
Abstract
Ovarian pregnancy is rare but may occur with in vitro fertilization-embryo transfer in women who have undergone bilateral salpingectomy. We report a case of an approximately 30-year-old woman who had in vitro fertilization and a history of bilateral salpingectomy, and was diagnosed with an ovarian pregnancy. Laparoscopic enucleation of the gestational product in the ovary and ovarian remnant reconstruction were performed. The patient recovered well after surgery and was discharged home 5 days postoperatively. ß-human chorionic gonadotropin was undetectable 3 weeks after the surgery. Awareness of the possibility of ovarian pregnancy after in vitro fertilization-embryo transfer is the most important step in an early diagnosis and treatment. Salpingectomy should be carefully performed to eliminate the risk of heterotopic pregnancy, especially in cases where a subsequent gestation is desired.
Keywords
Introduction
Ovarian pregnancy (OP) is one of the rarest forms of extrauterine pregnancy, accounting for 1/7000 to 1/40,000 pregnancies. 1 OP after in vitro fertilization-embryo transfer (IVF-ET) with a previous bilateral salpingectomy is even rarer, and only a few cases have been reported.2–5 We report an ovarian pregnancy following bilateral salpingectomy for tubal pregnancy twice in a patient who had IVF. We also performed a literature search for related cases and discuss these cases.
Case report
Case presentation
A woman who was almost 30 years old, G3P0, with a history of a tubal pregnancy twice, presented to the Emergency Department complaining of minor lower abdominal pain, which started 1 day before her presentation. She was pregnant as a result of an IVF cycle. The patient had her first spontaneous pregnancy in her early 20 s, and it was an ectopic pregnancy at the left fallopian tube and was treated with salpingectomy. Four years later, she became pregnant and the pregnancy was an ectopic pregnancy in the right fallopian tube, which was treated with salpingectomy. Three years later, the decision was made to treat her infertility via IVF after the surgery. This treatment was carried out and an IVF cycle was started. Twenty-three mature oocytes were collected and 16 were fertilized. Twenty-nine days before her admission to the Emergency Department, two thawed embryos on day 3 were transferred. Intramuscular progesterone in oil 60 mg daily was prescribed as luteal support. Her serum ß-human chorionic gonadotropin concentration was measured 2 weeks after the transfer, and it showed a positive result. However, a transvaginal ultrasound showed an empty uterine cavity and a right adnexal mass, which strongly suggested an ectopic pregnancy (Figure 1). Her serum ß-human chorionic gonadotropin concentration was 55,523 IU/L.

Ultrasound scan shows a gestational sac in the right ovary.
An injection of methotrexate was initially planned, but not performed to avoid bleeding due to puncture. An emergency laparoscopy was performed after the patient provided consent for treatment. The operation showed thickened inflammatory walls of the stump of the fallopian tubes with adhesions to adjacent tissues, a slightly enlarged uterus, absent fallopian tubes, and a normal sized left ovary. The right ovary was slightly enlarged with a normal appearance (Figure 2). We found that the stump of the right tube was covered with the ovary because the adhesion between the uterus and the right ovary was separated. When a knot on the stump of the right fallopian tube was pulled out, a ruptured gestational sac was observed in the ovary. Because this morphological feature suggested an ectopic right OP, wedge resection of the ovary at the site of abnormality was performed. The ovarian remnants were reconstructed with a 3/0 Vicryl suture. Approximately 600 mL of blood was lost during the operation. A pathological evaluation showed ovarian tissue with areas of hemorrhage and chorionic villi, which confirmed a right ovarian gestation (Figure 3).

Intraoperative image of the pelvic area during laparoscopy. A slightly enlarged right ovary with a normal appearance can be seen with no right fallopian tube. The arrow indicates the location of the gestational sac in the ovary.

Histology shows right ovary tissue. The villi (arrow) are surrounded by ovarian tissue and hemorrhage can be seen.
The patient recovered well after surgery and was discharged home 5 days postoperatively. ß-HCG concentrations were undetectable 3 weeks after the surgery. The patient and her husband were satisfied with the treatment.
The study received the approval of the ethical committee of the Second Hospital of Hebei Medical University (approval number: 2022-P029). Written consent was obtained from the patient for the use of their clinical information and images used in the case report. We have de-identified the details such that the identity of the patient may not be ascertained in any way. The reporting of this study conforms to the CARE guidelines. 6
Literature review
We performed a literature review using a MedLine and PubMed search with the keywords “ovarian pregnancy”, “primary ovarian ectopic pregnancy”, “in vitro fertilization embryo transfer”, “frozen–thawed embryo transfer”, “assisted reproductive technology” “IVF-ET”, “FET”, “ART”, and “bilateral salpingectomy”. We found four cases of OP after IVF–ET with previous bilateral salpingectomy in the literature from 1954 to the present2–5 (Table 1).
