
Abstract
Ectrodactyly, also known as split hand/split foot malformation, is a rare congenital disease defined as the absence or underdevelopment of the central digits with a median cleft of the hand or foot. It can be an isolated sonographic finding or associated with a syndrome. This case study describes isolated left-handed ectrodactyly diagnosed sonographically at 20 weeks gestation, during a routine anatomy sonogram. The patient had no family history of this condition, which demonstrates the importance of sonography for early diagnosis, counseling, and genetic testing options.
Ectrodactyly is most commonly defined as the absence or underdevelopment of the central digits with a median cleft of the hand or foot. The term split hand/split foot malformation (SHFM) is often used interchangeably for the condition. It can be an isolated finding or associated with a syndrome involving extra limb abnormalities. There is great variability in both clinical and genetic presentation.1–4 This report describes a case of fetal ectrodactyly diagnosed with sonography, at 20 weeks gestation.
Case Report
A 26-year-old G4P2012 presented initially to the maternal fetal medicine department for a first trimester sonogram. The patient had no significant medical history. A single intrauterine pregnancy was noted with a 13-week, 0 day gestational age. The sonogram demonstrated a normal nuchal translucency measurement and the first trimester anatomy was unremarkable. Cell-free fetal DNA was collected at this time with negative diagnostic results. The patient presented again for a routine anatomy sonogram at 20 weeks, 1 day gestation. A Philips EPIQ 7 system (Philips Medical, Bothell, Washington) was used with a C5-1 MHz curved array transducer. The sonogram demonstrated left-handed ectrodactyly with a significant cleft in the middle of the hand and normal right hand (see Figure 1). No other overt structural anomalies of the fetus were noted and growth was appropriate for gestational age.

Sonographic image of the normal right hand at 20 weeks, 1 day.
Genetic counseling was initiated and a 3+ generation family pedigree was constructed and reviewed. No history of consanguinity, birth defects, intellectual disability, or limb deformities were reported and the patient’s two other living children had no defects. The paternal grandmother had multiple miscarriages and had a female child pass away shortly after birth. Considering that the amniocentesis revealed both a normal karyotype and microarray, the genetic counselor recommended a gene panel testing specific for ectrodactyly with prevention genetics to further look for a genetic cause of the ectrodactyly. However, the patient was counseled that a negative result for this test would still not fully eliminate the presence of a genetic disorder. The patient decided not to pursue this panel but may consider it postnatally. However, an amniocentesis was performed at 22 weeks, 5 days. Prior to the procedure, the left-handed ectrodactyly was again documented with ultrasound using a Philips iU22 system (Philips Medical) with a C5-1 MHz curved array transducer. The procedure was performed without complications. The results reported no currently known, clinically significant genomic gains or losses using chromosomal microarray (CMA) with the Illumina CytoSNP-850K BeadChip array performed by Colorado Genetics in Denver, Colorado. No excessive regions of homozygosity were detected with the same test. Concurrent cytogenetic studies revealed a 46, XX female karyotype. The specimen was negative for maternal cell contamination. The patient had two additional fetal sonograms at 24 weeks, 5 days (see Figure 2) and 30 weeks, 5 days, using a Philips iU22 system (Philips Medical) with a C5-1 MHz curved array transducer. Both examinations revealed no overt anomalies, apart from the ectrodactyly, and growth was appropriate for gestational age. At delivery, syndactyly of the thumb and forefinger were noted with absent third and fourth digits.

Sonographic image of the left hand and forearm demonstrating ectrodactyly at 24 weeks, 5 days.
