
Abstract
This case report details the management of a patient with cirrhosis who developed chylous pleural and peritoneal effusions. The patient, with a 28-year history of untreated hepatitis B, presented with dyspnea and cough after traveling to a high-altitude area. Imaging and laboratory tests confirmed the presence of chylous effusions. Treatment included thoracentesis, paracentesis, antibiotics, somatostatin analogs, and supportive care. The patient showed significant improvement and was discharged with no recurrence at follow-up. This case highlights the importance of early diagnosis and conservative management of chylous effusions in cirrhosis, emphasizing the potential role of somatostatin analogs in reducing effusion formation and promoting lymphatic healing.
Introduction
Chylous ascites is a rare form of ascites, usually caused by the rupture of lymphatic vessels due to trauma or increased pressure in the abdominal lymphatic vessels due to obstruction, leading to the leakage of lipid-rich lymph into the peritoneal cavity. The underlying causes of chylous ascites can have traumatic, congenital, infectious, neoplastic, postoperative, cirrhotic, or cardiac origins. The occurrence of nontraumatic chylous ascites in cirrhosis is rare, accounting for only 0.5%–1.0% of ascites cases, and some may be associated with chylous pleural effusion. The mortality rate can reach 40%–70% or even higher. 1 Chylous pleural effusion accounts for approximately 3% of all pleural effusion cases. 2 Chylous pleural effusion in cirrhosis is caused by obstruction or injury to the thoracic duct or its tributaries or by the leakage of chyle into the pleural cavity through the diaphragmatic blood flow from the peritoneal cavity. Chylothorax is a pleural effusion that appears milky because it is rich in chylomicrons and triglycerides. A triglyceride level >110 mg/dL supports the diagnosis; however, if the fluid appears serous or bloody, protein electrophoresis can confirm the presence of chylomicrons. Most chylothoraces are exudative as per Light’s criteria and arise from thoracic duct injury—often after cardiothoracic surgery—or from lymphatic obstruction by tumors or mediastinal lymphadenopathy, both of which allow chyle to leak into the pleural space. 3 The 90-day mortality rate for chylous pleura can be as high as 82%. Currently, both domestic and international literature consists mostly of case reports, and there are no guidelines or consensus on its pathogenesis, nature of the effusion, diagnostic methods, and treatment plans. 4 The pathogenesis of chylous ascites in cirrhosis is due to impaired hepatic venous return, increased sinusoidal pressure, excessive production of hepatic lymph beyond the drainage capacity of the thoracic duct, lymph leakage, and obstruction of thoracic duct lymphatic returns due to compression by cirrhotic nodules, leading to lymphatic dilation and rupture. The pathogenesis of secondary chylous pleural effusion is similar to that of chylous ascites in cirrhosis. In this pathogenesis, the negative pressure in the pleural cavity causes chylous ascites to pass through small channels in the diaphragm into the pleural cavity, where it accumulates to form chylous pleura. Alternatively, portal hypertension leads to lymphatic dilation, lymphatic return impairment, and rupture or exudation of small lymphatic vessels or the thoracic duct, resulting in chylous pleura. 5
Case report
A male patient in his late 40s was admitted to Mianyang Central Hospital, Sichuan, China. He had been infected with hepatitis B virus (HBV) for 28 years without treatment. Eighteen months ago, he presented with abdominal distention secondary to decompensated cirrhosis caused by hepatitis B infection and was diagnosed with chylous ascites. Since then, he had been regularly treated with antiviral therapy, avoiding hepatotoxic medications, human serum albumin supplementation, and diuretics. Three days before admission, the patient, who had traveled to a plateau area (elevation 2600 m), suddenly experienced dyspnea, accompanied with coughing, mainly dry cough. Physical examination revealed pale conjunctiva, lips, and nail beds of the limbs, without scleral icterus. The respiratory rate was 23 per min. Coarse breath sounds were heard in the upper lungs bilaterally, occasionally with fine crackles. The breath sounds were coarse in the left lower lung and absent in the right lower lung, and dullness was noted on percussion of the right lower lung. The heart rate was 82 beats per min, with no pathological murmurs heard in any valve auscultation areas. The abdomen was distended, without periumbilical varices. There was no tenderness, rebound tenderness, or muscle rigidity in the abdomen. The liver was not palpable below the costal margin, but an enlarged spleen was palpable. There was no tenderness in the liver and kidney areas. Positive shifting dullness was noted, and bowel sounds were normal. There was no edema in the lower limbs.
