
Abstract
Objective:
Magnetic resonance imaging (MRI) has been established as the gold standard imaging technique for assessing knee joint pathologies. However, high-resolution sonography (HRS) is affordable, easily available, cost-effective, and can be used for knee joint assessment. This study was conducted to assess the diagnostic yield of HRS in the evaluation of knee joint pathologies compared with MRI.
Materials and Methods:
In the study, 103 patients, with symptomatic knee pain, were included. HRS was performed followed by MRI. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were calculated. Kappa values were calculated to assess the performance of HRS compared with MRI.
Results:
The most frequent pathologies observed on HRS were knee joint effusion (84%) followed by medial meniscal (43%) and lateral meniscal (26%) tear.
Conclusion:
HRS demonstrated good diagnostic accuracy in diagnosis of knee joint pathologies as compared with MRI. Therefore, HRS could be utilized as a screening tool for detection of knee joint pathologies.
The knee joint is commonly assessed joint for internal derangement. A myriad of injury mechanisms and a wide variety of pathological disorders affecting the various intra-articular structures of the knee joint are a significant cause of pain and instability.1,2
Knee injuries are especially common and detrimental to high quality of life and account for a significant proportion of musculoskeletal trauma encountered in the emergency department. 3
As the stability of the knee joint relies upon the strong ligaments (cruciate—anterior and posterior; collateral—medial and lateral), muscles, tendons, and menisci (medial and lateral) that bind the femur and the tibia together, the same are more prone to injury and therefore should be assessed properly for their anatomy and pathology.2,4
Magnetic resonance imaging (MRI) is a noninvasive, gold standard imaging technique which is indispensable for assessing the different kinds of knee pathologies and injury occurring in intra-articular knee structures along with the extra-articular ligaments, tendons, and periarticular muscles. In recent times, MRI has been shown to have a very important part in diagnosing various types of knee pathologies, since it is radiation free and has multiplanar capabilities without exposure of the patient to harmful radiation.5–7 However, it is costly, not widely available, and has some contraindications.
High-resolution sonography (HRS) is noninvasive, affordable, easily available, and allows for dynamic evaluation. It is well accepted by the patients and does not have any major contraindications like MRI. It can easily be carried out in claustrophobic patients too. Few studies have shown that knee joint pathologies such as joint effusion, collection of bursal fluid, meniscal tears, collateral and cruciate ligament tears, tears of tendons, bursitis, occult fractures, and tendonitis can be diagnosed by HRS.7,8 HRS also provides high spatial resolution images of superficial structures of the knee joint, compared with MRI. 9
The purpose of this study was to establish the role of HRS for evaluation of knee joint pathologies, compared with MRI. The study hypothesis was that HRS can be used as a primary screening tool, for the evaluation of knee joint pathologies.
Materials and Methods
This was a hospital-based prospective observational study that comprised 103 patients. The inclusion criteria were based on complaints of unilateral or bilateral knee joint pain/instability. The patients were referred for MRI of the knee, to the radiology department, with complaints of pain in the knee joint, as well as with or without history of preceding trauma. The participation of the patient in the study was purely voluntary, and informed consent was obtained prior to conducting HRS, on all the patients. Patients who were unwilling to participate in the study or had contraindications to MRI were excluded. MRI of the symptomatic knee was done followed by HRS. The images were interpreted by two radiologists, each of whom had no knowledge of the imaging findings. One radiologist performed all the HRS and the other interpreted all the MRIs. Both radiologists had at least 8 years of experience in performing HRS and MRI.
MRI Technique
The patients were examined using 1.5T (Siemen’s Magnetom Avanto Tim + Dot system). The following images were acquired in the following sequences for knee joint analysis: PD: axial, coronal, and sagittal with 3.5-mm slice thickness and interslice gap of 1 mm; T1W axial and coronal, T2W sagittal and T2 GRE sagittal with 3.5-mm slice thickness and interslice gap of 1 mm; and short tau inversion recovery (STIR) coronal 3.5-mm slice thickness and interslice gap of 1.2 mm. 3D sequences and cine loops were not performed routinely.
HRS Technique
After obtaining informed consent from the patient, HRS was performed using a linear transducer with a frequency ranging from 4 to 13 MHz (Siemens Acuson S3000, Siemens Acuson S2000, Siemens Acuson Juniper). The patients were placed in the supine and prone positions. Four approaches were performed: anterior, posterior, medial, and lateral for the assessment of knee joint pathologies.1,4,10 Depth and gain were adjusted to acquire acceptable image quality. Both longitudinal and transverse sonographic images were obtained.
The anterior aspect of the knee was examined with the patient in the supine position and slight knee flexion of approximately 20° to 30°, by keeping a rolled towel under the knees. The key structures that were examined in the anterior aspect of the knee were the extensor group (quadriceps tendon, patella, and patellar tendon), prepatellar and infrapatellar bursa, suprapatellar synovial recess, joint recesses, and femoral articular cartilage.1,4,11
For evaluation of the anterior cruciate ligament (ACL), the transducer was placed over the patellar tendon in the suprapatellar region in the sagittal imaging plane, and for evaluation of the femoral cartilage, the transducer was placed in the same position, for the transverse imaging plane.1,4,11
For the evaluation of the posterior knee, the patient was placed in the prone position, with the knee extended. The key structures which were evaluated in the posterior knee were the presence of Baker’s cyst, the posterior horns of the menisci (medial and lateral), the posterior cruciate ligament (PCL), and the popliteal neurovascular bundle.1,4,11
For the evaluation of the medial knee, the patient was examined in the supine position with the hip rotated externally and knee flexed to 30° to 45°. The structures which were evaluated in the medial aspect of the knee were the medial collateral ligament (MCL), the body and anterior horn of the medial meniscus, medial tibiofemoral joint space, and the pes anserine tendon complex (sartorius, gracilis, and semitendinosus).1,4,10,11
For evaluation of the lateral knee, the patient was examined in the supine position with hip rotated internally with the slight flexion of the knee. The key structures which were evaluated in the lateral knee were the iliotibial band (or tract), lateral collateral ligament (LCL), common peroneal nerve, popliteus, lateral tibiofemoral joint space, and anterior horn and body of the lateral meniscus.1,4,10,11
Statistical Analysis
Images were independently interpreted by two different radiologists with at least 8 years of experience, and the findings were recorded on a predefined proforma. The data were analyzed statistically using SPSS software v20. The P value of less than .05 was considered statistically significant. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were calculated.
MRI was regarded as the gold standard examination for various knee joint pathologies. The agreement between studies of HRS and MRI was calculated using the kappa (κ) coefficient. Strength of the kappa coefficient was interpreted in the following manner: 0.01 to 0.20, slight; 0.21 to 0.40, fair; 0.41 to 0.60, moderate; 0.61 to 0.80, substantial; and 0.81 to 1.00, near perfect. 12 - 14
Results
This prospective observational study was conducted over a period of 1 year. There were 103 patients, with suspected knee joint pathologies, evaluated with imaging. In this study, majority (n = 30) of the patients were in the age group of 21 to 30 years of age, with a mean age of 32.9 years (Table 1). Seventy-six (76%) patients were males and 24 (24%) were females. Seventy-four patients gave history of preceding trauma to their knee.
