
Abstract
Objective:
The study assessed optic nerve diameter (OND) and clinical biomarkers in patients with poorly controlled diabetes compared with healthy nondiabetic volunteers.
Materials and Methods:
There were 1320 adult participants recruited to the study. The cohort was divided into 600 Type 2 diabetic (DM II) patients and 720 apparently healthy, nondiabetic volunteers. The OND was measured using a high-resolution dedicated ultrasound device (Sonoace 5500; Medicol, Medison, Miami, FL, USA) with a 10-MHz linear array transducer. Subjects were examined in a supine position with their eyes closed. Three measurements of the OND were taken and the average recorded. Hemoglobin A1c concentration and lipid profiles were determined using Bio-Rad Diamat analyzer (Bio-Rad, Hercules, CA). Body mass index and age were matched for both cohorts for comparativeness.
Results:
The mean OND of the DM II patients was 3.10 ± 0.14 mm (range of 2.6–4.0 mm), which was significantly (P < .05) lower than the control volunteers (4.22 ± 0.15 mm). The OND demonstrated a negative significant correlation with HA1c, duration of diabetes and low-density lipoprotein cholesterol level (P < .05). Lipid profiles, blood urea, serum creatinine, and hemoglobin A1c showed statistical difference between diabetics and control subjects.
Conclusion:
Poorly controlled DM II patients may have significantly narrower OND than nondiabetic patients. This imaging biomarker has the potential to transform visual care for DM II patients.
The incidence of diabetes mellitus (DM) is growing rapidly worldwide,1–3 with the global estimate at 171 million as of 2020. 4 In Nigeria, more than 30% of the elite population including decision makers are diabetic,5,6 and the risk of developing associated complications and mortality is higher with poorer hyperglycemia control. 7 Several studies have been tailored toward early diagnosis and mitigation of complications of DM.8–10 Type II diabetes mellitus (DM II) is a chronic disease typified by impaired metabolism of glucose and other energy yielding fuels. It is a collection of diseases with abnormal insulin deficiency and resistance, leading to chronic hyperglycemia and distorted lipid metabolism.7,11 DM II increases the risk of chronic kidney disease, cardiovascular conditions, and complications in several other human organ systems.10,12 Studies suggest that in most developing countries, DM accounts for one in ten deaths in economically productive individuals.13,14
DM II is the leading cause of blindness in persons aged 20 to 70 years, and statistics indicates that diabetics are 20 times more likely to develop blindness, than nondiabetic subject.15,16 The effect of blindness and the costs of affording relevant testing are cumbersome on the diabetics and family members. 17 The optic nerve is one important structure affected by DM II. 4 It is an extension of the forebrain, which conveys afferent fibers, from the ganglion cells of the retina and transmits visual signals to the brain. Its fibers are lined with myelin where most of the axon terminate in the lateral geniculate nucleus and information relayed to the visual cortex.18,19 The optic nerve and small blood vessels of the eye can be damaged when blood sugar levels are out of control. Changes involving the optic nerve may serve as a useful indicator of impending or existing optic nerve neuropathy, in diabetic patients. These changes can affect the morphometry of the optic nerve. Sonography is useful in optic nerve evaluation and can detect any changes in its morphometric value. 11 With the rising incidence of DM, and the complications that elicit social and psychological burdens on patients and society, measures toward early detection are vital. The associated clinical complications and subsequent prevention of blindness would be of great value to diabetics and the society. The integration of optic nerve diameter (OND) as an imaging biomarker into the routine diagnostic evaluation of diabetic patients could significantly improve visual care, among this group. The research objective was to determine if any imaging difference exists in the OND and clinical biomarkers, in patients who have poorly controlled DM II, compared with nondiabetic patients.
Materials and Methods
This study recruited 1320 adults, of which 600 were DM II patients from a Nigerian teaching hospital clinic and 720 apparently healthy, nondiabetic volunteers. Only diabetic patients with fasting blood sugar of 144 mg/dL or more were included in this study. Patients with type I DM were excluded from the study. The control group consisted of apparently healthy adult volunteers, who came fasting. On arrival to the imaging room, the investigation was explained to patients and volunteers. Only the patients and volunteers who gave their informed consent were recruited to the study. The OND was measured using a high-resolution dedicated ultrasound equipment system (Sonoace 5500; Medicol, Medison, Miami, FL, USA) and a 10-MHz linear array transducer. The ultrasound equipment system produced a 3 × 4 cm field of view and an axial resolution of 0.5 mm, as well as a lateral resolution of 1–2 mm. The mechanical index (MI) was kept below 0.23. The ultrasound quality control measures included a quality assessment of images and a repetition of ultrasound measurements. Ethical approval for the study was obtained from the Ethical Research Committee within the Department of Radiography and Radiological Science, at the University of Calabar.
