
Abstract
This is a case study of a 47-year-old Caucasian male whose chief concern was left lower leg swelling for 1 month. A unilateral lower extremity venous duplex examination was performed. The results concluded that the distal femoral vein was occluded to the distal popliteal vein. Incidentally, a hypoechoic region in the distal thigh near the distal femoral artery was noted by the technologist. The patient was placed on anticoagulation and was told to return for further examination if there was no relief. Three months later, the patient continued to experience lower left leg swelling and returned for another sonogram. The hypoechoic region was seen again in the distal thigh and remained occluded. A computed tomographic arterial (CT-A) and magnetic resonance imaging (MRI) were ordered for further investigation of the hypoechoic area. The CT-A and the MRI revealed the presence of a mass in the distal thigh. The mass was biopsied and diagnosed as a leiomyosarcoma, grade 1. The mass caused the compression and occlusion of the distal femoral vein. The mass was removed, along with a portion of the distal femoral artery due to involvement of the artery within the mass. The artery was repaired with a graft.
Keywords
A 47-year-old Caucasian male presented to the vascular sonography laboratory, and his chief concern was left lower leg swelling, for 1 month. No prior examinations had been ordered or performed. The patient was in good health and was an active middle-aged man. A unilateral lower extremity venous (LEV) duplex examination was performed.
Case Report
During the examination, normal blood flow and compressions were visualized in the proximal and mid femoral vein of the left leg. However, the distal femoral vein was occluded from the distal thigh region through the distal popliteal vein (Figure 1). The posterior tibial veins were visualized and were fully compressible. The peroneal veins were unable to be visualized. Incidentally, a hypoechoic region in the distal thigh near the distal femoral artery was noted by the technologist. Results from the radiologist report concluded that an occlusive, mildly echogenic thrombus was present within the distal superficial femoral vein (SFV) and popliteal veins. The vessels were both surrounded by the sarcoma; thus, the deep venous thrombus (DVT) was due to extrinsic compression. The patient was placed on anticoagulation and was told to return for further examination if there was no relief.
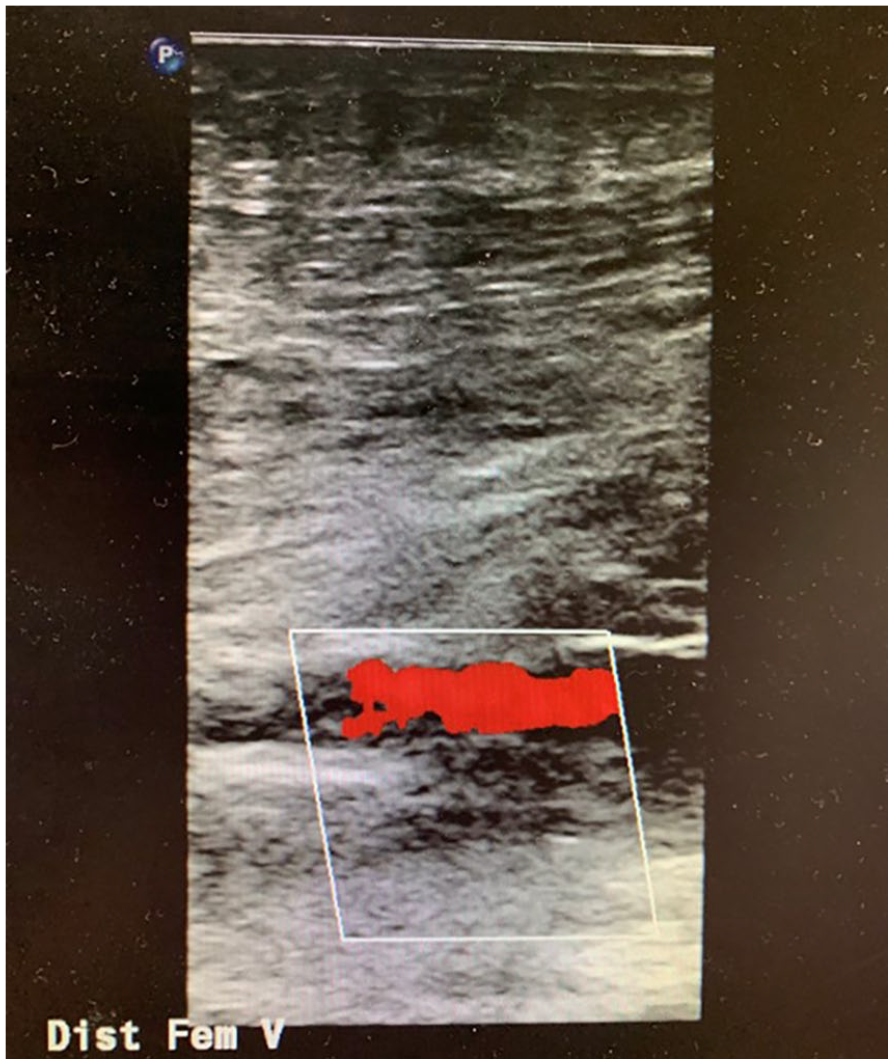
Color Doppler image from the first sonographic examination, showing occluded distal femoral vein. In this image, only arterial flow was noted with color Doppler.