Age Distribution of Study Patients.
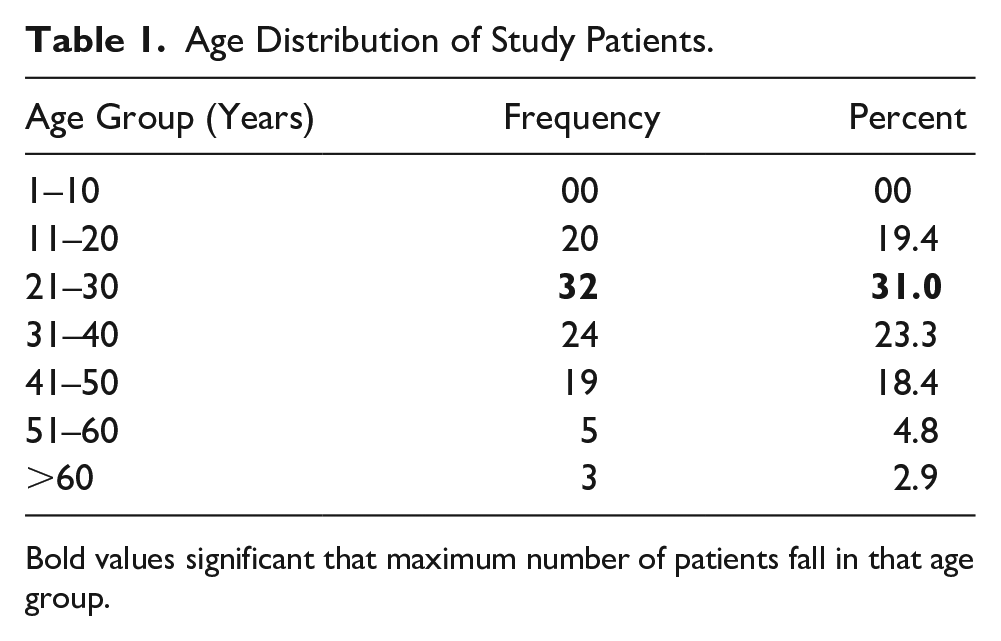
Bold values significant that maximum number of patients fall in that age group.
Anterior Tendons of Knee
There were four cases of quadriceps tendinopathy and three cases of patellar tendinopathy, observed with HRS, while MRI demonstrated six and four of these cases, respectively.
Substantial agreement with coefficient κ = 0.79 was noted between HRS and MRI in detection of quadriceps tendinopathy, and it was found to be significant statistically (P < .001).
Almost perfect agreement with coefficient κ =0.85 was noted between HRS and MRI in detection of patellar tendinopathy, and it was also found to be statistically significant (P < .001).
HRS demonstrated accuracy, sensitivity, and specificity of 98%, 66.6%, and 100.0%, respectively, in detection of quadriceps tendinopathy and 100.0%, 75.0%, and 99%, respectively, in detection of patellar tendinopathy. However, sample size with positive cases was small to be able to accurately comment on the same.
Effusion
Knee joint effusion was the most common finding detected in 86 patients, with HRS and 90 patients with MRI. Substantial agreement with coefficient κ = 0.67 was noted between HRS and MRI in detection of knee joint effusion, and it was found to be significant statistically with P < .001.
HRS demonstrated sensitivity, specificity, and accuracy of 92.2%, 90% and 92%, respectively, in detection of effusion.
Meniscal Tears
Out of the 103 patients, a total of 26 lateral meniscal tears and 43 medial meniscal tears were detected with HRS and 50 medial meniscal tears and 32 lateral meniscal tears were detected with MRI. Almost perfect agreement (κ = 0.82) was seen between HRS and MRI in detection of medial meniscal tear and substantial agreement (κ = 0.61) was seen between HRS and MRI in detection of lateral meniscal tear.
HRS demonstrated sensitivity, specificity, and accuracy of 84.0%, 98.0, and 91%, respectively, in detection of medial meniscal tear and 65.6%, 92.7%, and 84.1%, respectively, in detection of lateral meniscal tear.
Cruciate Ligament Tears
Out of the 103 patients, a total of 7 ACL tears and 6 PCL tears were detected on HRS, as well as 20 ACL tears and 11 PCL tears were detected with MRI. Slight agreement (κ = 0.13) was seen between HRS and MRI, in detection of an ACL tear and substantial agreement (κ = 0.55) was seen between HRS and MRI in detection of a PCL tear. Due to the small number of cases showing cruciate ligament tears, sensitivity, specificity, and accuracy values which were calculated were unreliable.
Collateral Ligament Tears
Out of the 103 patients, a total of ten MCL tears and seven LCL tears were detected on HRS. There were eight MCL tears and seven LCL tears detected with MRI. Substantial agreement (κ = 0.63) was seen between HRS and MRI, in the detection of an MCL tear and almost perfect agreement (κ = 0.83) was noted between HRS and MRI in detection of an LCL tear.
Again, due to the small number of cases showing cruciate ligament tears, sensitivity, specificity, and accuracy values which were calculated were unreliable.
Baker’s Cyst
Baker’s cyst was present in five patients on HRS and in six patients on MRI. Almost perfect agreement (κ = 0.90) was seen between HRS and MRI in the detection of Baker’s cyst.
The most common pathologies observed on HRS were knee joint effusions (84%) followed by medial meniscal (43%) and lateral meniscal (26%) tears (Table 2).
Knee Pathologies on HRUS and MRI.
