
Abstract
Wormian bones are accessory bones that occur within the cranial suture and fontanelles, most commonly within the posterior sutures. The incidental 3D sonographic detection of isolated wormian bone during a second trimester sonographic examination is reported, together with the counseling and clinical management strategies that followed. We have demonstrated that supernumerary bone can be seen as an isolated sonographic finding in a healthy fetus or can be associated with multiple congenital anomalies. The sonographic detection of a fetus with wormian bone indicates the need for a very thorough examination and genetic counseling for the parents regarding prognosis and risk of recurrence.
Introduction
Wormian bones are accessory bones that occur within the cranial suture and fontanelles, most commonly within the posterior sutures. They occur more frequently in disorders that have reduced cranial ossification, hypotonia, or decreased movement, thereby resulting in deformational brachycephaly. The pathogenesis of wormian bones may be due to environmental variations in dural strain within open sutures and fontanelles. 1
Case Report
A 35-year-old gravida 2, para 1 presented for routine second trimester sonography at 20 weeks 2 days gestation. The patient had undergone a first trimester combined screening test with negative results. (The calculated risk for trisomy 21 was 1:5085 and for trisomy 18/13, 1:10404). The sonographic examination was carried out by using a Voluson E8 (General Electric, Milwaukee, Wisconsin) with a transabdominal 2D and volumetric RAB 4-8D MHz probe.
The biparietal diameter (BPD) was 46.9 mm (25th percentile for gestational age), the fronto-occipital diameter (FOD) was 61.7 mm (75th percentile for gestational age), and the cranial circumference (CC) was 175 mm (25th percentile for gestational age). The cephalic index (CI) was 76. The BPD/FL (femur length) was 1.457 (25th percentile for gestational age), and the BPD/FOD was 0.760 (25th percentile for gestational age). By conventional 2D scan, the skull showed normal morphology with opened cranial sutures and normal fontanelles (Figure 1). The posterior cranial fossa was normal with a transverse cerebellar diameter measuring 21.2 mm (50th percentile for gestational age). The lateral ventricle was 6.4 mm. Humerus length was 31 mm (25th percentile for gestational age), and the femur length was 32.2 mm (50th percentile for gestational age).

Transabdominal conventional 2D sonography performed at 20 weeks 2 days. The cephalic pole is visualized in the sagittal plane without evidence of wormian bone.
