
Abstract
Ganglion cysts are a common, often asymptomatic, finding in the wrist although they may also be found in other joints. This is a case study of a rare presentation of a ganglion cyst in the anterior aspect of the elbow, the antecubital fossa (ACF). Sonography played a primary role in the diagnosis of this unusual injury with magnetic resonance imaging (MRI) confirming the site of origin and surgical intervention resolving the patient’s symptoms.
Keywords
Ganglion cysts in the elbow are rare.1–9 They are a potential cause of posterior interosseous nerve (PIN) compression and/or superficial radial nerve compression which together have an annual incidence rate of less than 0.03%.8,9 These symptoms can be misdiagnosed as lateral epicondylitis causing a delay in relief and treatment. In this case, the correct diagnosis was not made until a sonogram of the antecubital fossa (ACF) was performed showing nonpalpable cystic structures adjacent to the radial nerve. A magnetic resonance imaging (MRI) examination confirmed the diagnosis, and the cyst was excised. The goal of this case report is to emphasize the value of recognizing, searching for, and documenting all potential causes of a patient’s symptoms.
Case Report
A 56-year-old sonographer presented with increasing pain and symptoms of dysesthesia (a disagreeable sensation such as burning, icy-hot, prickly, etc.) 4 with little to no motor symptoms (grip strength, mobility). Six months prior, she had had a hyperextension injury involving her right arm which initially affected her shoulder with extension to her elbow over the following 3 months. At 3 months post hyperextension, she was unable to work without pain in her elbow, numbness in her thumb and forefinger, and went on workplace injury status. A working diagnosis of lateral epicondylitis was made. Symptoms persisted and a sonogram of the right ACF was requested.
The initial sonogram was performed on a Philips iU22 using a linear 15-7 MHz transducer in a primary care hospital. This sonogram showed a series of small hypoechoic lesions adjacent to the radial nerve (see Figure 1). A gadolinium contrast MRI was ordered to determine if these were lymph nodes or neurofibromas and was reported as inconclusive. An electromyography (EMG) study was performed and reported as normal. A second sonogram, in a private specialist clinic, was performed using a Philips Epiq linear 18-5 MHz transducer. The official report stated that there was “a multiloculated ganglion that measured up to 2.2 cm. This results in some superficial displacement of both the superficial and posterior branches of the radial nerve” (see Figure 2).
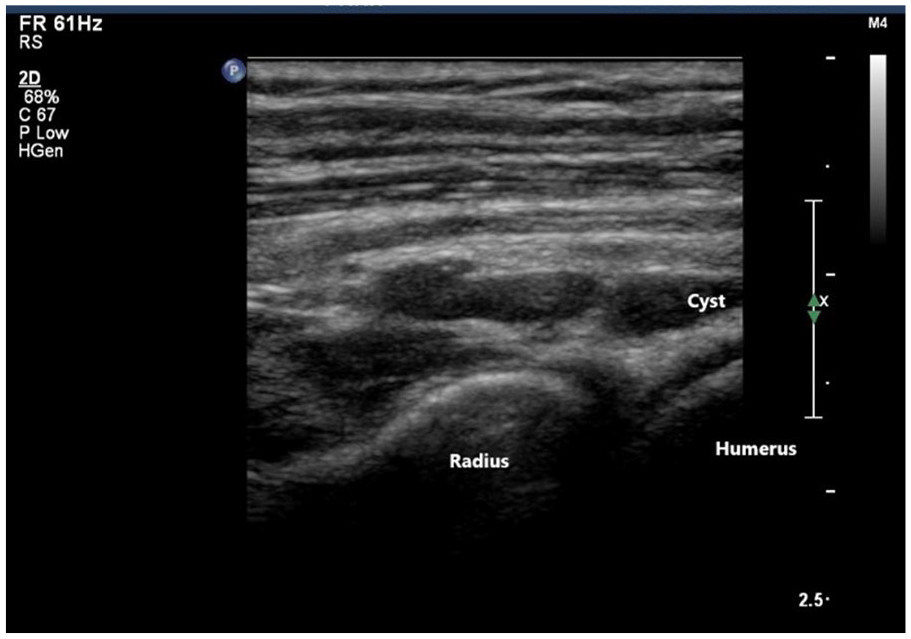
Initial sonographic findings of a set of hypoechoic masses located in the right antecubital fossa, adjacent to the radial head.