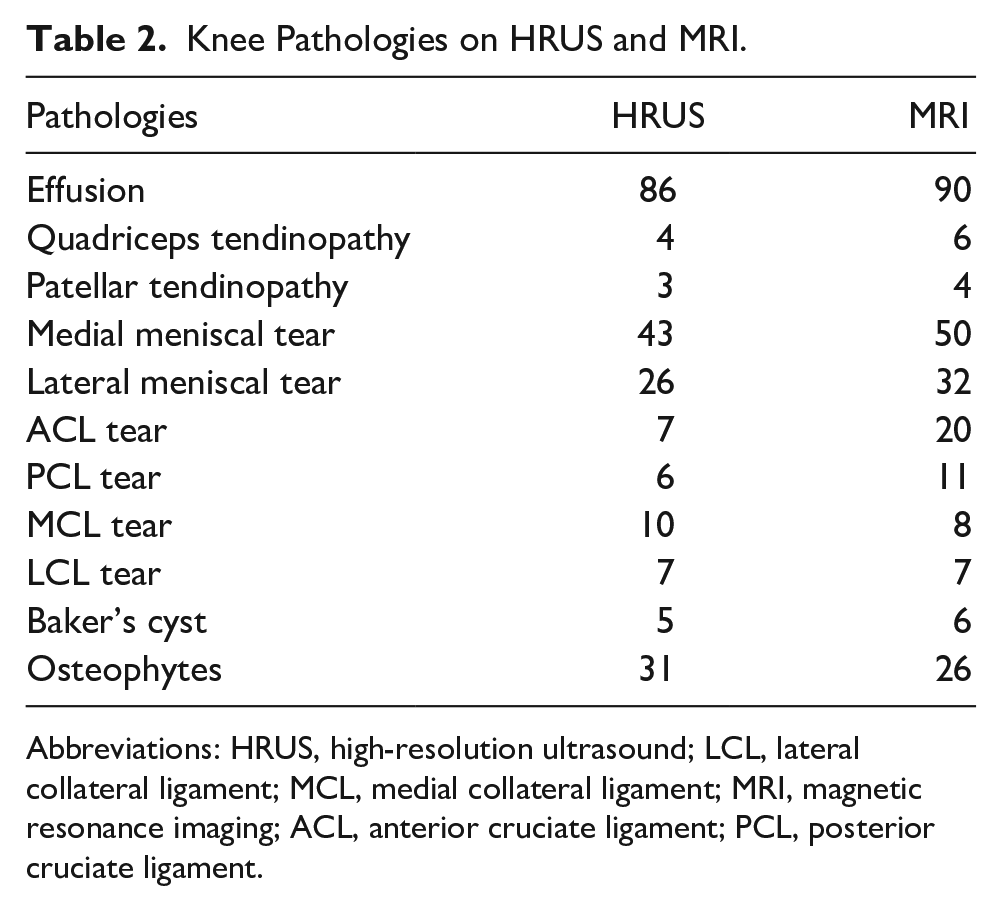
Abbreviations: HRUS, high-resolution ultrasound; LCL, lateral collateral ligament; MCL, medial collateral ligament; MRI, magnetic resonance imaging; ACL, anterior cruciate ligament; PCL, posterior cruciate ligament.
Sensitivity, specificity, accuracy, and agreement level of HRS in detecting the various knee joint pathologies with MRI as gold standard are shown in Table 3.
Diagnostic Accuracy and Agreement Level of HRUS Compared With MRI for Detecting Various Knee Joint Pathologies.
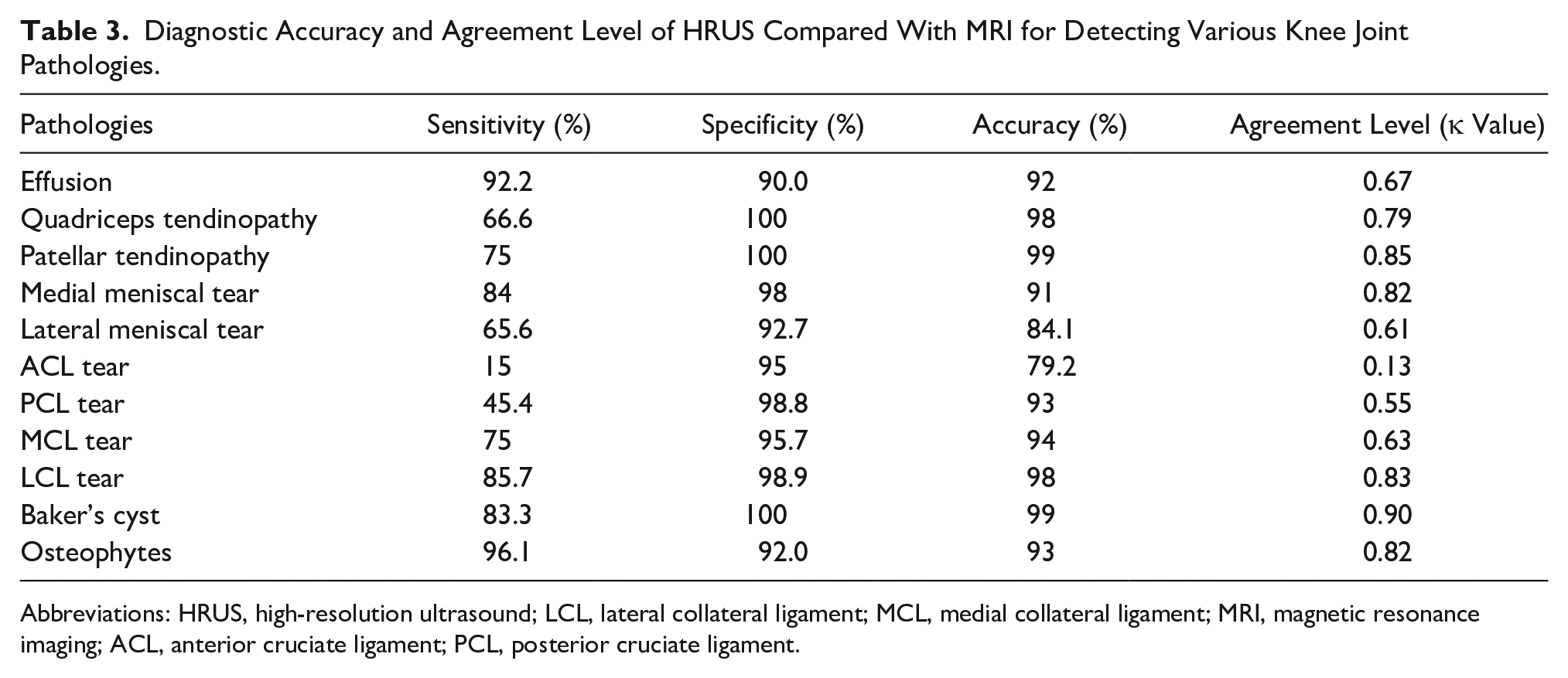
Abbreviations: HRUS, high-resolution ultrasound; LCL, lateral collateral ligament; MCL, medial collateral ligament; MRI, magnetic resonance imaging; ACL, anterior cruciate ligament; PCL, posterior cruciate ligament.
Among various pathologies, HRS demonstrated an accuracy of 99% for detecting Baker’s cyst and patellar tendinopathy, 98% for detecting quadriceps tendinopathy and LCL tear, and 94% and 93% for detecting MCL and PCL tear, respectively.
Almost perfect agreement was noted between HRS and MRI for detecting the medial meniscal tear, LCL tear, patellar tendinopathy, Baker’s cyst, and osteophyte.
Discussion
In recent years, musculoskeletal imaging has expanded rapidly due to imaging capabilities of MRI and HRS, to detect the musculoskeletal pathologies. Although the role of MRI has been undoubtedly established, HRS continues to be investigated for musculoskeletal imaging, as an effective accessory tool. Not much information is available on the effective utilization of musculoskeletal HRS, for evaluation of knee joint pathologies, in developing countries. Over the past few decades, literature has shown that HRS is quite sensitive and specific for assessing numerous pathologies of knee joint, such as the meniscal tears and ligament injuries.7,9
This study is unique since it has been conducted in a considerably basic setup, in a developing country, which has limited resources for a large population. The chances for bias are less since the observers were blinded to the findings of the other imaging modality.
In this study, the majority (n = 30) of the study population were in the age group 21 to 30 years of age and mean age was 32.9 years. There were 78 males and 25 females and male predominance, which was similar to studies conducted by Khan et al 15 and Singh et al. 16
In this study, 74 patients gave history of preceding trauma to the knee. The most common HRS findings in the study were knee joint effusion (n = 86) followed by medial meniscal tear (n = 43), osteophytes (n = 31), and lateral meniscal tear (n = 26).
