
Abstract
Standard 2D sonography has variable success in the prenatal diagnosis of cleft lip combined with cleft palate. A case is presented that demonstrates the added value of 3D sonography plus color Doppler imaging in confirming this diagnosis. Additional techniques such as the flipped-face view, the reverse-face view, and the oblique-face view are discussed as further enhancements to the prenatal sonographic study of the fetal palate.
The incidence of cleft lip and palate varies over a range of 1 in 700 to 1 in 1000 worldwide. In 1999, the sensitivity of a 2D sonographic scan for detecting facial clefts was reported to be around 25% for cleft lip, 22% for cleft lip and palate, and 1.4% for isolated cleft palate in the routine obstetric screening population, depending on the experience and training of the examiner. 1 Although facial clefting of the fetus can be prenatally diagnosed by 2D sonography and new insights have been provided into prenatal study of the fetal palate by the introduction of 3D sonographic techniques such as the flipped-face view, the reverse-face view, and the oblique-face view,2–5 only a few publications in the medical literature have reported on the role played by Doppler in prenatal sonography diagnosis.6–8
Case Description
The fetal face was scanned with the fetal head mildly flexed, thus avoiding the presence of the umbilical cord, placenta, and bony parts, while awaiting fetal deglutition in order to have a highly anechogenic film of amniotic fluid inside the oropharynx. The sonography equipment used was the Voluson E8 (General Electric Healthcare System, Milwaukee, Wisconsin) with the RAB 4- to 8-MHz transabdominal probe. Standardized second-trimester 2D scan settings were used (second harmonic on high level; cross beam 1; speckle reduction imaging 3; dynamic range 6 and dynamic contrast 7; line density normal and gray map 7; Th = 30, quality, high 1; B53°/V50°). After 2D scanning was completed, a static 3D image was acquired with the region of interest (ROI) set to comprise the area extending from the crown to the fetal neck. A 70/30 mixture of gradient light was used. The scan was performed as part of a routine second-trimester sonographic examination at 21 weeks’ gestation on a woman in her early 30s with no history of consanguinity or congenital anomalies. In the left panel shown in Figure 1a, the sagittal section of the fetal profile obtained in B-mode revealed the fetal tongue in the correct position, a moderately opened mouth with amniotic fluid inside, and a defect in the anatomical right upper lip (white arrow). Color Doppler was then applied, which clearly demonstrated an abnormal bidirectional flow; a trajectory of flow was observed from the oral cavity into the right nasal fossa (Figure 1b, dotted red arrow), followed by exit at the cleft (Figure 1b, dotted white arrow). Three-dimensional volume rendering in the minimum and maximum surface mode was applied, which not only confirmed the 2D sonography diagnosis of cleft lip but also led to the diagnosis of a previously undetected cleft palate (Figure 1c). Antenatal T2-weighted, single-shot fast-spin echo (SSFSE), targeted sonographic magnetic resonance (MR) imaging was then performed as a complementary examination using Tesla 1.5 equipment (Intera Achieva, Philips, Eindhoven, The Netherlands) with a SENSE body coil. T2-weighted images were acquired in the three orthogonal planes using SSSE (single-shot turbo-spin echo sequence, with repetition time of 15,000 ms; echo time of 120 ms; echo train length of 140; acquisitions: 2; matrix: 139 × 256). Each pulse sequence lasted 30 seconds. T2-weighted MR imaging confirmed the presence of a right cleft lip and cleft palate in the sagittal section (Figure 2a–c).
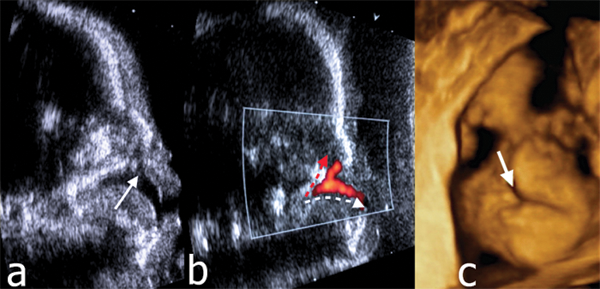
Sagittal section of the fetal profile obtained by 2D sonography showing the fetal tongue, a mildly opened mouth with amniotic fluid within, and a defect at the level of the right upper lip (a, white arrow); color Doppler image with a clear demonstration of an abnormal bidirectional flow showing a trajectory going from the oral cavity into the right nasal fossae (b, dotted red arrow) followed by an exit at the level of the cleft (b, dotted white arrow); and 3D volume rendering with minimal surface modality, which confirmed the 2D sonographic diagnosis (c).
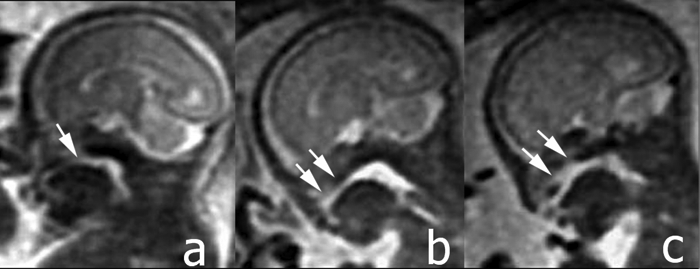
Antenatal single-shot fast-spin echo T2-weighted magnetic resonance imaging in the sagittal section showing the cleft lip (a, white arrow) and the defect in the hard palate (b and c, white arrows).