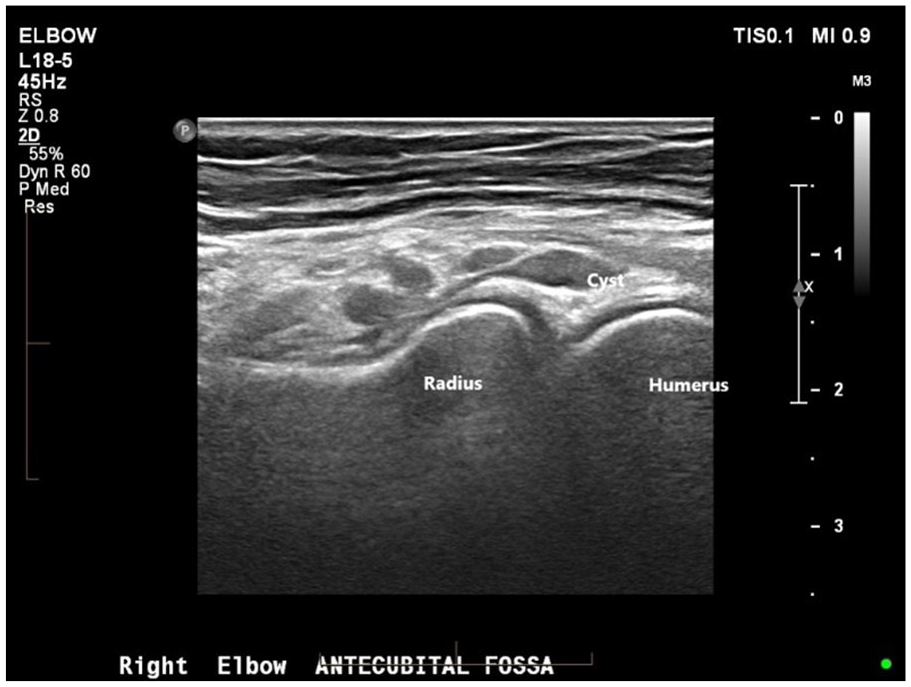
The follow-up sonogram that demonstrated a multiloculated ganglion cyst, adjacent to radial head and joint space.
Ultrasound guided aspiration was attempted. A second gadolinium contrast MRI specifically weighted to identify a ganglion cyst was performed, a ganglion cyst arising from the right radiocapitellar joint was identified (see Figure 3).
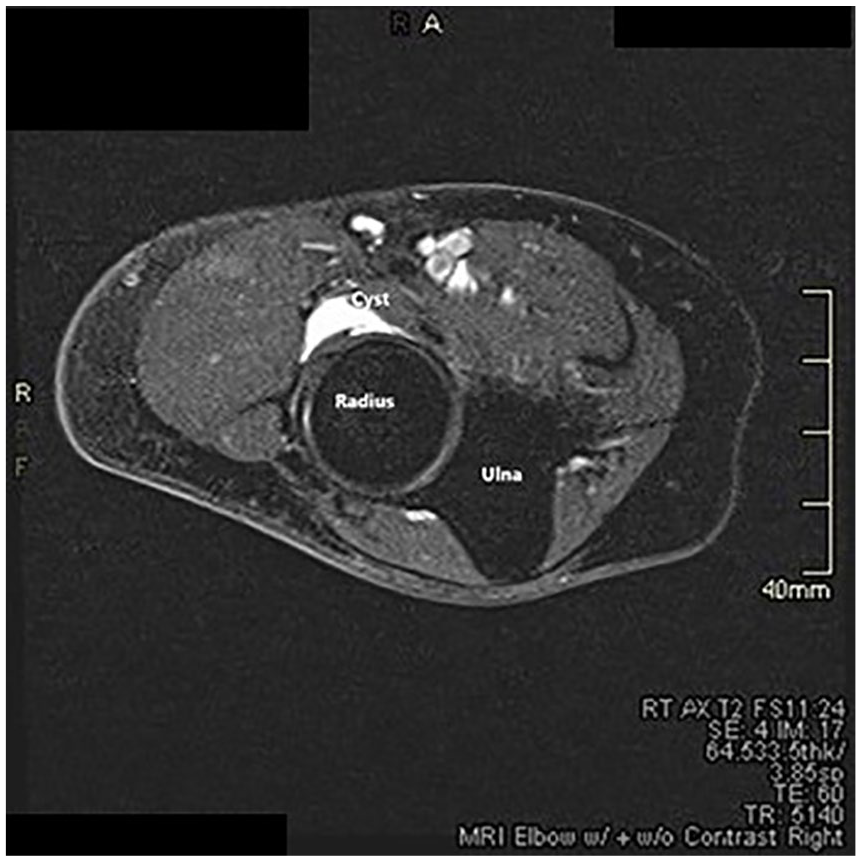
An MRI image that demonstrated a right antecubital fossa ganglion cyst, as a hyperintense mass with T2 weighting, anterior to radius. MRI, magnetic resonance imaging.