Review of cases of ovarian pregnancy following in vitro fertilization-embryo transfer with previous bilateral salpingectomy.
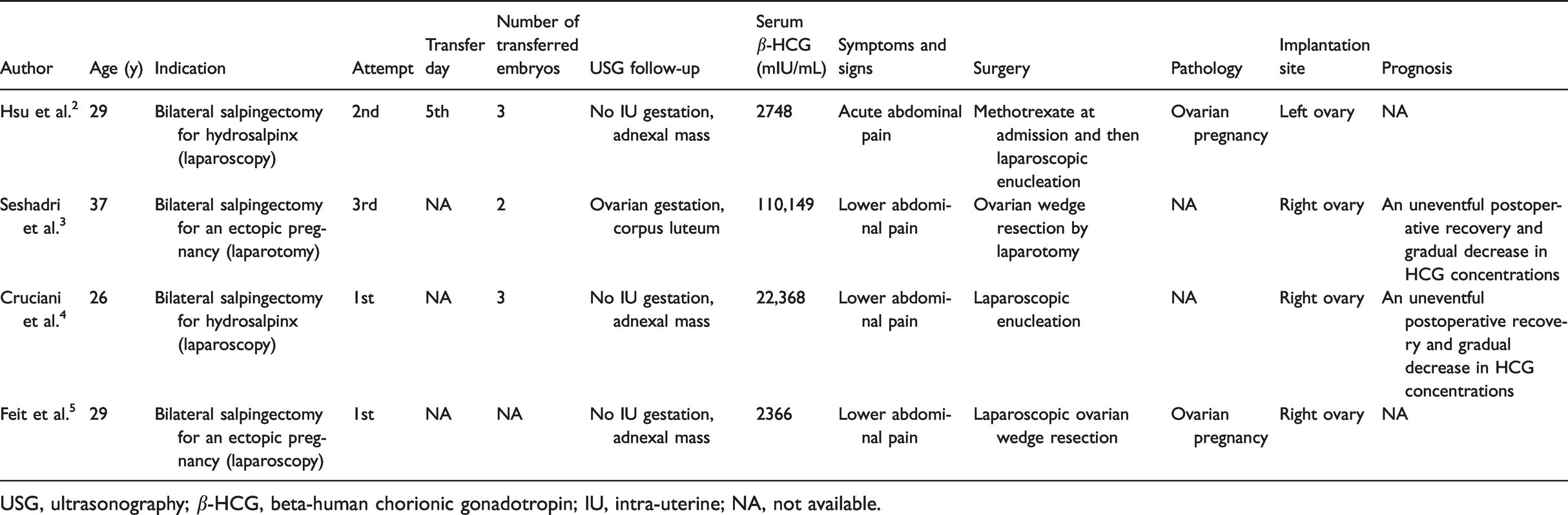
USG, ultrasonography; β-HCG, beta-human chorionic gonadotropin; IU, intra-uterine; NA, not available.
Discussion
In 1968, some researchers 7 suggested that there are two types (intrafolliculary and extrafolliculary) of OP, and less is known about the intrafolliculary type. Dursun et al. 8 stated that, in the primary type of ovarian ectopic pregnancy, the ovum is fertilized in the peritoneal cavity and then it is implanted into the ovary. Secondary ovarian ectopic pregnancy develops as a cause of tubal abortion of the embryo and then it is implanted in the ovary. Four criteria have been proposed to distinguish OP from abnormal pregnancies, and one of them is that the fallopian tube with its fimbria should be intact and separate from the ovary. However, the patient diagnosed with OP in the present study did not have the fallopian tubes. The mechanism of OP after IVF-ET with previous bilateral salpingectomy is unknown.
In 2014, Shan et al. 9 showed that pelvic inflammatory disease, previous surgery in the pelvic area, and intrauterine device use may be associated with OP. These factors are generally thought to be associated with ovarian inflammation, which leads to a reduction in follicular fluid pressure and ovulation disorder. The ovum is then trapped in the ruptured follicles and fertilization only occurs in the ovary. Zhu et al. 10 found that IVF-ET was a risk factor for OP. Possible causes of OP include the reverse migration of embryos through the fallopian tubes, the volume of the injected culture medium, a difficult ET, and even perforation of the uterus during ET. These pathological processes may explain why the implantation site occurs in the ovary, but they cannot explain how the embryo ended up in the ovary in this case.
Hsu et al. 2 and Seshadri et al. 3 suggested that dissecting the fallopian tubes with electrocauterization can cause a reduced blood supply and poor healing at the utero-cornual region, which might result in pressure necrosis and then fistula formation after salpingectomy. This situation is likely to have occurred in our case. Feit et al. 5 considered that, while transferring the embryo via an ET tube, migration of the embryo through a tuboperitoneal fistula may occur. In our case, the right tubal stump was adherent to the right ovary, and a tract could not be seen by the naked eye, but a cornual fistula was the most likely reason for OP.