Discussion
During weeks 4 to 8 of gestation, fetal limb development occurs. It begins with the limb bud, which consists of highly proliferative mesenchymal cells overlying endoderm internally and covered by ectoderm externally.5,6 The process starts with the paddle stage, when the ectoderm thickens to form the apical ectodermal ridges (AERs) distally. Next, plate-like structures with five radially oriented digital rays form on the limb buds. These will eventually form the hands and feet and the digital rays will become the digits in what is called the plate stage. Finally, during the rotation stage, the upper and lower limbs rotate in opposite directions. 5 The limbs can be divided into three segments: the stylopod (upper arm and leg), zeugopod (forearm and lower leg), and autopod (hand and foot). 3
Three types of specialized cells are responsible for producing signaling molecules that control the growth and development of the developing limb buds by instructing the cells to remain undifferentiated, differentiate, or proliferate. These groups of cells include, the previously described and most critical, AER, the progress zone (PZ) and the zone of polarizing activity (ZPA). Environmental or genetic factors that cause cell death in these regions, most notably the AER, can lead to ectrodactyly.6,7 The second, third, and fourth digits make up the central rays flanked on either side by the preaxial or medial ray and postaxial or lateral ray. The central rays differentiate as directed by the AER at a different time from the preaxial and postaxial rays, therefore leading to a central ray defect or ectrodactyly, if a problem occurs (see Figure 3).1,7
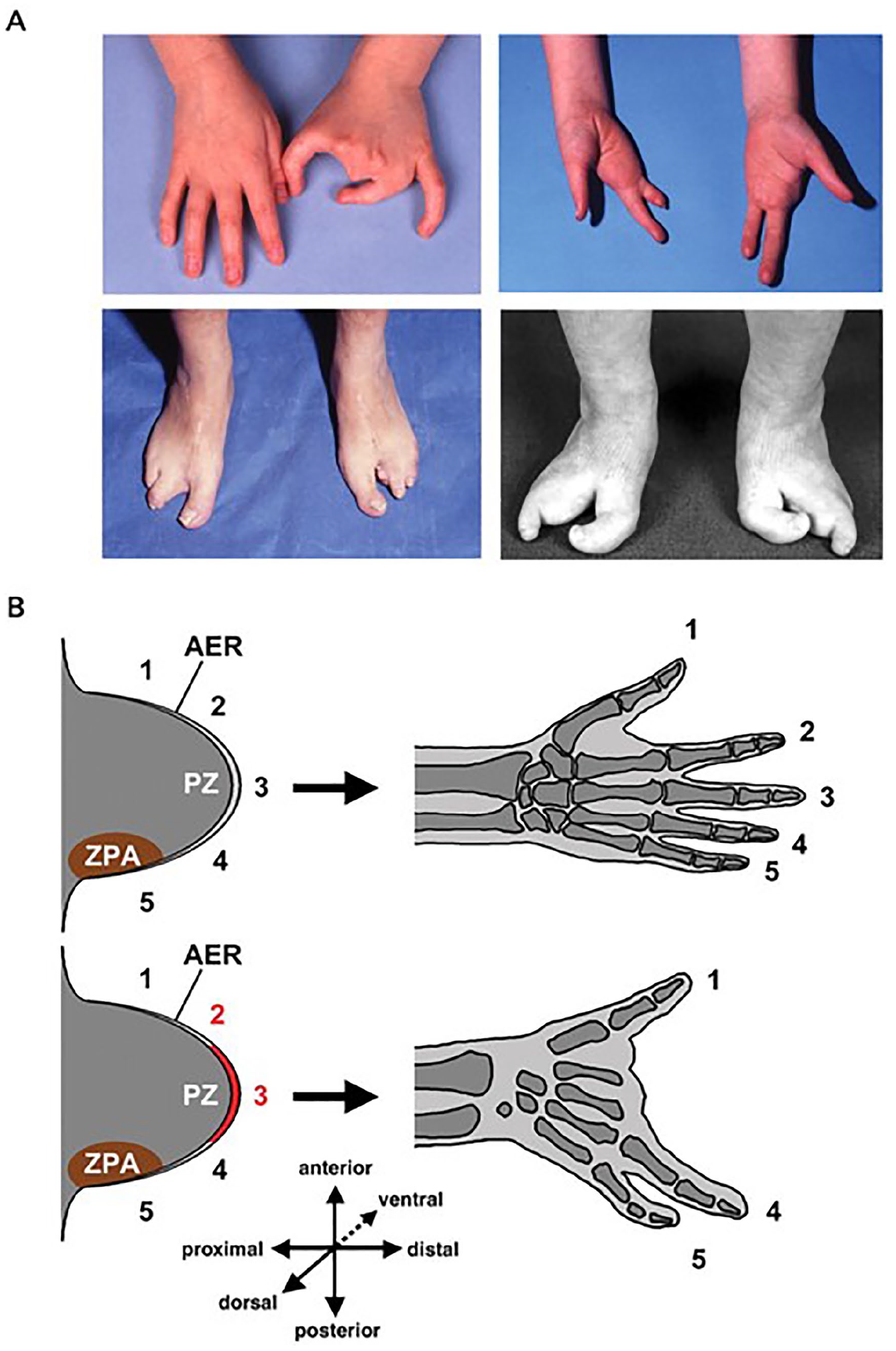
(A) Macroscopic appearance of ectrodactyly demonstrating the phenotypic variability in both hands and feet and (B) diagram of the normal development of the hand (top) and AER defect (bottom). AER, apical ectodermal ridge. Reproduced with permission from Duijf et al 7 (Oxford University Press).