Three-dimensional sonography with volume rendering of the fetal head using skeleton mode was performed and showed evidence of a supernumerary bone at the level of the anterior fontanelle in the coronal plane. This bone appeared isoechoic compared to the surrounding bony structures and was diagnosed as a wormian bone (Figures 2A and 2B). A case of morphologically normal metopic suture captured at 19 weeks 3 days in a normal fetus is rendered for comparison in Figure 3.
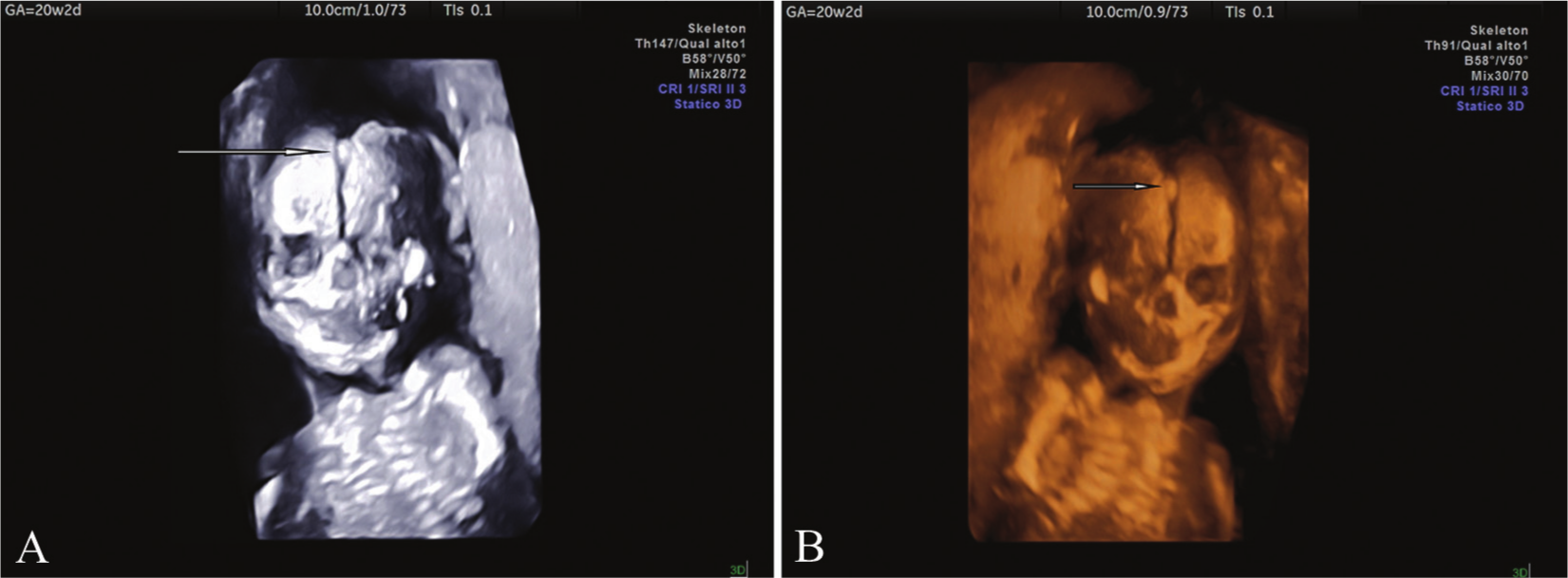
(A) 3D gray-scale sonography performed using skeleton mode in the coronal plane demonstrating a median wormian bone at the level of the normally developed metopic suture (white arrow). Note that the wormian bone appears isoechoic compared to the other surrounding bony structures. (B) Same as Figure 2A with color rendering using a Mix 30/70 gradient light setting.

Transabdominal 3D sonography performed at 19 weeks 3 days using skeleton mode showing a morphologically normal metopic suture in the coronal plane.
The sonographic settings used for the gray-scale 3D rendering were quality, high; B58°/V50° (B = B-mode acquisition angle; V = volume acquisition angle); Mix: 28/72. This acquisition angle was used to avoid motion artifacts from the skull base. A Mix 30/70 gradient light was used for the 3D color rendering. Two volume data sets were acquired with the volume of interest (VOI) set to compose the entire fetal head for subsequent offline “navigation” and analysis.
No other associated sonographic findings were detected. The couple received genetic counseling regarding prognosis and potential outcomes in cases such as this of prenatally detected isolated wormian bone during a second trimester scan, as well as risk of recurrence.
Discussion
Metabolic disorders of the mesoderm might be the underlying etiology in wormian bone formation, 2 and Torgersen has proposed that wormian bones are inherited as a dominant trait. 3 Wormian bones are observed in the coronal suture in 25% of cases, while the rest may occur in any remaining suture and/or fontanelles. 4
Sanchez-Lara et al 1 evaluated the cephalic index in 20 purposefully deformed pre-Columbian skulls and found no significant correlation between the CI and the number of wormian bones in skulls with varying degrees of brachycephalic cranial deformation. When the CI was grouped into the three categories of normal (CI < 81), brachycephalic (CI 81–93), and severely brachycephalic (CI > 93), there was a trend toward an increasing number of wormian bones as the skull became more brachycephalic.