Data Synthesis
For each investigation, subjects were placed in the supine position, lying still and holding their eyes closed. Coupling gel was placed on the closed eyelids, and a 10 MHz transducer was softly placed on the upper temporal eyelid, in an axial plane. This section provided a transverse view of the globe and the post bulbar area. Thereafter, the ultrasound output intensity and overall gain were adjusted to achieve an optimum level of contrast, between the echogenic post bulbar fat and the hypoechoic optic nerve complex. In this view, the optic nerve sheath appeared as a well-defined homogenous low-reflection band and extends posteriorly from the base of the bulb. The OND was measured perpendicular to the vertical axis of the scanning plane as a horizontal distance between the two walls of the nerve sheath (see Figures 1 and 2). All measurement was performed by a single sonographer, with 15 years of sonographic experience. Three measurements were taken for the right and left,. The fasting blood sugar level was assessed using a digital glucose meter, Accu-check active (serial number GG03111364, Roche Group, UK). Hemoglobin A1c concentration and lipid profiles were determined in the laboratory similarly using Bio-Rad Diamat analyzer (Bio-Rad, Hercules, CA). The tip of the thumb was pricked with a lancet after the area was cleaned with cotton wool and spirits. A drop of blood from the thumb was placed on the strip of the Bio-Rad Diamat analyzer and the hemoglobin A1c concentration and lipid profiles were determined electronically.
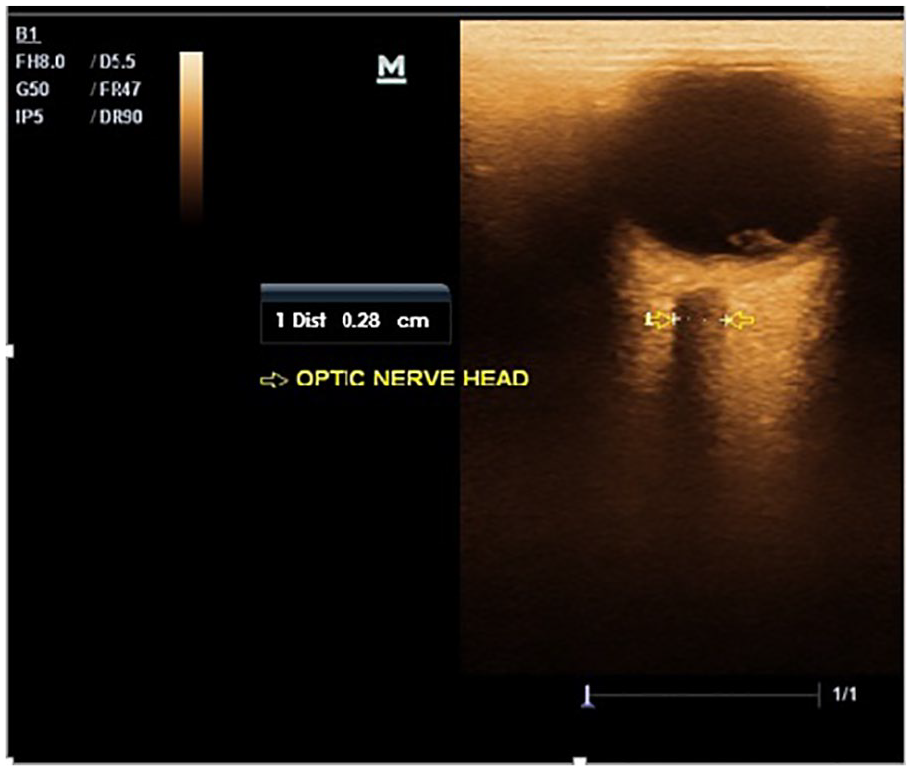
A sonographic image with measurement calipers showing the measurement of OND, in a poorly controlled Type II diabetic patient. OND, optic nerve diameter.