Anterior tendons of knee, which include quadriceps and patellar tendons, are the most common tendons evaluated in knee trauma. Overuse of the anterior compartment tendons causes more stress and injury. Tendinopathy is one of the most common causes of acute knee joint pain. In this study, HRS had a sensitivity of 75% and 66.6% in detecting patellar and quadriceps tendinopathy in comparison to 84% and 87.5% reported by Basha et al. 17 In this cohort, there was almost perfect agreement with a coefficient κ = 0.85, which was noted between HRS and MRI, in detection of knee patellar tendinopathy. Likewise, there was substantial agreement with coefficient κ = 0.79, which was noted between HRS and MRI, in detection of knee quadriceps tendinopathy. All these comparisons were noted to be statistically significant (P < .001). This would indicate that HRS has the reliability needed, for the evaluation of patellar and quadriceps tendinopathy.
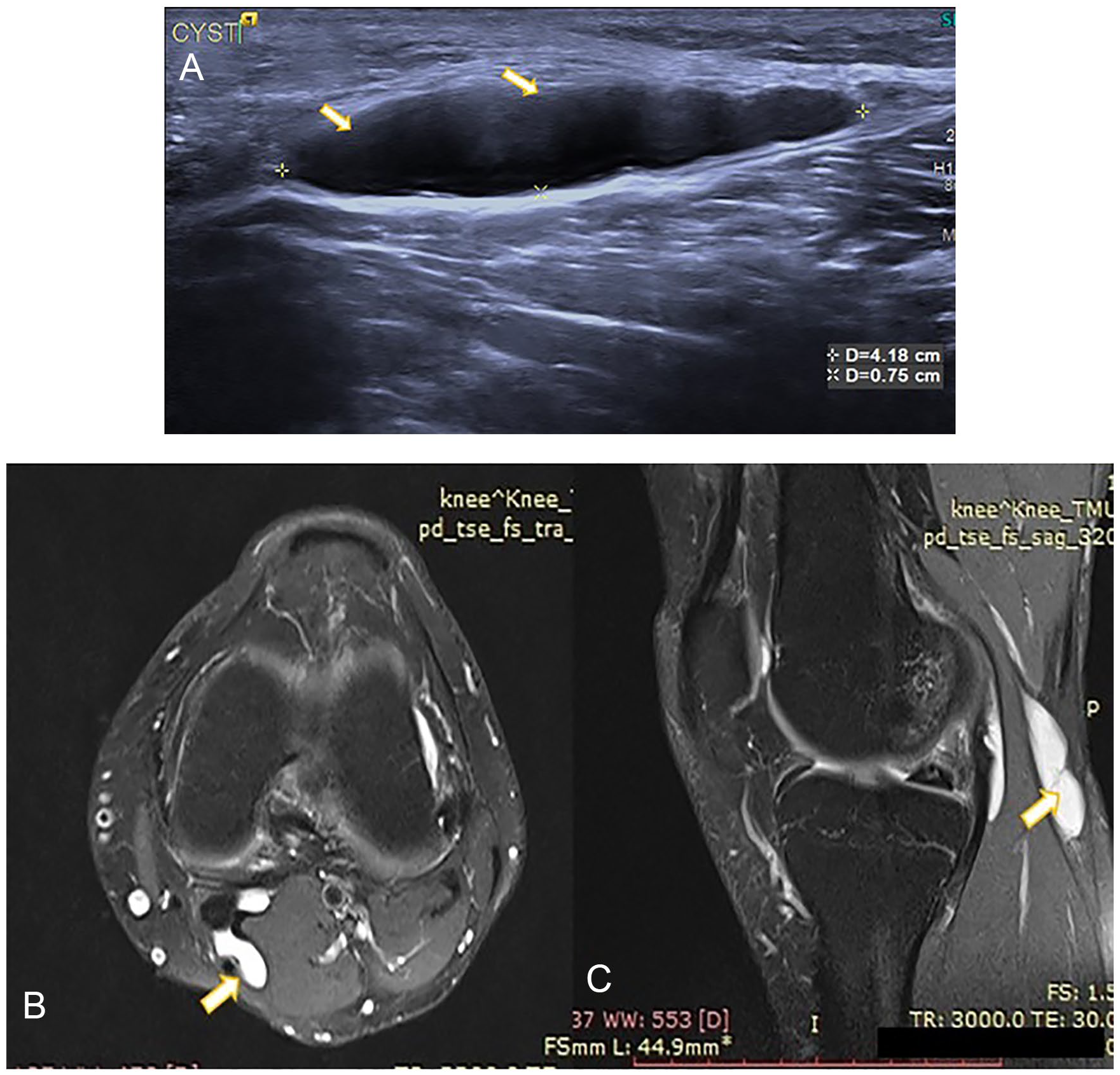
Knee joint effusion was one of the most common HRS findings in this study, and a substantial agreement was noted (κ = 0.67) between HRS and MRI, in detection of knee joint effusion. This comparison was also found to be statistically significant (P < .001). HRS demonstrated sensitivity, specificity, and accuracy of 92.2%, 90%, and 92%, respectively, in detection of knee joint effusion (Figure 1). The PPV was 98.8% and NPV was 58.2%. Wang et al evaluated the diagnostic accuracy of HRS in detecting knee effusion. They demonstrated that the sensitivity, specificity, PPV, and NPV of the sonographic examination, for detecting knee joint effusion, were 79.1%, 50%, 86.3%, and 37.5%, respectively. 18 Singh et al and Draghi et al also showed good sensitivity and specificity of HRS in detection of knee joint effusion, which compares nicely with this study. Singh et al showed the sensitivity, specificity, and accuracy of 100%, 100%, and 100%, respectively, in detection of knee joint effusion. Draghi et al also posted a sensitivity, specificity, PPV, and NPV of 81.3%, 100%, 100%, and 77.5%, respectively.19,20 All these findings reinstated the fact that HRS can dependably detect knee joint effusion. It can also further screen for added diagnostic findings in the knee joint which makes HRS an important first choice for the evaluation of the knee.