Surgical excision of the cyst was performed under general anesthesia. Post surgical physiotherapy for range of motion, strength, and nerve desensitization followed. After 7 weeks, the patient was able to begin a return-to-work program with a full return in 12 weeks (see Figures 4 and 5).

The right antecubital fossa, 4 weeks post surgical removal of the ganglion cyst.
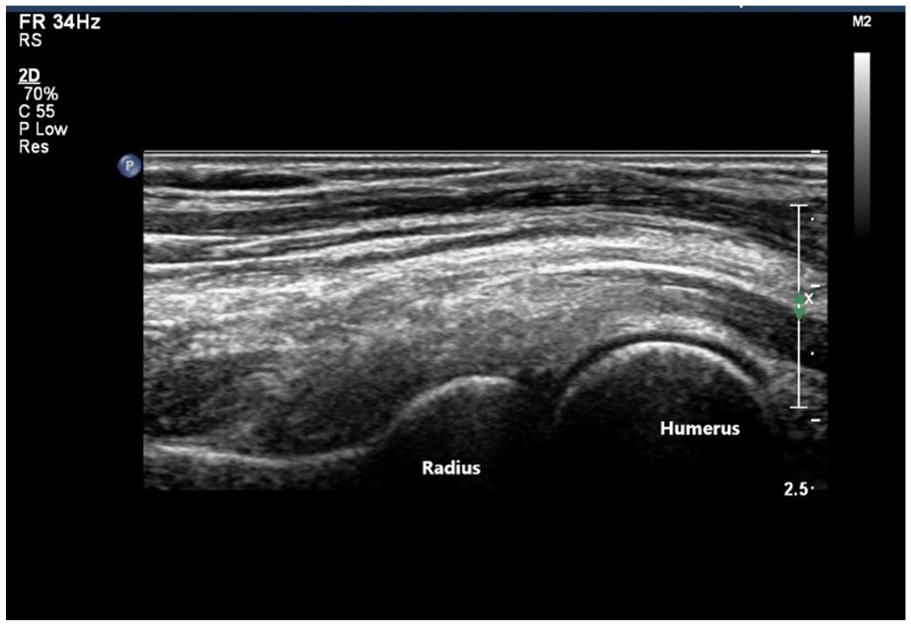
A normal appearing right antecubital fossa, with sonography, 10 months post surgical removal of ganglion cyst.
Discussion
Ganglion cysts are not true cysts as they lack a synovial lining. 2 They are benign sacs filled with a jelly-like material loosely attached to adjacent tendon/tendon sheath or joint capsule.1,3,5 Aspiration of this material is often difficult due to its viscosity. Most ganglion cysts are found in the wrist and hand, up to 88%, and ankle and foot, up to 11% 6 ; they are rarely seen in the elbow.1–9
Ganglion cyst etiology is unclear with most current theories suggesting the mucinous degeneration of connective tissue secondary to chronic damage or continuous micro-injury. 3 Degenerative changes and repeated minor trauma are risk factors. 3
Ganglion cysts are common and largely asymptomatic. They may be assessed as inconsequential or incidental findings by both sonographers and sonologists. Although generally asymptomatic, ganglion cysts can cause pain and discomfort as space-occupying lesions. 1
When present in the elbow, ganglion cysts can compress the radial nerve affecting either the motor branch (PIN), the sensory branch (superficial radial nerve), or both as the cyst is located anterior to the radial head.3,7 Purely sensory symptoms without motor symptoms, as in this case, are uncommon. 4
The PIN compression alone may present as motor weakness in the PIN distribution (fingers and thumb) while compression of the sensory branch alone may present as pain and decreased sensation along the radial side of the dorsum of the hand. 7 The PIN is commonly compressed in the region of the arcade of Frohse proximal to the supinator muscle (see Figure 6). The superficial radial nerve does not pass through the radial tunnel and is therefore less likely to be compressed. 4
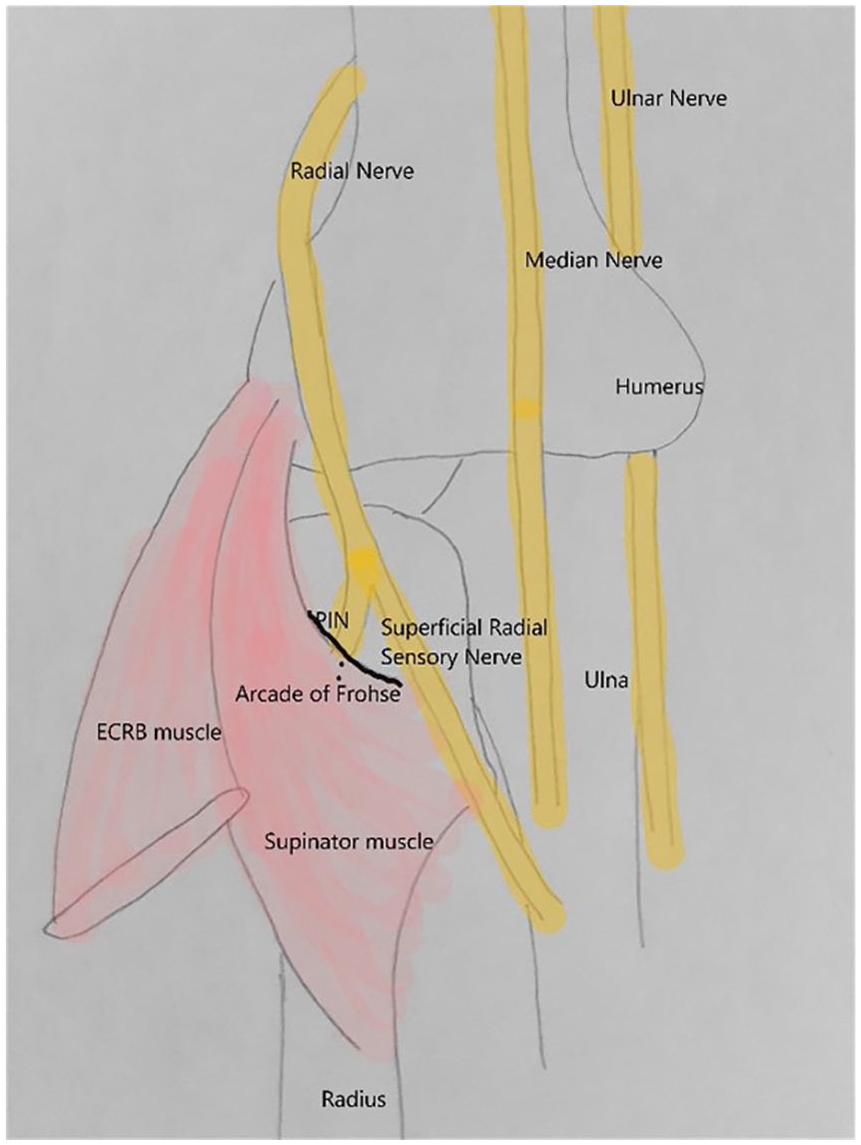
An anatomical diagram of peripheral nerves at the elbow modified from https://musculoskelatalkey.com/radialneuropathy.
Taken together, PIN and superficial radial nerve compression from all causes have an annual occurrence rate of less than 0.03%. 9 Ganglion of the elbow, while rare, should be considered when the presentation involves progressive weakness or sensory changes in an extremity. 7