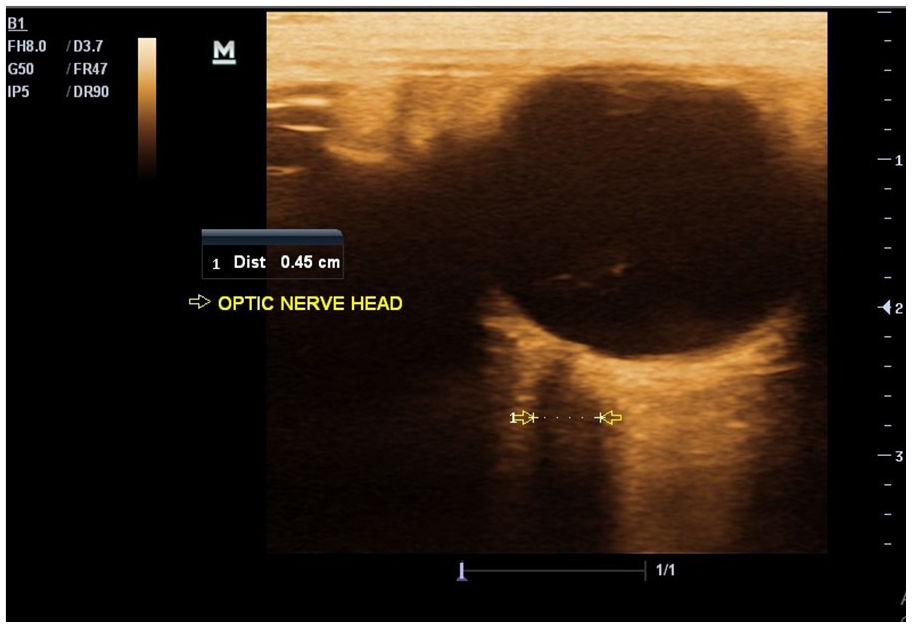
A sonographic image with measurement calipers showing the measurement of OND, in a nondiabetic volunteer. OND, optic nerve diameter.
Statistical Analysis
Normality of the data set was assessed using both the Shapiro-Wilk and Kolmogorov-Smirnov tests, and the results indicated that the data were normally distributed. Descriptive statistics were used to determine the means and ranges of the various variables measured in both the DM II patients and the nondiabetic volunteers. Mean ONDs for both groups were compared using the Student t test, and the level of statistical significance was set at P < .05. A Pearson correlation was used to determine the strength of association between OND and the clinical variables. The analysis was done using the Statistical Package for the Social Sciences (SPSS Inc, Chicago, IL, USA) version 21.0, and all statistical significance was determined a priori at P < .05.
Results
A subset, of the study participants, consisted of 600 poorly controlled DM II patients and 720 apparently healthy volunteers. The subset of DM II patients comprised 236 males with a mean age of 63.6 ± 7.4 years and a range of 35–75 years. There were also 214 females with a mean age of 58.3 ± 9.2 years, ranging from 37 to 72 years. The demographics of the normal volunteers consisted of 334 males with a mean age of 57.8 ± 10.3 years, within a range of 31–73 years. There were also 386 females with a mean age of 51.7 ± 13.6 years, within a range of 34–76 years. The mean OND in the DM II patient group was 3.10 ± 0.14 mm (within a range of 2.6–4.0 mm), which was significantly (P < .05) lower than the control volunteer group (4.22 ± 0.15 mm). In Table 1, the demographics and laboratory values of DM II and healthy volunteers are provided. Most of the laboratory variables (high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, blood urea, serum creatinine, hemoglobin A1c, urine albumin excretion, and fasting plasma glucose) were statistically different between the poorly controlled DM II patients and health volunteers. However, body mass index did not differ significantly between the two groups. Participants with a significant reduction in optic nerve size were DM II patients with a high hemoglobin A1c concentration. Results showed that OND demonstrated a significantly moderate negative correlation with HbA1c (r = −0.53; P < .05), while a significantly weak negative correlation existed between OND and a fasting blood sugar (r = −0.17; P < .05). The OND and duration of DM II also had a significantly weak negative correlation (r = −0.33; P < .05) (see Table 2). The ONDs varied with Hemoglobin A1c percent concentrations as follows: 3.87 cm (6.5%–7.4%); 3.44 cm (7.5%–8.4%); 3.08 cm (8.5%-9.4%), and 2.46 cm (9.5%–10.4%).
The Demographic and Laboratory Values of DM II Patients and Nondiabetic Volunteers.