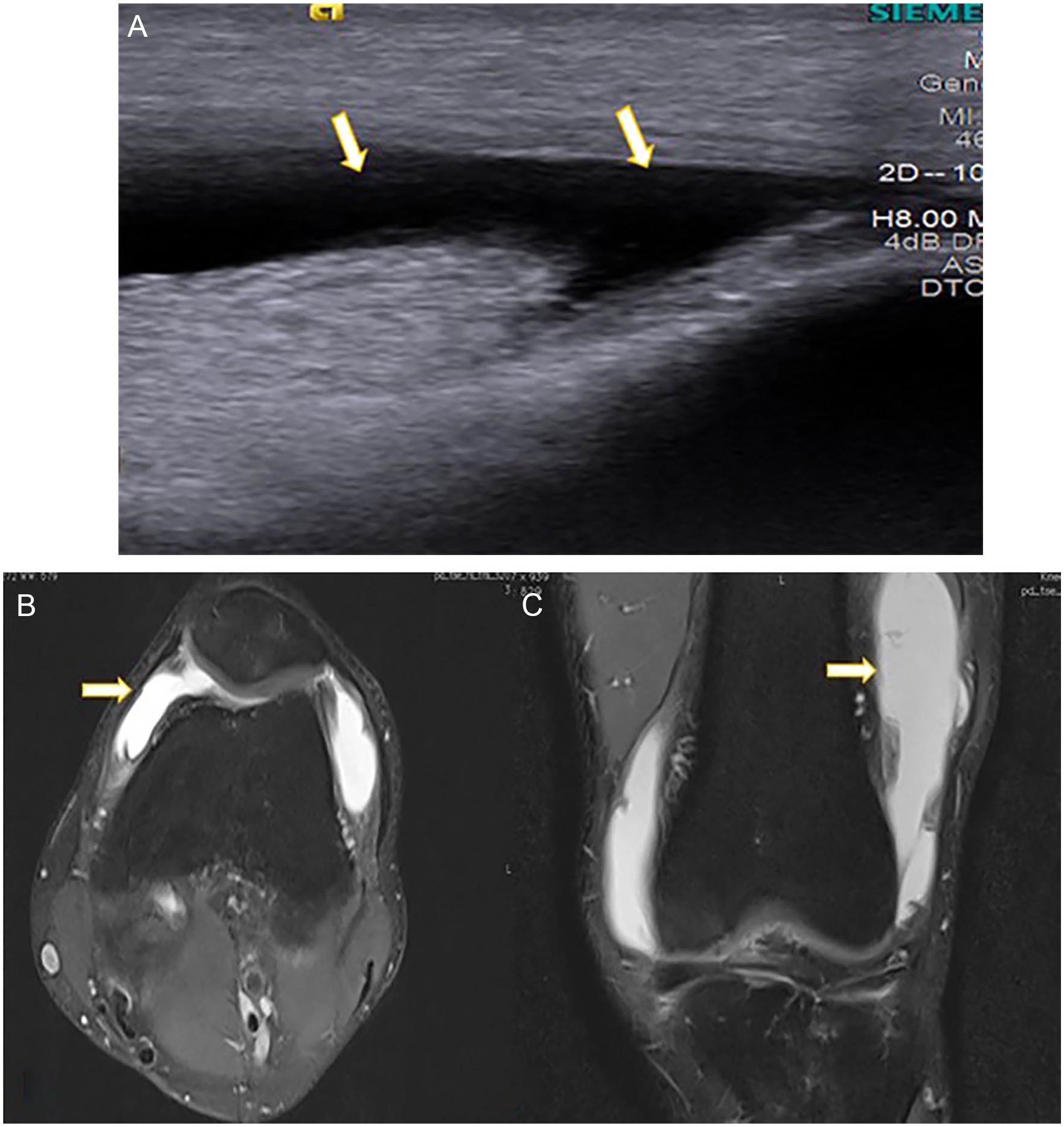
(A) Longitudinal high-resolution sonography image depicts hypoechoic collection within the joint space suggestive of effusion. (B, C) Magnetic resonance imaging Proton Density Fat Saturated (PDFS) axial and coronal images show hyperintense collection within the joint space suggestive of knee joint effusion.
Degeneration and tears constitute majority of meniscal lesions and are common cause of knee joint pain. In this study, almost perfect agreement (κ = 0.82) was seen between HRS and MRI, in detection of medial meniscal tear and substantial agreement (κ = 0.61) was seen between HRS and MRI in detection of lateral meniscal tear. For meniscal tear, in this study, HRS demonstrated specificity, sensitivity, and accuracy of 98.0%, 84.0%, and 91%, respectively, in detection of medial meniscal tear. It also demonstrated a specificity, sensitivity, and an accuracy of 92.7%, 65.6%, and 84.1%, respectively, in detection of lateral meniscal tear. In this study, a lateral meniscal tear was less common, compared with a medial meniscal tear. This is consistent with studies published by Artul et al and Singh et al. In those studies, they found that a lateral meniscal tear was less common than a medial meniscal tear.19,21 In the study done by Singh B et al and Singh A et al, they showed a sensitivity of 92% and 77.7%, specificity of 96% and 90.4%, and accuracy of 94% and 86.6% in diagnosing medial meniscal tears by HRS. They also showed sensitivity of 64.5% and 40.0%, specificity of 98.8% and 91.1%, and accuracy of 95% and 78.3% in diagnosing lateral meniscal tears. Findings in both these studies were similar to our studies.16,19 Sharma and Grewal concluded that sonography can also be an effective diagnostic imaging modality for evaluating patients with medial meniscal tears, compared with MRI. They demonstrated sensitivity, specificity, NPV, PPV, and accuracy of medial meniscal tear as 80.77%, 98.6%, 93.5%, 95.4%, and 94.0% and of lateral meniscal tear as 70.0%, 93.3%, 53.8%, 96.5%, and 91.0%, respectively (see Figures 2 and 3). However, the accuracy of diagnosing the lateral meniscal tear by sonography was low (53.8%) as compared with this study (84.1%). 22 In the study done by Park et al, 23 it was seen that the sensitivity was 86.2%, specificity was 84.9%, accuracy was 85.4%, PPV was 75.8%, and NPV was 91.8% in detection of meniscal tears. This work which was in agreement with this study revealed that HRS had good correlation with MRI and thus suggested the usefulness of the HRS, in evaluating meniscal injuries. However, in the study conducted by Shett et al, 24 it was reported that HRS had a high sensitivity of 86.4% and low specificity of 69.2% in detection of meniscal tear as compared with this study.