The word ectrodactyly can be broken into two parts, ektroma and daktylos, meaning abortion and finger, respectively, in Greek. The term split hand/foot malformation, or SHFM, can also be used interchangeably. 1 Other terms include cleft hand, oligodactyly, partial terminal aphalangia, and lobster or crab claw malformation. 4 Ectrodactyly is a rare congenital condition characterized by a wide spectrum of phenotype, ranging from a slightly short or malformed central digit to the presence of only a single digit (monodactyly). It can affect one to all autopods. However, the most common presentation is the absence or underdevelopment of the central digits with a median cleft of the autopod and possible fusion of the lateral digits (syndactyly).1–3 There can also be variability in the clinical presentation within first and multiple generation family members affected or between limbs of a single person. 4
The condition has been further classified as either typical or atypical. Typical ectrodactyly is defined as a V-shaped lesion, involving only the phalanges with an incidence of one per 90,000, whereas the atypical condition involves the phalanges and also the metacarpals creating a U-shaped lesion and is less common at one per 150,000 incidences.4,8
Ectrodactyly can occur as an isolated sporadic malformation (nonsyndromic) or be part of a syndrome with other extra limb abnormalities. The most common form of inheritance is autosomal dominant with incomplete penetrance, but recessive or x-linked cases have been reported as well.1–4,6,9 These can also occur as sporadic de novo mutations.3,6,9 Nonsyndromic ectrodactyly can involve one or more limbs. Split hand/foot malformation with long bone deficiency, frequently involving the tibia and fibula, has also been described.2,6,9 Incidence for isolated ectrodactyly has been estimated to be one per 18,000 births with 80% of these cases having only one limb affected.1,6 Recent literature has shown that at least 12 different types of nonsyndromic SHFM have been mapped to chromosomes. 9
Syndromic ectrodactyly may also occur with extra limb abnormalities. The most common is the EEC syndrome (ectrodactyly, ectodermal dysplasia, and cleft lip/palate). This syndrome presents with abnormal teeth, nails, lacrimal ducts, nipples, skin, hair, urinary tract, and hearing impairment. Other less common syndromes include limb-mammary, ADULT (acro-dermato-ungual-lacrimal-tooth), Rapp-Hodgkin (RHS), AEC (ankyloblepharon-ectodermal defects-cleft lip/palate), EEM (ectrodactyly ectodermal dysplasia-macular degeneration), ACFS (acro-cardio-facial), Karsch-Neugebauer, Cornelia de Lange, focal dermal hypoplasia, LADD syndrome (lacrimo-auriculo-dento-digital), CHARGE syndrome, and VATER association.3,6 Overall, both syndromic and nonsyndromic ectrodactyly are extremely complex conditions both clinically and molecularly, with great variability in presentation and inheritance, and are genetically heterogeneous.3,4
The hands can be visualized by sonography as soon as the long bones begin to ossify at 11 to 12 weeks gestation. Therefore, the hands can potentially be visualized late in the first trimester, which is also an ideal time as fetal movements are frequent, and the hands are often open. The latter also applies to the middle of the second trimester when the anatomy sonogram is often performed. 10 The following needs to be observed for the hands to be considered sonographically normal: five separate digits of different lengths with three hyperechoic phalanges each (two in the thumb), five hyperechoic metacarpals, hypoechoic carpus, and flexion and extension of the hands to rule out contractures or fixed positions. In addition, visualization of normal long bones (radius, ulna, and humerus) is also important. 10
Historically, ectrodactyly has been detected by sonography in the second trimester, but there are reports of diagnosis as early as 11, 12, and 13 weeks’ gestation using transabdominal and endovaginal sonography. The use of three-dimensional (3D) sonography has also been shown to aid in early characterization and diagnosis of this condition.1,4,11 In addition, 3D sonography may help clinicians counsel appropriately and provide guidance for surgical treatment options and other decision-making processes.4,5
If syndromic ectrodactyly is suspected sonographically, other systemic abnormalities are likely to be involved and a thorough anatomy sonogram should be completed. For example, the lip and palate should be carefully evaluated as ECC syndrome (ectrodactyly, ectodermal dysplasia, and cleft lip/palate) is the most common syndrome associated with ectrodactyly. Cardiac defects have also been reported in association with ectrodactyly. Therefore, the heart should be thoroughly assessed and a fetal echocardiogram may be warranted. 4 Other conditions, such as hearing impairment, have been linked with ectrodactyly syndromes, necessitating hearing screening considerations postnatally. 3
Differential diagnoses for ectrodactyly include brachydactyly (short fingers), oligodactyly (absence of one or more fingers), clinodactyly (often an abnormal fifth digit angling toward the fourth digit), hypoplastic or absent distal phalanges, symphalangism (fused phalanges), syndactyly (fused digits), deformed thumbs and big toes, and amniotic band syndrome leading to amputation of digits.4,10 The reported incidence of amniotic band syndrome varies within the literature from one of 56 fetuses to one of 15,000 live births, to one of 1200 live births. 10 The most widely accepted etiology of amniotic band describes rupture of the amnion in early pregnancy leading to constrictive amniotic bands which lead to compromised circulation and growth of affected body parts, including the digits of the hands and feet.10,12
Surgical management and repair after birth is the only current treatment for ectrodactyly. As each patient’s deformity is different, each surgical repair will also be unique to the patient. Even without surgery, most patients maintain a high level of function with the affected hand. However, surgery can still be considered to further enhance function, as well as the cosmetic appearance. If ectrodactyly is an isolated finding, the patient can often live a very normal life. 8
Conclusion
Ectrodactyly is a complicated condition with significant clinical and phenotypic heterogeneity, making it difficult to make a definitive diagnosis prenatally. However, sonography is an important tool for identifying deformities of the hands and feet. This case highlights the importance of sonography to detect ectrodactyly and how an early diagnosis can aid in early testing and treatment planning.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.