In addition, during controlled ovarian hyperstimulation, high drug concentrations cause an increase in steroid hormone concentrations, the ovaries are overstimulated, and the ratio of serum estrogen and progestogen changes. This situation increases the sensitivity of constriction of uterine smooth muscle, 11 and strong endometrial waves in the fundal area of the uterus can move embryos into the cornual fistulae. Oocyte retrieval may lead to the formation of ovarian surface scars 3 and a fistulous communication between them, resulting in ectopic implantation from the uterus to the ovary. However, in this case, ET involved a frozen–thawed cycle rather than a fresh cycle, there was no ovarian stimulation, and the scar may have recovered within several months after oocyte retrieval. However, regardless of using frozen ET, the above-mentioned factors cannot be ruled out as a possible etiology for OP. At the same time, the patient had a history of open surgery for ectopic pregnancy twice, and extensive adhesion of the pelvis and abdominal cavity was observed during the operation. Additionally, inflammatory factors cannot be completely excluded.
The clinical manifestations of OP are easily confused with gynecological acute abdomen, and the preoperative diagnostic rate is low. The diagnosis of OP is mainly based on intraoperative exploration and postoperative pathological results. Color Doppler ultrasound plays an important role in the preoperative diagnosis of OP. With the progress of three-dimensional technology, three-dimensional ultrasound can be used in medicine to distinguish OP from an ovarian cyst, which is expected to improve the preoperative diagnostic rate of OP.
With the development of laparoscopic technology, laparoscopic conservative surgery is the main treatment of OP. 12 A common surgical procedure for OP is ovarian cystectomy or ovarian wedge resection, which can achieve ovarian preservation. By enucleating the gestational sac bluntly from the ovary and stopping blood by suture, not by bipolar coagulation, the surrounding ovarian tissue is protected to the greatest possible extent in patients suffering from infertility. This method was also used in our case. In a ruptured ectopic pregnancy accompanied by severe bleeding, a partial oophorectomy can be considered.
Besides salpingectomy for a tubal pregnancy, this procedure is the preferred pretreatment for hydrosalpinx before IVF-ET to improve the chance of pregnancy and a live birth.13,14 Surgeons must pay attention to the details of salpingectomy to avoid a heterotopic pregnancy in patients with IVF. In our case, the stump of the right fallopian tube was a little long with a loose knot on it. The presence of the fallopian tube stump and the formation of a uterine cornual fistula were the main causes of the ectopic pregnancy. Therefore, to eliminate the risk of an ectopic pregnancy, all fallopian tubes should be removed as completely as possible, even for bilateral fallopian tube resection. 15 Aiding uterine cornual suture by silk is recommended. The interstitial part of the fallopian tubes was sutured, and electrocoagulation was performed at the end of the interstitial part of the fallopian tubes in our case. This suggests that this technique can prevent the formation of a postoperative fistula caused by inadequate electrocoagulation, and thus prevent migration of the embryo out of the uterus.
In conclusion, the mechanism of ovarian pregnancy is unclear. The findings in our case suggest that the formation of a uterine horn fistula after bilateral salpingectomy may promote the occurrence of OP. According to the technical standard of an operation, the interstitial part of the fallopian tubes should be removed close to the uterine angle during the operation, and the tubal stump should be closed by ligation at the proximal end of the operation. Additionally, a silk thread should be used for all ligations. In addition, resection of irreparable tubal diseases may not necessarily achieve positive clinical effects. In patients with double tube resection and high-risk factors for OP, especially those with assisted reproductive technology, clinicians and ultrasound technicians should be vigilant, be familiar with and be proficient in the diagnosis and treatment of OP, avoid misdiagnosis and mistreatment, perform an early diagnosis and early treatment, and maximize the protection of the patient’s fertility.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221123683 - Supplemental material for Ovarian pregnancy after bilateral salpingectomy in a patient with in vitro fertilization: a case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605221123683 for Ovarian pregnancy after bilateral salpingectomy in a patient with in vitro fertilization: a case report by Mingle Zhang, Caijun Zhao, Jiahua Zheng, Zhongkang Li, Meiyun Yin, Haiyan Li, Yuan Wang and Xianghua Huang in Journal of International Medical Research
Footnotes
Acknowledgements
We thank the patient and their family in agreeing to share their experience to provide guidance in treating the rare condition of OP.
Author contributions
Mingle Zhang contributed to the conception of the study, performed data analysis, and wrote the manuscript. Caijun Zhao, Jiahua Zheng, and Zhongkang Li contributed to preparing the manuscript. Meiyun yin, Haiyan Li, and Yuan Wang contributed to managing the patient. Xianghua Huang helped perform the analysis with constructive discussions.
Data availability statement
The datasets used during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.