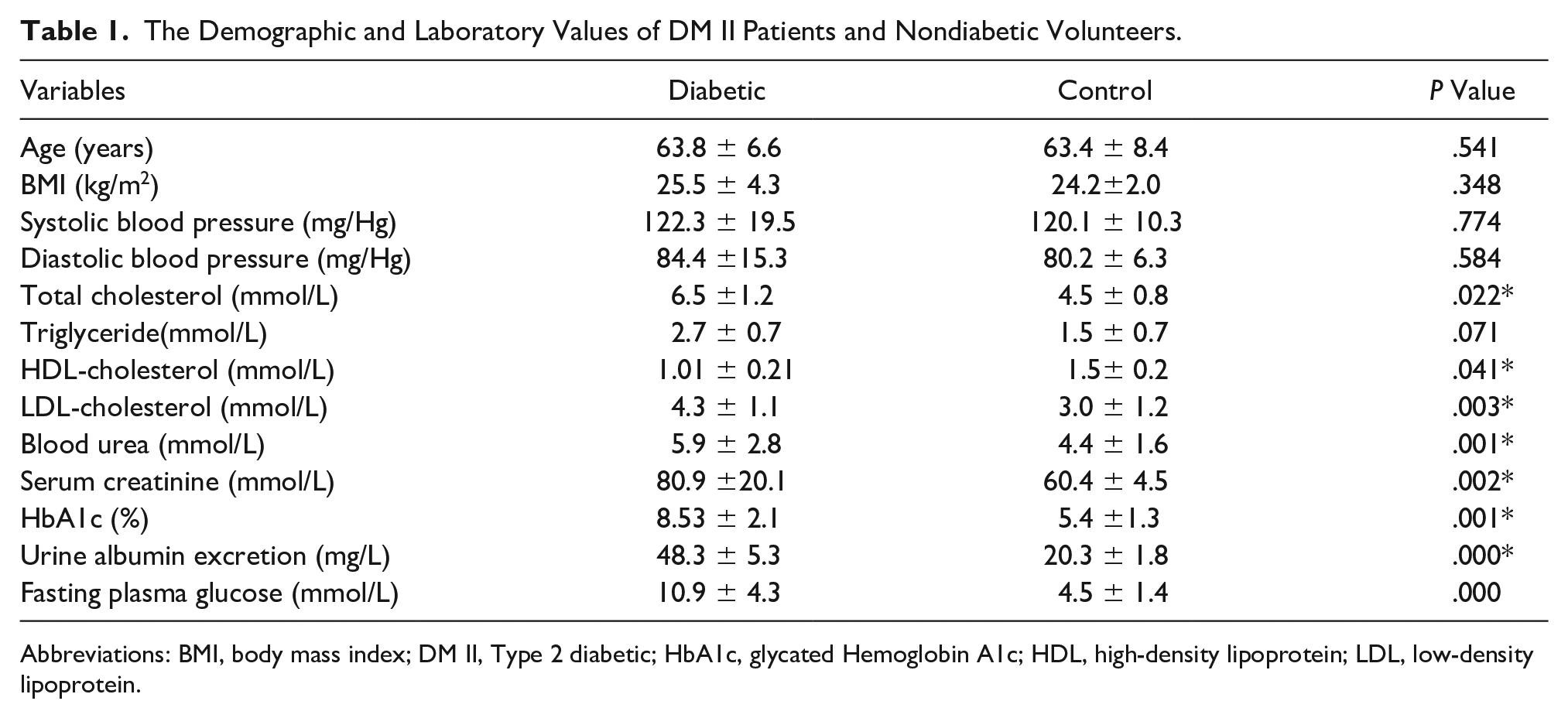
Abbreviations: BMI, body mass index; DM II, Type 2 diabetic; HbA1c, glycated Hemoglobin A1c; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
The Strength of Association Between OND With the Clinical Biomarkers Collected From DM II Patients.