Among 207 cases of craniosynostosis studied by 3D computerized tomography (CT) scans, there was a 3.5 greater odds of developing a wormian bone with premature suture closure. 1 Midline synostosis, specifically metopic or sagittal synostosis, was noted to have more wormian bones in the midline, whereas unilateral lambdoidal or coronal synostosis more often had wormian bones on the contralateral side. Taken together, these data suggest that wormian bones may arise as a consequence of mechanical factors that spread sutures apart and affect dural strain within sutures and fontanelles. 1
The incidence of fontanelle closure by a wormian bone in isolated, nonsyndromic sagittal craniosynostosis is approximately 4%. 5 A wormian bone can occupy the anterior fontanelle in children with isolated sagittal craniosynostosis, giving the appearance of a “closed fontanelle.” Woods and Johnson 6 described a series of 11 patients with fontanellar bones replacing the anterior fontanelle on CT scan. Five children had associated craniosynostosis, 1 had acrocallosal syndrome, and 5 had no other craniofacial abnormalities. They concluded that replacement of the anterior fontanelle with a fontanellar bone is an uncommon finding, often associated with craniosynostosis, and that isolated anterior fontanellar bones can be managed conservatively without an adverse effect on the child.
EL-Najjar and Dawson evaluated 120 adult and 80 human fetal skulls and concluded that wormian bones occur in deformed and undeformed skulls with no significant differences. 7 Researchers have debated whether the presence and frequency of wormian bones (sutural bones, supernumerary bones, and ossicles) are attributable to genetic factors, environmental factors, or both. 8 In a sample of 127 deformed and undeformed crania from New World archaeological sites, O’Loughlin demonstrated that all cranially deformed groups exhibited significantly greater frequencies of lambdoid ossicles, and the apical, parietomastoid, and occipitomastoid wormian bones also appeared with greater frequency in some groups of culturally deformed crania. 9
Jeanty et al were the first to report the prenatal diagnosis of wormian bones in four fetuses. 10 They also noted that wormian bones may be seen in association with congenital anomalies such as chondrodysplasia punctata and cleidocranial dysplasia, dysgenesis of the corpus callosum, micro/macrocephaly, mandibular dysplasia, Menkes syndrome, congenital heart disease, otopalatodigital syndrome, osteogenesis imperfecta, Prader-Willi syndrome, Schinzel-Giedion syndrome Zellweger syndrome, and trisomy 21. More recently, wormian bone has been sonographically detected during a second trimester scan in a fetus presenting with craniosynostosis, wide metopic suture, femoral hypoplasia, and focal distal fibula deficiency. 11
In the case presented, acquisition of volume data sets by 3D ultrasound allowed subsequent offline analysis and navigation within the volume. An acquired volume such as this can then be sectioned on demand along the three orthogonal planes (sagittal, coronal, and axial plane) and resliced with simultaneous anatomical rendering to improve diagnostic accuracy. An additional advantage to using 3D volume sets is that these volumes can be acquired remotely and be interpreted later using offline analysis by readers at tertiary referral centers using DICOM (Digital Imaging and Communications in Medicine) image transfer.
Conclusion
Wormian bone may be incidentally detected during a routine second trimester sonographic examination, especially when using the capabilities of modern real-time ultrasound equipment. If wormian bone is detected, a very thorough sonographic examination is mandatory to search for potential associated congenital anomalies. The sonographic examination should exclude possible underlying or overlapping skeletal dysplasias, and the morphologic features of cranial sutures and fontanelles should be carefully evaluated. Three-dimensional ultrasound, especially in skeleton mode, may aid the prenatal diagnosis by enhancing image quality and rendering of the anatomical details.
In a case in which wormian bone is an isolated sonographic finding and the mother had had a negative first trimester screening test (as in the case presented), counseling and reassurance can be given regarding a likely normal perinatal outcome. If wormian bone is found in association with other congenital anomalies, fetal karyotyping with molecular biology as well as complementary in utero investigation (CT scan and/or magnetic resonance imaging) should be carried out to ensure appropriate diagnosis and management. Histologic evaluation of the chondral plate should be carried out in those cases undergoing termination of pregnancy with suspected or superimposed skeletal dysplasias. Radiographs, 3D CT and/or magnetic resonance imaging, and photographic images should be obtained at delivery and DNA should be collected in a bio-bank for subsequent analysis with a Comparative Genomic Hybridization (CGH) array to search for microdeletions, as there is a growing body of knowledge using this novel genetic investigation.12–14
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.