Three months later, the patient continued to experience lower left leg swelling and returned for another sonogram. The hypoechoic region was again seen in the distal thigh, and the distal femoral and popliteal veins remained occluded (Figure 2). The radiologist, suspecting a mass, ordered a magnetic resonance imaging (MRI) study (Figure 3) and a computed tomographic arterial (CT-A) study (Figure 4), for further investigation of the hypoechoic area seen on the sonogram.
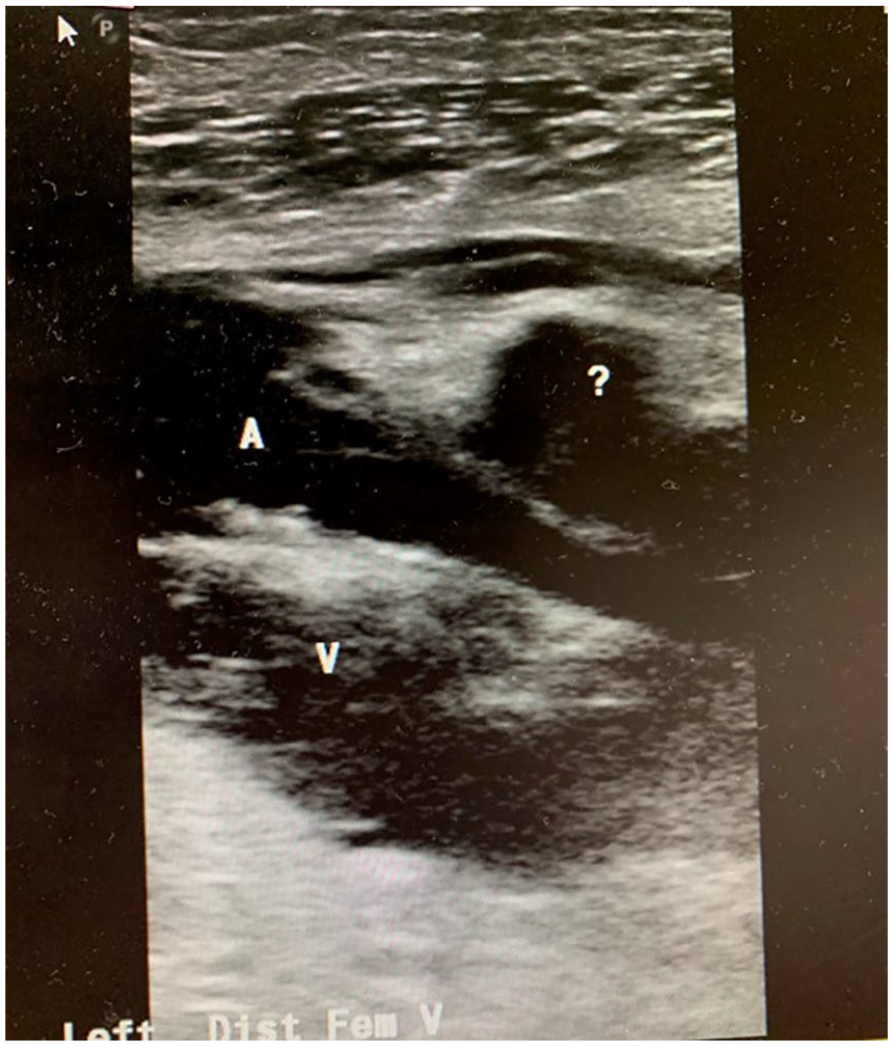
A gray-scale sagittal view from the second sonogram showing distal superficial femoral artery (A), occluded distal femoral vein (V), and hypoechoic region of suspicion (?).