Noncontrast computed tomography (CT) of the chest, abdomen, and pelvis revealed right pneumonia, increased and blurred lung markings on the left side, a large amount of loculated pleural effusion on the right side, significant atelectasis and compression of the right lung, cirrhosis of the liver, a slightly hypo-dense nodule in the right lobe of the liver (nature to be determined), portal hypertension with collateral circulation, a significantly enlarged spleen, marked edema and roughness of some intestinal walls, swelling and blurring of some mesentery and omentum, unclear fat planes in the abdominal and pelvic cavities, and effusions in the abdominal and pelvic cavities (Figure 1(a) and (b)).

(a) Large amount of pleural effusion shown on chest computed tomography (CT) and (b) small amount of effusion shown on follow-up enhanced CT after drainage of 2100 mL of pleural effusion.
Blood tests showed the following results: total protein level, 54.40 g/L; albumin level, 31.66 g/L; sodium level, 126.41 mmol/L; lymphocyte count, 0.31 × 109/L; monocyte percentage, 86.30%; lymphocyte percentage, 5.50%; red blood cell count, 3.27 × 1012/L; hemoglobin level, 77.00 g/L; hematocrit, 25.60%; mean corpuscular volume, 78.40 fL; mean corpuscular hemoglobin, 23.60 pg; and mean corpuscular hemoglobin level, 301.00 g/L. Peripheral smear showed a reduced number of red blood cells, which varied in size, with enlarged central pallor. Further laboratory test results were as follows: folate level, 1.650 μg/L; serum ferritin level, 14.70 μg/L; carbohydrate antigen CA72-4 level, 11.05 U/mL; cytokeratin 19 fragment level, 5.44 ng/mL; D-dimer level, 1.37 μg/mL; prothrombin time, 15.40 s; prothrombin activity, 67.48; and international normalized ratio, 1.26. The fecal occult blood test was positive. The level of hepatitis B surface antigen (as determined via chemiluminescent immunoassay) was >250.0000 IU/mL, level of hepatitis B core antibody was >10.000 IU/mL, and the hepatitis B pre-S1 region signal-to-cutoff ratio was 28.43. High-precision HBV viral load testing was negative. Renal function, lipid profile, fasting blood glucose, tumor markers (lung), tumor markers (gastrointestinal tract), alpha-fetoprotein, carcinoembryonic antigen, N-terminal brain natriuretic peptide, and procalcitonin were all within normal limits.