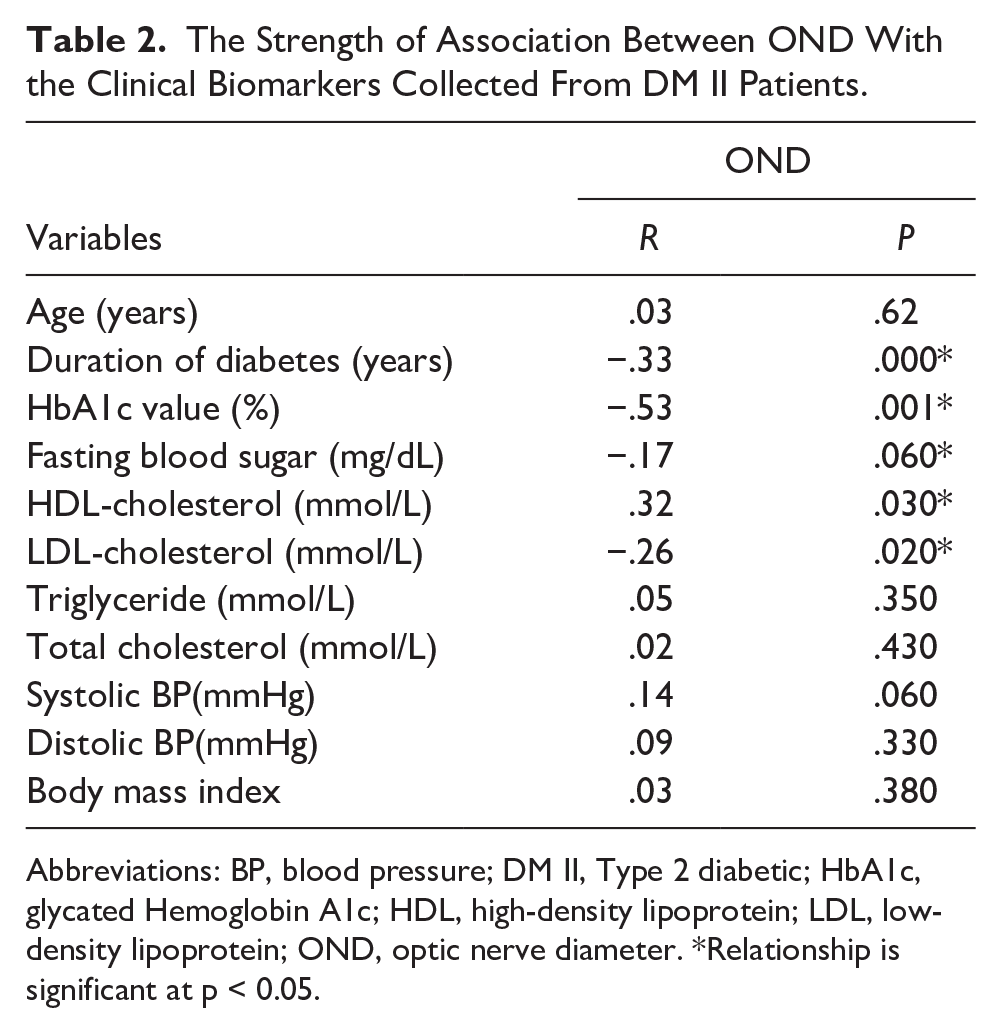
Abbreviations: BP, blood pressure; DM II, Type 2 diabetic; HbA1c, glycated Hemoglobin A1c; HDL, high-density lipoprotein; LDL, low-density lipoprotein; OND, optic nerve diameter. *Relationship is significant at p < 0.05.
Discussion
Optic nerve involvement is a typical complication with diabetes and the pathogenesis has been documented in recent studies.4,20 The present study determined the OND and related values with some clinical biomarkers in adults with both poorly controlled DM II patients and their healthy counterparts. The mean OND for the DM II subset of participants was 3.10 ± 0.14 mm, within a range of 2.6–4.3 mm. This value was observed to be significantly lower than that of the healthy volunteers (see Table 3) and was comparable to a study conducted by Osman et al, 18 with a cohort of diabetic Sudanese. The lowered OND in the diabetic patients, according to recent studies, has been linked to degenerative changes from alterations in metabolic pathways, oxidative stress, hemodynamic changes, and ischemia, attributed to DM.4,20–23 Skillern and Lockhart 24 had previously documented this finding with a series of fourteen uncontrolled diabetics, who they observed had developed optic nerve atrophy, as well as a few cases of retinopathic changes. Recent studies have underpinned a sorbitol pathway of glucose metabolism in the etiology of diabetic complications.
The Age Distribution of OND in the DM II Patients and Nondiabetic Volunteers.