Discussion
To the best of our knowledge, this is the first case to report on the use of color Doppler sonography in aiding prenatal diagnosis of cleft lip plus cleft palate, followed by confirmation with antenatal MR imaging. In a systematic electronic search (PubMed/Embase) of the medical literature made by Maarse et al 9 on the diagnostic accuracy of 2D sonography in low-risk pregnant women, prenatal detection rates ranged from 9% to 100% for cleft lip with or without cleft palate, 0% to 22% for cleft palate only, and 0% to 73% for all types of cleft defects. When 3D sonography was performed in high-risk pregnant women, the result was a detection rate of 100% for cleft lip, 86% to 90% for cleft lip with cleft palate, and 0% to 89% for cleft palate only. These results have recently been confirmed by Bäumler et al 10 in an investigation of the accuracy of prenatal axial 3D sonography in predicting cleft palate in the presence of cleft lip. Of 79 cases with a prenatal 2D sonographic screening diagnosis of unilateral or bilateral cleft lip at 22 to 25 weeks’ gestation, the sensitivity for detection of cleft lip and palate within this high-risk population was 100%, and specificity was 90%. They concluded that axial 3D sonography of the fetal palate is highly accurate in identifying prenatal cleft palate when cleft lip is diagnosed at mid-trimester 2D sonographic screening.
Campbell and Lees 2 were the first to report the clinical value of a new sonographic 3D technique called the “reverse-face” (3D-RF) view. Campbell et al 3 applied the 3D-RF view in 8 cases of suspected orofacial clefting in which the fetal lips and alveolar ridge were first examined in the frontal plane, and the face was then rotated 180 degrees on the vertical axis to examine the secondary palate by the 3D-RF view. In all but one case (a left-sided cleft in the lips and alveolar ridge, as well as an intact hard palate, where the correct diagnosis was made but a cleft in the soft palate was missed), the 3D-RF technique provided a relatively straightforward assessment of the fetal palate with a high degree of accuracy. Platt et al 4 described the “flipped-face” view, where static volume data sets are acquired and then rotated 90 degrees so that the cut planes are directed along a plane extending from chin to nose. The volume-cut planes are then scrolled from chin to nose to examine in sequence the lower lip, mandible, and alveolar ridge; the tongue; the upper lip, maxilla, and alveolar ridge; and the hard and soft palates. Using this approach, they were able to determine the full length and width of the structures of the mouth and palates, thus allowing examiners to identify both normal anatomy and clefts of the hard and soft palates.
In their examination of 60 fetuses (10 with cleft lip and palate) with gestational age ranging from 20 to 33 weeks, Martinez Ten et al 5 compared the effectiveness of the reverse-face, flipped-face, and oblique-face sonographic techniques in visualizing the hard and soft palate for diagnosis of cleft lip and palate. In their series, involvement of the hard palate was diagnosed correctly in 71% of the cases using the 3D-RF view, 86% of the cases using the flipped-face view, and 100% of the cases using the oblique-face view. Involvement of the soft palate was diagnosed correctly using the flipped-face and oblique-face views in only one of seven fetuses with defects of the secondary palate. Recently, Sommerlad et al 11 assessed the clinical impact of adding the 3D-RF view to conventional 2D sonography in prenatal evaluation of the involvement of the lips, alveolar ridge, and secondary palate in 100 fetuses with suspected isolated orofacial clefting. The sensitivity of 2D sonography with 3D-RF enhancement in the diagnosis of cleft of the lip was 95%, with a false-positive rate (FPR) of 7.7%; for alveolar ridge, the sensitivity was 84.5%, with FPR of 7.2%; and for hard palate, sensitivity was 89.7%, with FPR of 15.6%. Moreover, the 3D-RF view proved to be workable in almost 90% of cases. Benacerraf et al 12 have reported prenatal diagnosis of cleft of the soft palate using the 3D thick-slice en face technique, with further confirmation by antenatal MR imaging, in a fetus affected by Fryns syndrome (cleft palate, diaphragmatic hernia, enlarged echogenic kidneys, and severe polyhydramnios).
Summarizing the medical literature, and based also on our observations, the following clinical considerations can be made: (a) diagnosis of isolated cleft lip is possible with 2D sonography, although enhancement with the 3D-RF view may improve the diagnosis of possible associated cleft palate; (b) directional color Doppler imaging is effective in the prenatal detection of cleft lip and cleft palate by demonstrating an abnormal bidirectional flow trajectory; (c) antenatal targeted MR imaging is a useful complementary examination that contributes to enhancing in utero diagnosis of facial clefting; and (d) when sagittal MR imaging is used, the secondary palate is seen as a smooth midline arch displaying soft tissue signal intensity that is contiguous with the primary palate, whereas coronal images are particularly diagnostic of disorders in the nose and lips.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.