The pleural effusion appeared milky white, with a positive chylous test. Examination revealed chylous-like turbidity, positive mucin qualitative test (Rivalta test), cell count of 1080.00 × 106/L, nucleated cell count of 80.00 × 106/L, mononuclear cell percentage of 81.40%, polymorphonuclear cell percentage of 18.60%, glucose level of 6.61 mmol/L, total protein level of 9.0 g/L, lactate dehydrogenase level of 53.00 U/L, and adenosine deaminase level of 2.00 U/L. The ascites appeared milky white, with a positive chylous test. Examination revealed slight chylous-like turbidity, positive mucin qualitative test (Rivalta test), cell count of 2059.00 × 106/L, nucleated cell count of 59.00 × 106/L, mononuclear cell percentage of 89.70%, polymorphonuclear cell percentage of 10.30%, glucose level of 7.01 mmol/L, total protein level of 5.04 g/L, lactate dehydrogenase level of 42.00 U/L, and adenosine deaminase level of 1.67 U/L. The level of pleural fluid triglycerides was >121 mg/dL
Treatment included thoracentesis and paracentesis with catheter placement, ceftriaxone, human serum albumin combined with a somatostatin analog (octreotide), furosemide, spironolactone, omeprazole, sucrose iron, and folate. Pleural effusion was drained for 3 consecutive days (700, 800, and 600 mL, respectively), and ascites was drained for 1 day (700 mL) (Figure 2(a) and (b)). The drained effusions were initially milky white, which turned to an egg white color on the second day and light yellow on the third day. On day 4, follow-up abdominal ultrasound and contrast-enhanced chest CT showed multiple anechoic areas in the abdominal cavity, with the deepest area being approximately 5.0 cm, a small amount of pleural effusion, and infiltrate noted in the right lung lobe and left upper lung lobe (Figure 3(a) to (c) and Figure 4(a) and (b)). Increased and blurred lung markings were noted, with cirrhosis of the liver, a slightly hypo-dense nodule in the right lobe of the liver, portal hypertension, collateral circulation established, enlarged splenic vein, varices in the lower esophagus-cardia region, splenomegaly, and thickened, rough gallbladder wall (Figure 5(a) to (c)). The patient had a daily urine output of >2000 mL. After 7 days of treatment, the patient had no dyspnea, exhibited only occasional dry cough at night, without hemoptysis or melena, and requested discharge. The patient was in good condition at discharge. Follow-up at 1 and 2 weeks after discharge showed no recurrence or worsening of symptoms. The reporting of this study conforms to Case Report (CARE) guidelines. 6
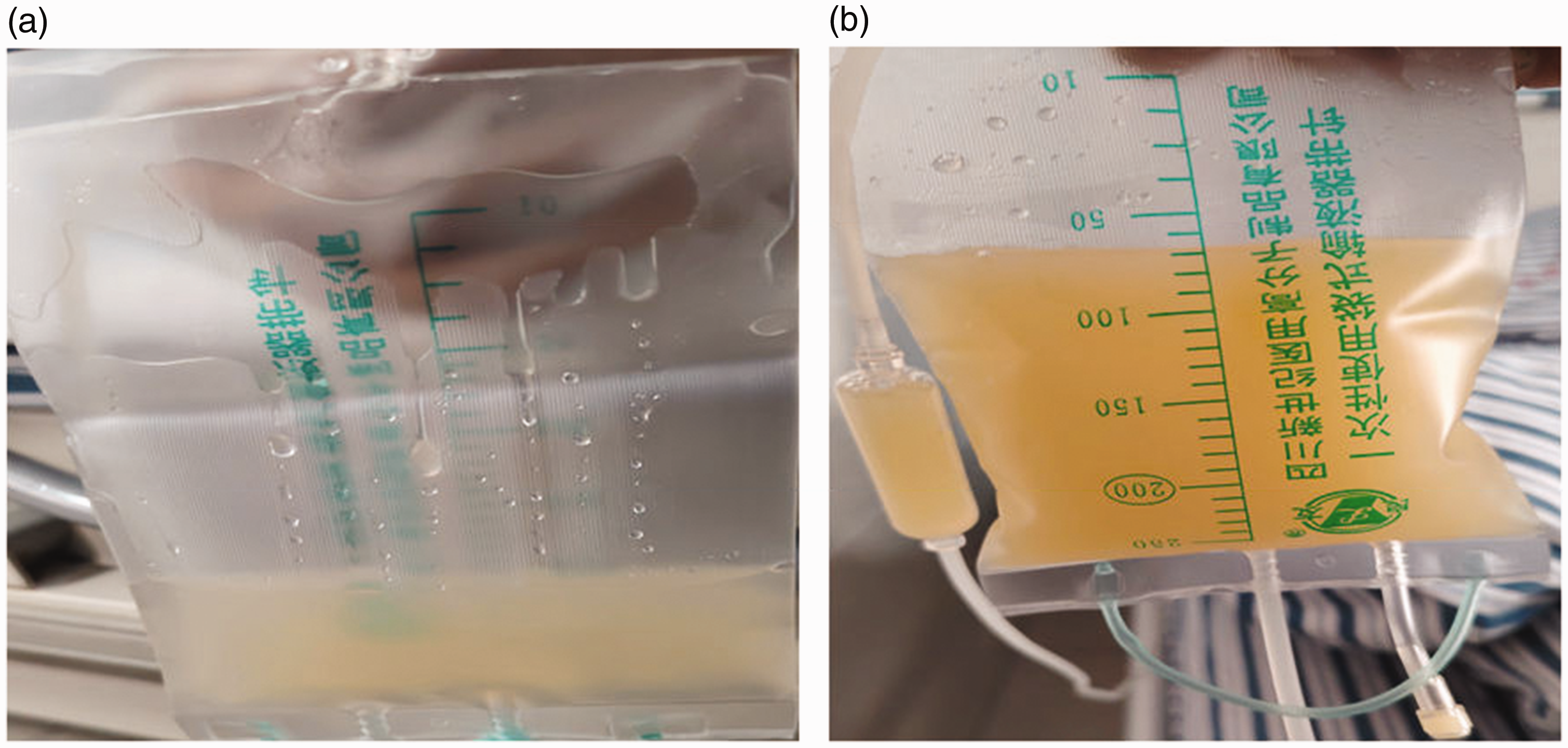
Drainage of effusion. (a) Ascites and (b) pleural effusion (on the second day of drainage).