A selected magnetic resonance imaging view of the leiomyosarcoma mass, located in the distal thigh.
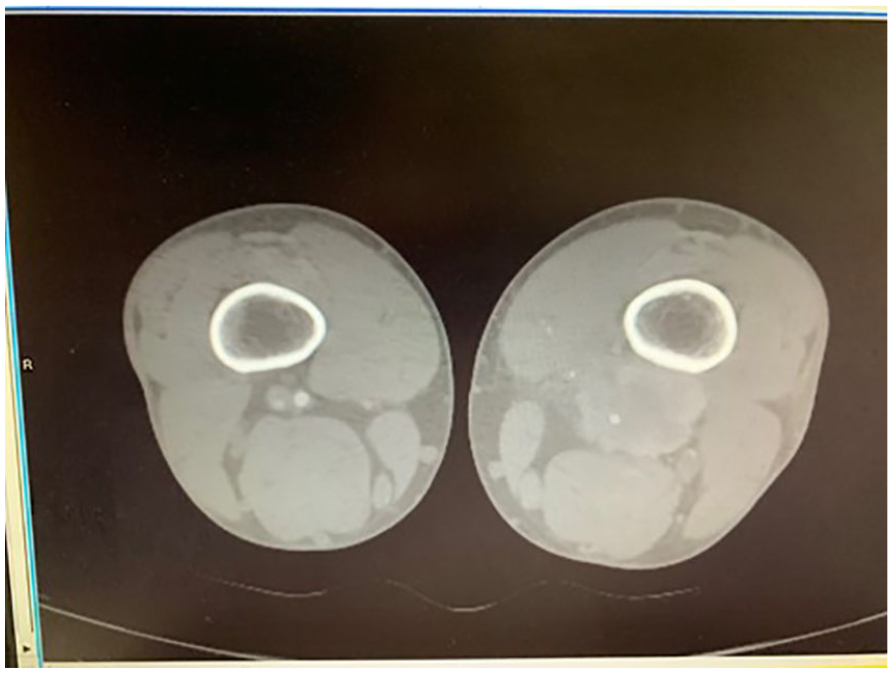
A computed tomographic arterial image of the affected area, which demonstrates the leiomyosarcoma mass impinging on the distal femoral vein.
After the MRI revealed that a mass was present in the distal thigh, the mass was biopsied and was diagnosed as a leiomyosarcoma (LMS), grade 1. The mass had caused the compression and occlusion of the distal femoral vein. The mass was subsequently removed, along with a portion of the distal femoral artery due to its involvement with the mass. The artery was repaired with an in situ graft using the contralateral greater saphenous vein (GSV) and an additional stent at the distal anastomosis.
Following successful vascular surgery, the patient has had two follow-up LEV sonographic examinations. The results revealed that flow was still not visualized in the distal femoral and popliteal veins. The arterial flow was biphasic and flowing well through the graft. The patient will receive follow-up sonographic examinations biannually for the next few years.
Discussion
LMS is one of the more common sarcomas, but it is still a rare type of cancer that affects smooth muscle tissue. 1 LMS is a type of soft tissue sarcoma and makes up between 10% and 20% of soft tissue sarcoma cases. LMS is an aggressive cancer, and tumors are most commonly found in the abdomen but can occur anywhere in the body, including the uterus. 2 Other common sites include blood vessels and skin. LMS can also affect the large blood vessels, particularly the inferior vena cava. LMS is more common in adults than children. It is estimated that only about 20–30 children are diagnosed with LMS in the United States per year. LMS of the uterus affects about 6 per 1 million people per year in the United States. 2
Removal of the tumor is the main course of treatment. If the mass has metastasized, the patient can receive chemotherapy and radiation. Advanced stage LMS is incurable with current systemic antitumor therapies. 3 In this case, the vascular surgeons removed a portion of the superficial femoral artery along with the mass. A bypass graft using the great saphenous vein was then performed to restore flow through the arterial system.
Conclusion
The technologist had mentioned their suspicions of the possibility of a mass being present in the original report. It is important to be sure to mention an incidental finding, such as a “hypoechoic region of interest.” Sonographic examinations are crucial to overall in-patient care, and technologists are the eyes and ears for the radiologist. Technologists need to look at the “whole picture,” that is, above and below the specific region of interest, because as in this case, the artery appeared as if something was compressing it. Finally, it is also important to be sure to listen to the patients’ chief concerns as to where the pain originates and to be sure to image that area.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.