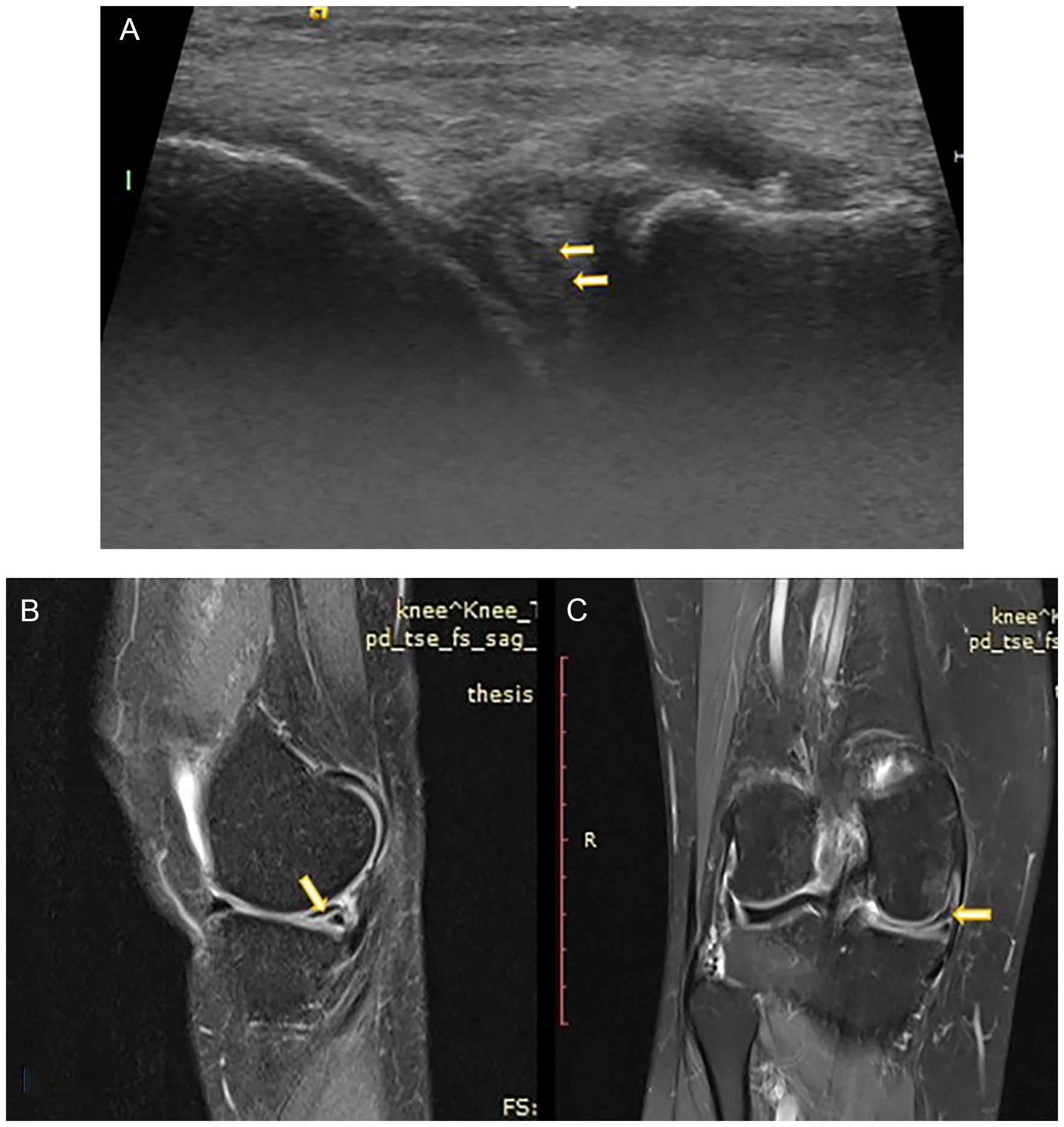
(A) Longitudinal high-resolution sonography image depicts linear hypoechoic area involving the medial meniscus suggestive of tear. (B, C) Magnetic resonance imaging Proton Density Fat Saturated (PDFS) sagittal and coronal images show linear hyperintense altered signal intensity area in the posterior horn of medial meniscus suggestive of tear.
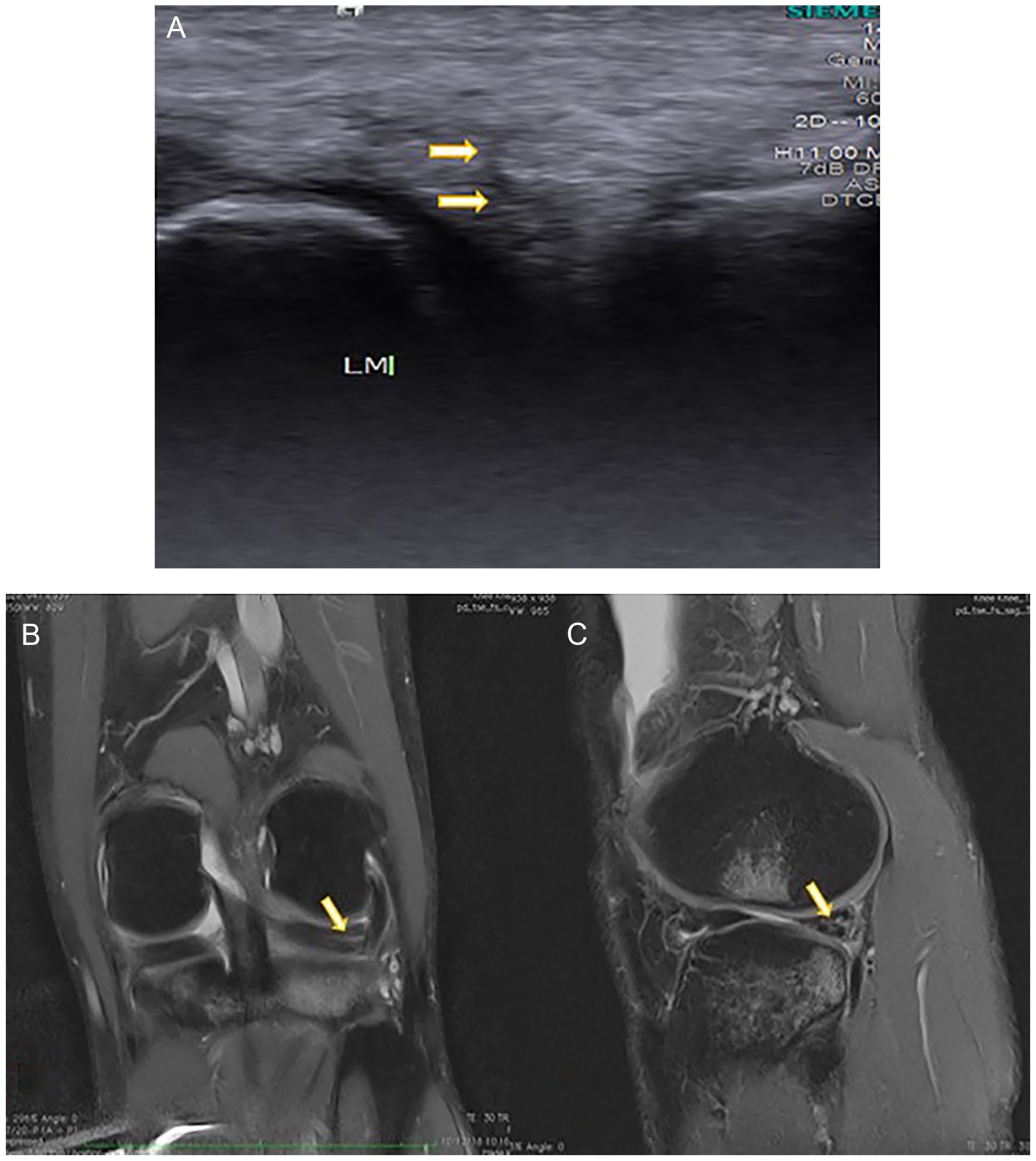
(A) Transverse high-resolution sonography image depicts linear irregular hypoechoic area involving the lateral meniscus suggestive of tear. (B, C) Magnetic resonance imaging Proton Density Fat Saturated (PDFS) sagittal and coronal images show linear hyperintense altered signal intensity area in the anterior and posterior horn of lateral meniscus suggestive of tear.