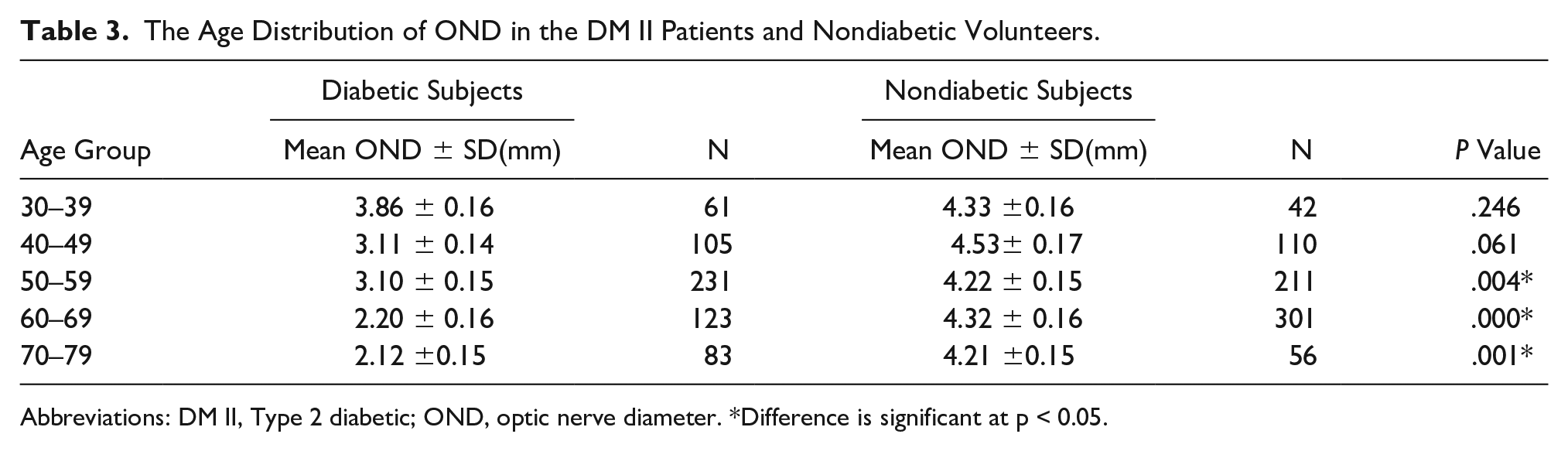
Abbreviations: DM II, Type 2 diabetic; OND, optic nerve diameter. *Difference is significant at p < 0.05.
There are clinical manifestations of optic nerve changes with diabetic retinopathy (DR), such as diabetic papillopathy, neovascularization of optic disk, and optic nerve atrophy imposed by metabolic alterations related to DM, production of advanced glycation products (AGEs), oxidative stress, and hemodynamic changes.4,20 In addition, available evidence highlights pathways such as a vascular phenomenon related to occlusion of optic nerve nutrients, capillary changes in the superficial optic disk, and toxic metabolic changes to cause optic nerve involvement, in uncontrolled DM.20,25
When comparing OND values, in the present study, between the subsets of participant, according to age, it yielded a significant difference between DM II and the healthy volunteers, in those 60 years and older. The DM II group had lower dimensions of OND than the control; however, for participants in their 40s and 50s, findings revealed a statistical homogeneity. In addition, the present study revealed that age did not influence OND among the DM II patients, as there was no statistical relationship established between these two variables. This outcome differs with the results of Sahar and Osman, 18 which revealed a linear relationship between diabetic patient’s age and optic nerve measurement. The current study patients with a significant reduction in OND were diabetics with high glycated Hemoglobin A1c concentration (HbA1c), while nondiabetic volunteers had significantly lower HbA1c values and higher OND values (see Table 1). It turned out that OND reduced moderately with higher values of HbA1c in the DM II group (see Table 2), and this result would suggest that the impact of DM on OND and its association with HbA1c levels, is evident compared with similar research.11,20,26 HbA1c, an indicator of blood glucose concentrations over the preceding 3 months, is useful for characterizing dysglycemia in population studies and for assessing the severity of DM and diabetic optic neuropathy.4,11 In a study by Hua et al., 20 they examined the relationship between the level of HbA1c, and progression of DR in a large cohort of diabetic persons. Their results showed a positive relationship between incidence and progression of retinopathy and glycated hemoglobin, after controlling for duration of diabetes, age, sex, and baseline retinopathy. Hua et al. added that glycated hemoglobin concentration seemed to explain most of the excess mortality risk with diabetes. HbA1c is a well-known predictive biomarker with regard to severity of DM and a propensity for complications. Its relationship with OND in the present study suggests that OND could be a useful predictive index for DM severity and risk of visual complication, and could transform care for DM II patients. There are instances where the HbA1c value can be influenced by other nonglycemic factors, such as any defect in the concentration of hemoglobin, conditions that lengthen the red blood cell lifespan, and iron deficiency.11,27 If this happens, results may become misleading and the patient’s management compromised there might be need to integrate such morphometric biomarker as OND to determine severity and improve care for DM II patients.