The shape of the liver and spleen as well as the ascites in the abdominal and pelvic cavities shown on abdominal computed tomography.

Enhanced computed tomography of the liver, spleen, and abdominal cavity.

(a) Dilated portal vein shown on color Doppler ultrasound; (b) Liver and (c) Spleen.
Discussion
Due to the anatomical course of the thoracic duct in the human body, rupture of the thoracic duct below the fifth thoracic vertebra can result in isolated right-sided chylous pleura, while rupture above the fifth thoracic vertebra can lead to bilateral chylous pleura. 4 The characteristics of chylous pleural and peritoneal effusions are as follows: 1. Chylous effusions can be milky white or serosanguineous, with a positive chylous test, and fat globules can be seen on microscopic examination of the pleural and peritoneal effusions. In this case, the triglyceride level was >121 mg/dL, protein levels ranged from 6 to 38 g/L, specific gravity was approximately 1.020, cell count was >500 × 106/L, with lymphocytes being predominant, and the Rivalta test was positive. First described in 1895 by the Italian physician Fabio Rivalta, the Rivalta test is a simple, inexpensive way to distinguish inflammatory exudates from noninflammatory transudates in serous effusions. Although it can be applied to any body cavity fluid, it is most commonly used for ascitic fluid. By detecting the relative abundance of protein, the test provides early evidence regarding the presence of an infection. Cultures of the ascites are usually negative. 2. Chest radiography rarely indicates the cause of chylothorax; it is helpful mainly when blunt or penetrating trauma is suspected.
Multidetector CT scans of the chest, abdomen, and pelvis are more informative, revealing the sites of lymphatic disruption, bulky or compressive lymphadenopathy, malignant masses, or associated ascites that may explain the chyle leak. When detailed mapping of the lymphatic system is required, the choices are lymphangiography, lymphoscintigraphy, and magnetic resonance (MR) lymphangiography. Selection is tailored to individual patients. Traditional lymphangiography—performed by injecting an oil-based contrast agent such as Lipiodol into a pedal lymphatic vessel and tracking its passage fluoroscopically to the thoracic duct—remains the gold standard. After opacification, the duct is further assessed via plain films or CT. In a retrospective case series, Alejandre-Lafont et al. 7 identified the site of leakage in 79% of patients with chylothorax, chylous ascites, lymphocele, or lymphatic fistula who underwent lymphangiography. The same procedure achieved occlusion of the leak in 70% of patients with drainage ≤500 mL/day, yielding an overall success rate of 51% independent of the mechanism of duct injury or the interval between injury and intervention. 5 The treatment of cirrhotic chylous pleural and peritoneal effusions includes conservative therapy and surgical therapy. Conservative therapy involves treating the underlying disease; adopting a low-sodium, low-fat, high-protein diet rich in medium-chain triglycerides; and, if necessary, administering total parenteral nutrition (TPN). TPN can reduce the production of lymph and, consequently, the formation of chylous pleural and peritoneal effusions while providing the body with essential nutrients. Other conservative measures include thoracentesis and paracentesis with albumin infusion, infection prevention, diuretic use, somatostatin application, and pleural and peritoneal drainage. 8
If there is no significant improvement after 4–6 weeks of conservative treatment or if the daily drainage volume remains >500 mL despite some improvement, surgical intervention may be considered. 8 Preoperative procedures such as direct lymphangiography, CT lymphangiography, radionuclide lymphoscintigraphy, or MR lymphangiography can help locate the lymphatic fistula. During surgery, precise localization can be achieved using nanocarbon tracers. Thoracic duct embolization is currently the first-line, minimally invasive treatment for high-output chylothorax because it reliably stops chyle leakage with less morbidity than prolonged conservative therapy or open surgery. When embolization is not feasible, surgical ligation is the next step. Virtually, all procedures are performed through a right-sided, minimally invasive approach—video-assisted thoracoscopic surgery or robotic-assisted thoracic surgery. These techniques provide excellent visualization and are associated with low morbidity; thoracotomy is reserved for rare cases that cannot be managed thoracoscopically. The side of exploration is dictated by the duct’s anatomy and the location of the injury. In postoperative chylothorax, this site is usually known; in noniatrogenic cases, this site is mapped preoperatively using a pedal lymphangiogram. When bilateral chylous effusions are present, exploration begins on the right side. 9
Laparoscopic or open abdominal exploration can be performed to identify and ligate the leak site for repair. Other surgical options include transjugular intrahepatic portosystemic shunt (TIPS) or reversed saphenous vein shunts to reduce portal hypertension. 10 TIPS creates a low-resistance channel between an intrahepatic branch of the portal vein and a hepatic vein by deploying a metal stent. By converting portal blood flow into systemic flow, TIPS directly reverses the hemodynamic derangements that drive ascites in cirrhosis rather than merely offering symptomatic relief, as observed in paracentesis. Effective shunting lowers portal pressure, restores effective arterial blood volume, and augments visceral-to-systemic perfusion, thereby improving cardiac output and renal function. If all treatments fail, liver transplantation can be considered as the only effective option for patients with end-stage cirrhosis and its multiple complications. However, due to the shortage of donor organs and high costs, liver transplantation is not widely available in clinical practice.