Collateral ligaments are commonly injured during sport and vigorous daily activities. Collateral ligaments can be easily visualized due to their superficial location. In this study, a total of ten MCL tears and seven LCL tears were detected with HRS and eight MCL tears and seven LCL tears were detected with MRI. Collateral ligament tears appear as a hypoechoic and thickened ligament on HRS. Singh A et al, Singh B et al, and Artul et al showed a high proportion of menisci and cruciate ligament tears, compared with the collateral ligaments. Artul et al reported on only one case of each MCL and LCL out of 276 patients.16,19,21 In this study, substantial agreement (κ = 0.63) was seen in detection of an MCL tear with a high sensitivity, specificity, and accuracy of 75.0%, 95.7%, and 94.0%, respectively. There was almost perfect agreement (κ = 0.83) seen in detection of LCL tear, with a high sensitivity, specificity, and accuracy of 85.7%, 98.9%, and 98.0%, respectively, between HRS and MRI (see Figures 4 and 5). However, due to the smaller number of cases of MCL/LCL tears in this cohort, the significance of these values was questionable. Compared with this study, Singh B et al and Singh A et al showed a higher sensitivity (83.3% and 84.6%) but similar specificity (97.7% and 100%) and accuracy (96% and 96.6%), in detection of MCL. Likewise, they demonstrated a similar sensitivity, specificity, and accuracy for LCL by high-resolution ultrasound (HRUS).19,16 Ghosh et al 25 showed a lower sensitivity (67%) and specificity (83%) for MCL tear in comparison to our study. Sekiya et al 26 revealed high sensitivity and low specificity of 92% and 75%, respectively, for diagnosis of the LCL injuries in comparison to this study.
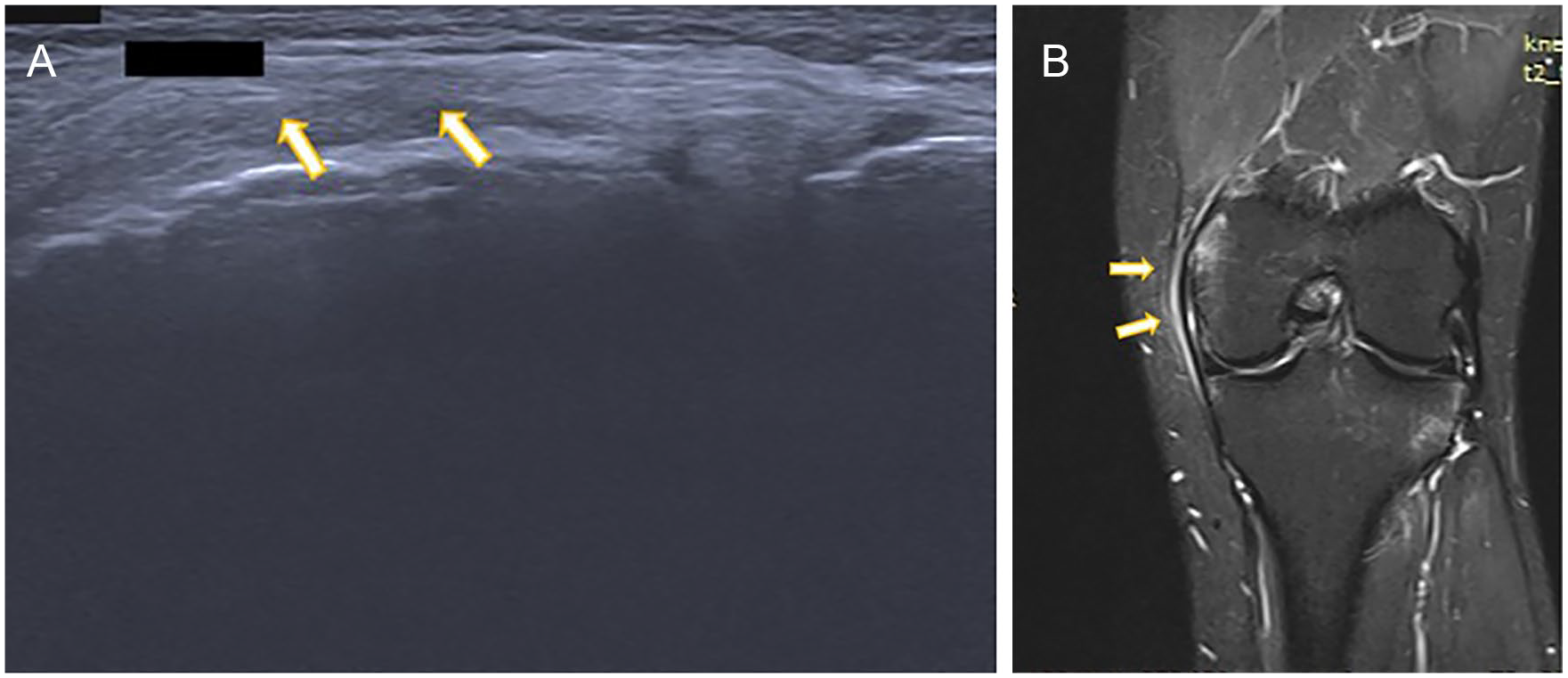
(A) Longitudinal high-resolution sonography image depicts heteroechoic and thickened medial collateral ligament suggestive of sprain/tear. (B) Magnetic resonance imaging T2IR coronal image shows hyperintensity and thickening of medial collateral ligament suggestive of sprain/tear.
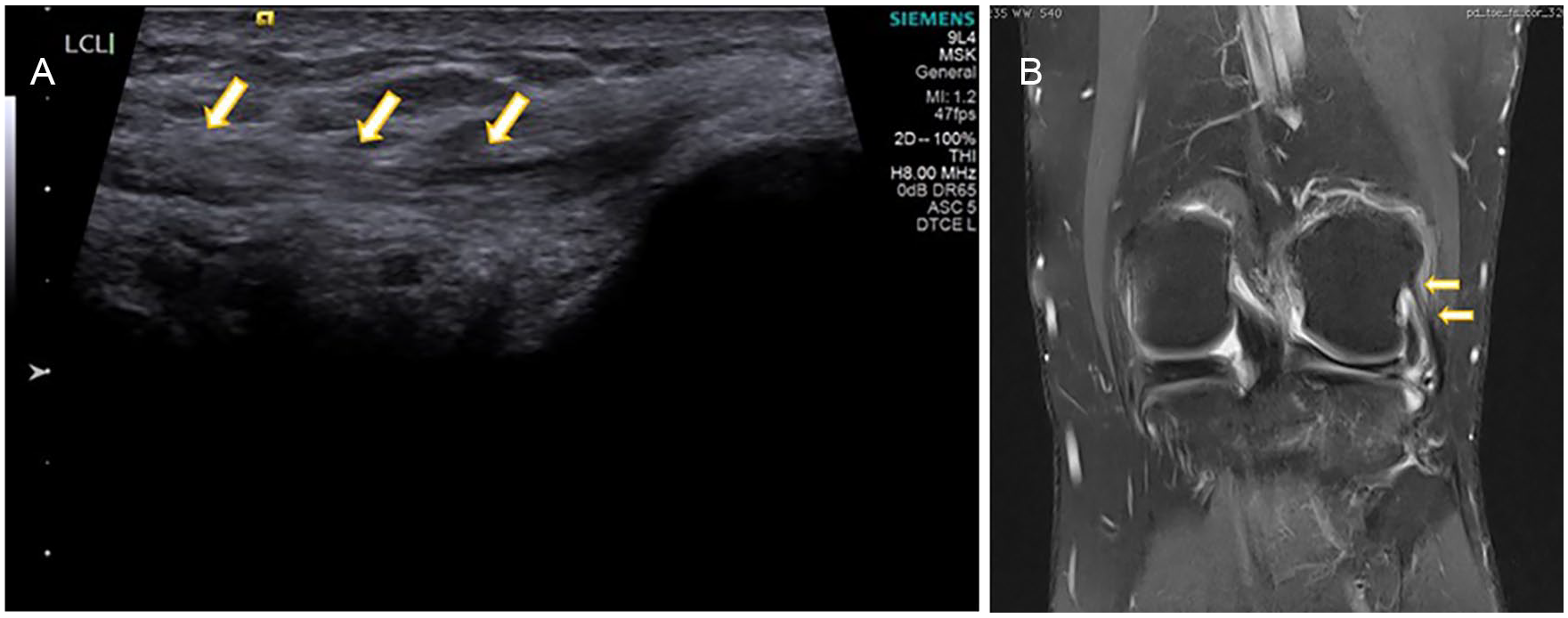
(A) Longitudinal high-resolution sonography image depicts heteroechoic lateral collateral ligament suggestive of tear. (B) Magnetic resonance imaging Proton Density Fat Saturated (PDFS) coronal image shows PDFS hyperintensity and thickening of lateral collateral ligament suggestive of sprain/tear.