Most previously reported cases of radial nerve compression by a ganglion cyst have involved the PIN and have presented with a palpable swelling in the ACF unlike the case reported here which had no motor symptoms and no swelling.1,3,4,5,7 Jou et al reported a similar case without swelling or motor symptoms where a ganglion cyst arising from the radio capitellar joint was found at surgery. 7
Diagnosis can be difficult, and many cases are initially treated as cases of lateral epicondylitis.4,7
EMG studies, done to assess nerve or muscle dysfunction, may appear normal if performed less than 3 weeks or greater than 12 weeks post onset of neuropathy. 9
Correct diagnosis is dependent on advanced imaging with sonography and MRI particularly when a palpable mass is not present making the differential diagnosis more difficult. 8 Sonography is often the first imaging modality as it can be less difficult to get an appointment and is widely accepted for the assessment of peripheral nerves. 9
On sonography, ganglion cysts appear as well-lobulated/unilocular, hypo/anechoic masses with no internal flow seen on Doppler investigation. Locating the neck of the cyst as it arises from the joint space aids in the diagnosis of cyst over neurofibroma, abscess, or other hypoechoic lesion. In this case, the neck of the cyst was not seen on a sonogram but was located on the MRI images. On MRI, a ganglion cyst is classically hyperintense on T2 and hypointense on T1 weightings. 1 An MRI has a sensitivity for ganglion cysts of approximately 80%, has a specificity of approximately 50%, 5 and can assess site of origin as well as cyst size.
Surgical excision of a ganglion cyst is the gold standard of treatment with a lower risk of recurrence. 1 Less invasive treatments, including aspiration, steroid injection, and “watch and wait” have a high recurrence rate and other complications. 1
Conclusion
Radial nerve compression by a ganglion cyst is rare. It can present with a variety of symptoms depending on the site of compression and which, if any, branches are involved. Posterior interosseous nerve compression will cause motor symptoms while superficial radial nerve compression will cause sensory symptoms. Normal EMG studies and a possible lack of palpable mass make diagnosis difficult.
Recognition of the possible presentation of a ganglion cyst of the elbow can lead to faster diagnosis shortening the duration of discomfort for the patient.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.