pain. At this time, her βhCG had dropped to 48. A sonogram was performed to evaluate the etiology of pain. A transabdominal and endovaginal pelvic sonogram was performed on a Philips IU-22 ultrasound system (Philips Medical), using C5-1 MHz and C10-3v MHz transducers. This sonogram revealed no evidence of an intrauterine pregnancy; however, an irregular hyperechoic area in the right adnexa was noted (Figure 5) and a new finding of hemoperitoneum (Figure 6). Based on the previous diagnosis, these new sonographic findings were concerning for a ruptured ectopic pregnancy.
Longitudinal sonogram of the right adnexa demonstrates an irregular hyperechoic area, without definite mass.
Longitudinal sonogram of the uterus demonstrates a thin endometrial lining with no sign of intrauterine pregnancy. New findings of hemoperitoneum are demonstrated in the posterior cul-de-sac.
The patient was taken to the operating room for an exploratory laparoscopy. The left fallopian tube was found to be ruptured with active bleeding. The right fallopian tube was still intact. A bilateral salpingectomy was performed along with evacuation of 600 cc of hemoperitoneum.
Pathology results for the bilateral salpingectomy confirmed the preoperative sonographic diagnosis of BTPs. Specifically, a ruptured left fallopian tube with ectopic pregnancy was found and an intact right fallopian tube that contained an ectopic pregnancy.
Discussion
There are several factors, which make this case unusual. First, this pregnancy was a very rare spontaneous BTP, occurring after a tubal ligation. Second, this case demonstrates a sonographic diagnosis of the BTPs. Finally, both corpus luteal cysts were located on the same ovary, suggesting ovum transmigration.
The incidence of ectopic pregnancies in the United States has increased in recent years to approximately 2% of all pregnancies.1-3 This increased rate of tubal pregnancy is likely multifactorial. Some reasons include more accurate methods for early detection of pregnancy, increased use of ARTs, ovulation-inducing medications, increased rates of tubal ligation, and other damage to the fallopian tubes. Damage to the fallopian tubes can be the result of a previous tubal pregnancy, sexually transmitted diseases, endometriosis, or adhesions from previous interventions.1,2,4,5 The biggest risk factor in this case was the patient’s history of a bilateral tubal ligation.
While it is extremely rare, the fallopian tubes can be the site of more than one ectopic pregnancy. This could occur in three different settings such as a unilateral tubal twin pregnancy, bilateral tubal twin pregnancy (BTP), or a tubo-uterine (heterotopic) pregnancy.2,6,7 Risk factors and clinical symptoms associated with BTP are the same as with a unilateral tubal pregnancy. A BTP would also require multiple ovulations.1-3,7-9 When both fallopian tubes are involved, there is greater risk of tubal rupture and hemorrhagic shock, and the patient’s morbidity and mortality is increased. 2
A BTP only occurs 1 in 200 000 pregnancies.1,2,4,7 The first reported case of BTP was by Bledsoe in 1918.2,10 Since then, there have been several reported cases of BTP as well as unilateral tubal pregnancies occurring after tubal ligation. Most of the reported cases of BTP have been after the use of assisted reproductive techniques or ovulation-inducing medication.7,8,11 Spontaneous BTPs make up a very small number of these cases, making them the rarest type of ectopic pregnancy reported.1,2,7,8,12 It is possible that the actual incidence may be higher; however, many cases likely go undiagnosed or unreported.7,8
The diagnosis of an ectopic pregnancy uses a combination of βhCG levels, sonographic findings, and clinical symptoms. The most frequent clinical findings with bilateral ectopic pregnancy are the same as with a unilateral ectopic pregnancy. These clinical findings include vaginal bleeding, abdominal pain, and amenorrhea. 1 As in this case, the βhCG with an ectopic pregnancy will not double as expected with a normal intrauterine pregnancy. 13 While an abnormal rise in βhCG suggests at least one tubal pregnancy, it gives no indication that bilateral disease should be suspected. 2 The diagnosis of multiple ectopic pregnancies can be very difficult and is typically an incidental finding diagnosed intraoperatively.1,7,8,11,14
Historically, sonography has not provided reliable information in patients with bilateral disease. This case demonstrates a preoperative diagnosis of BTPs with sonography. In the setting of a positive pregnancy test and the absence of an intrauterine gestational sac on sonogram, the adnexa should be thoroughly evaluated for the presence of an ectopic pregnancy. Sonographic demonstration of an ectopic pregnancy usually presents in one of the two ways. The most common finding, occurring nearly 60% of the time, is an inhomogeneous mass that moves separate from the ovary, as was seen in this case.15,16 The other less common finding is a mass with a hyperechoic ring around a gestational sac. The gestational sac may contain a yolk sac or a fetal pole with or without a heartbeat. 15
The management of BTP is either medical or surgical depending on the patient’s clinical condition at the time of diagnosis and their desire of future fertility.7,8,11 The use of methotrexate treatment for tubal pregnancy is common since it limits the damage to the fallopian tube that occurs with a surgical procedure. Bilateral tubal pregnancies require an adjustment of the systemic methotrexate dose. Without proper diagnosis by sonogram, the dose would not be appropriately adjusted, and therefore would not be as effective.1,2,14,17
In this case, the sonogram showed both corpus luteal cysts located on the right ovary, but the tubal pregnancies were located in both the right and left fallopian tubes, suggesting ovum transmigration. Many studies have shown that the corpus luteal cyst may be located on the contralateral ovary in up to 50% of ectopic pregnancies.18-20 This is due to the method of ovum migration. There are two theories for ovum migration during pregnancy. The first theory occurs when a sweeping motion of the fimbriated end of the fallopian tube picks up an ovulated oocyte over the ovary and takes it to the ipsilateral fallopian tube. The other theory suggests external or transperitoneal ovum transmigration, during which the oocytes are extruded into the follicular and peritoneal fluid in the cul-de-sac. From here, the ovum may be picked up by either fallopian tube.7,18-20 This can occur with both ectopic and intrauterine pregnancies.17,19,21 Ovum transmigration is considered a possible reason for ectopic pregnancy simply due to a delay in implantation. 19 Thus, when ectopic pregnancy is suspected, if more than one corpus luteal cyst is noted on the same ovary, it is important that the technologist thoroughly evaluate both adnexa for abnormal findings.
Conclusion
This case demonstrates the important role that sonography plays in diagnosing a suspected ectopic pregnancy. With clinical symptoms being the same for both unilateral and bilateral ectopic pregnancies, both adnexa must be thoroughly imaged to rule out bilateral pathology. A BTP is extremely rare; however, sonography can help aid in an early diagnosis and help ensure the patient is offered conservative medical treatment. Unfortunately, in this case, a sonographic diagnosis was made, but the conservative methotrexate treatment failed, resulting in a required surgical intervention.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.