In this case, the patient’s chylous pleural and peritoneal effusions were primarily attributed to cirrhosis; however, the potential association with the low-pressure, hypoxic high-altitude environment warrants further investigation. Although liver-transplant recipients often tolerate brief high-altitude exposure without incident, the safety of living permanently at elevation with chronic liver disease remains unknown. Anyone with cirrhosis should undergo a thorough pre-travel assessment to uncover factors that could worsen at altitude and devise strategies that lower these risks. Travelers must also receive clear guidance on recognizing, preventing, and treating acute mountain sickness, and they may need altitude-illness medications or dosages that differ from those recommended for healthy individuals. 11 Upon admission, the patient was treated with continuous oxygen therapy; a low-sodium, low-fat, high-protein diet; thoracentesis and paracentesis with catheter placement for drainage; ceftriaxone for infection control; human serum albumin supplementation; a somatostatin analog (octreotide) to reduce lymph production and promote lymphatic fistula healing; intravenous furosemide plus oral spironolactone for diuresis; and omeprazole for acid suppression. On the second day after initiating octreotide treatment, the patient’s ascites ceased to drain, and the pleural effusion significantly decreased, with the color of the drained fluid changing from milky white to egg white and then to light yellow the following day, and the volume of effusion also decreased, demonstrating a remarkable therapeutic effect. Somatostatin primarily acts on the widely distributed somatostatin receptors in gastrointestinal blood vessels and lymphatic vessels, reducing portal venous pressure and lymph production to decrease the formation of pleural and peritoneal effusions and promote the healing of lymphatic fistulas. 12
Conclusion
Patients with cirrhotic pleural and peritoneal effusions should be vigilant regarding the occurrence of chylous pleural and peritoneal effusions, and routine chylous tests should be performed. Early conservative treatment primarily based on the combination of human serum albumin and somatostatin analogs is effective in clinical practice. Moreover, studies have demonstrated that rational human serum albumin therapy, which raises the patient’s serum albumin levels, may facilitate the occurrence of recompensation and achieve “reversal” of cirrhosis. However, given the high mortality rate associated with this disease, it is crucial to enhance follow-up and patient education. Patients should be advised to seek medical attention promptly if there are any changes in their condition.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251371631 - Supplemental material for Management of chylous pleural and peritoneal effusions in a cirrhotic patient: A case report and review of literature
Supplemental material, sj-pdf-1-imr-10.1177_03000605251371631 for Management of chylous pleural and peritoneal effusions in a cirrhotic patient: A case report and review of literature by Xuegui Ju and Yaguang Li in Journal of International Medical Research
Footnotes
Acknowledgments
All authors contributed equally to this manuscript and are considered as first co-authors.
Author contributions
XJ: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing–original draft, Writing–review & editing.
YL: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Resources, Validation, Visualization, Writing–original draft, Writing–review & editing.
Availability of data and materials
Not applicable; please contact the author for data requests.
Consent for publication
Not applicable.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
Case reports do not need to be approved by the review board of the Chengdu Medical College Clinical Research Ethics Committee. Written informed consent was obtained from the patient for the publication of this case report.
Funding
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.