The duration of DM, explored in this study, showed a weak negative correlation with OND, after controlling for other variables for patients with poorly controlled diabetes (see Table 2). Findings in this regard were in agreement with a study conducted by Osman et al., 18 however, was opposed to result by Eda et al., 10 who argued that OND did not change with severity of DM. In their study, it was stated that pre-treatment of the OND for patients diagnosed with one of the acute hyperglycemic complications was not different from their healthy counterparts. They however noted that optic nerve sheath values increased with treatment of their patients. Some evidence has been underpinned to low levels of high-density lipoprotein (HDL) cholesterol in type 2 diabetes mellitus, albeit there are conflicting opinions.26,28 In the present study, circulating HDL levels were statistically higher in the healthy volunteers compared with the DM II patients (see Table 1). An observed decrease in the amount of circulating HDL cholesterol in these DM II patients is in line with related studies.7,26 It was noted that lowered HDL produced corresponding reduction in OND, which precedes retinal impairment. 7 According to Tabara et al., 29 high HDL cholesterol triggers anti-diabetic and atherogenic pathways including reversing cholesterol transport, anti-oxidation, and anti-inflammatory capacities. A significant reduction in diabetics’ HDL has been documented for patients suffering with diabetic optic neuropathy (DON) compared with those without DON. 20 Since OND has a direct association with HDL cholesterol, which is a predictor of DON incidence, it could present a similar predictive purpose in optic neuropathy incidence in a diabetic cohort, as an important in vivo approach.
The level of triglycerides in the current investigation was statistically comparable in both groups, albeit, in discordance with similar studies.26,30 The current study did not substantiate the association between triglycerides and DM as revealed in related studies. The expectation was a statistical association between triglycerides level and OND in the study, but the results did not substantiate it. Several factors, including method of data collection and sample size, could have undercut this outcome. One of the main factors used for diabetes assessment is serum level of low-density lipoprotein–cholesterol (LDL-C) and it is important to keep it less than 100 mg/dL in diabetic patients. The LDL cholesterol showed a weak negative correlation with OND in the DM II patients and was increased in the DM II patients compared with the controls, which agrees with related studies.31,32 The present study also revealed that systolic blood pressure (SBP) and diastolic blood pressure (DBP) were comparable in both groups but both parameters showed an insignificant relationship with OND. The current study findings were in discordance with those of Shiva Raj. 11 Blood urea, urine albumin excretion, and serum creatinine were found to be increased in the DM II patients compared with the nondiabetic patients, in the present study. These present results corroborate other similar research studies.33,34
Several factors including lifestyle have shown significant association with the development of complications of DM.35,36 Thus, good glycemic control is very essential in preventing diabetic complications. The alteration in the dimensions, the structure of OND, as well as other diabetic complications such as retinopathy, neuropathy, and macrovascular diseases can be traced to glycation reactions between reducing sugar and several precursors such as collagen and lipoproteins, among DM II patients.4,20,26 Recently, few studies have been conducted to elucidate damage due to DM and DR in the optic nerve and central visual pathway. In patients with DM, hyperglycemia enhances the synthesis of new collagen and accumulation of glycation end-products which accelerates the changes noted in OND in diabetic patients. 37 Complications from poor management of DM are on the increase. Long-term prospective nonrandomized study of DM control and complications has shown a 10-fold increase in the prevalence of diabetic complications such as retinopathy, in poorly controlled patients. Very few studies have addressed the usefulness of OND in risk stratification for DR, in low-resource settings. It may be critical to integrate OND assessment to provide timely recognition and management of patients with poorly controlled DM and who are at greater risk of DR progression. One limitation to this study was that the research design was a convenient case-control, and may not be generalizable beyond this group. Therefore, a random assignment of patients to a similar study would provide more power and effect in a replication of this work.
Conclusion
In this particular cohort, poorly controlled DM II patients had a significantly narrower OND than their control counterparts. This may suggest that one of the reasons for poor vision among diabetic patients is a reduction in OND.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.