Currently, MRI is considered the gold standard in diagnosing cruciate ligament injuries. Various methods have been described in literature to visualize the ACL and PCL by HRUS. In our study, ACLs were only partially visualized due to its deep and oblique orientation precluding its direct visualization. In our study, a total of 7 ACL tears and 6 PCL tears were detected on HRUS and 20 ACL tears and 11 PCL tears were detected on MRI. Slight agreement (κ = 0.13) was seen with an extremely low sensitivity of 15% but high specificity and accuracy of 95% and 79.2%, respectively, in detection of ACL tear, and substantial agreement (κ = 0.55) was seen with a low sensitivity of 45.4% but high specificity and accuracy of 98.8% and 93%, respectively, in detection of PCL tear between HRUS and MRI. Again, due to the smaller number of these findings, the statistical significance was unreliable. However, further studies concentrating only on cruciate ligament tears would be the way forward.
Compared with the cohort study, Khan et al, Singh A et al, and Singh B et al all showed high sensitivity, that is, 78.2%, 82.3%, and 75%, respectively, for diagnosing an ACL tear. These were much higher rates of diagnosis than this study. However, the specificity and accuracy of HRS in diagnosing ACL tear in this cohort was similar to their studies (i.e., 78.3%, 90.0%, and 86.6%, respectively).15,16,19 Grzelak et al 27 revealed a higher sensitivity (91.9%) for HRS, in the detection of ACL tears which was higher than that found in this cohort. However, specificity (95.6%) in detection of ACL tear was similar to that in this group. The proximal part of PCL cannot be detected by HRS; however, the middle and distal most part of PCL can be detected, using a posterior sonographic approach. In this study, HRS showed a lower sensitivity (45.4%) which is consistent with the study done by Singh A et al, who posted a sensitivity of 33.3% in detection of PCL tear. Studies completed by Lalitha et al 28 and Wang et al 18 showed higher sensitivity of 83.3% and 83.3%, respectively, in comparison to the other study. However, HRS showed high specificity of 98.8% which is consistent with other studies done by Singh et al, 19 Singh et al, 16 and Lalitha et al. 28 El-monem et al 29 showed high accuracy, sensitivity, and specificity of HRS in diagnosis of ACL as 83.3%, 81.2%, and 84.2%, respectively, and for PCL as 90%, 50%, and 96%, respectively, as compared with this study.
Due to the deep-seated location of these ligaments, sonography equipment systems, with higher resolution and more operator experience, would be indispensable for their evaluation of the knee with HRS.
Baker’s cysts appear as a hypoechoic/anechoic loculated collection of fluid between the medial head of gastrocnemius and semimembranosus in popliteal fossa. In our study, HRS showed a sensitivity, specificity, and accuracy of 83.3%, 100%, and 99.0%, respectively (see Figure 6), which is consistent with the findings of Singh et al 19 and Ward et al. 30 Makarova et al 31 revealed high accuracy of HRS in diagnosing Baker’s cyst, which was consistent with this study findings.
(A) Longitudinal high-resolution sonography image depicts linear hypoechoic area in posterior aspect of knee suggestive of Baker’s cyst. (B, C) Magnetic resonance imaging Proton Density Fat Saturated (PDFS) axial and sagittal images show hyperintense altered signal intensity area in posterior aspect of knee between the medial head of gastrocnemius tendon and semimembranosus tendon suggestive of Baker’s cyst.
Thus, the role of HRS for detection of Baker’s cyst was again reestablished by the results of this cohort of patients.
For the detection of osteophytes, HRS showed an accuracy, specificity, and sensitivity of 93.0%, 92.0%, and 96.1%, respectively. Almost perfect agreement (κ = 0.82) was seen between HRS and MRI in detection of osteophytes. For detecting the osteophytes, Sharma and Grewal 22 showed high sensitivity of 100%, specificity of 97.2%, and accuracy of 98% which is consistent with this study’s findings. Podlipska et al demonstrated a high accuracy and almost perfect agreement in detection of osteophytes. They showed sensitivity, specificity, and accuracy of 98.1%, 87%, and 91.2%, respectively, for femoral osteophytes. 32
With the ever-increasing prevalence of obesity which leads to osteoarthritis, HRS might become an important nonionizing diagnostic tool for the detection of this disease.
Study Limitations
This study’s limitations were the small sample of patients evaluated. The results cannot be generalized due to the threats to internal and external validity, inherent to the study design. Given this was a convenient sample of patients, it would be recommended that a larger study be done to randomly recruit patients and ideally from multiple centers.
Conclusion
HRS shows good accuracy and sensitivity in diagnosis of a meniscal tear, knee joint effusion, and tendinopathy. However, in this study, HRS demonstrated low sensitivity but good specificity and accuracy in diagnosing a lateral meniscal tear. Both ACL and PCL are partially visualized due to deep and oblique location; therefore, HRS is not recommended as a primary imaging modality, for the evaluation of cruciate ligament tears. However, it can be used as a screening tool and as an alternative modality of choice, when MRI is not available or contraindicated. HRS is a good choice as a diagnostic imaging technique and shows good sensitivity, specificity, and accuracy in detection of knee joint effusion and Baker’s cyst. HRS could also be used for evaluation of collateral ligaments and other knee joint pathologies, like osteophytes.
This study adds to the growing evidence that HRS could be used as a primary screening tool or diagnostic imaging modality, for the assessment of knee joint pathologies. An expensive and time-consuming investigation like MRI can then be reserved for those cases where HRS is equivocal and when a detailed evaluation of deep structures is required, for certain knee joint pathologies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.