
Abstract
Glomus tumors are rare benign soft tissue tumors that arise from the glomus body. They typically develop in the subungual region but may develop extradigitally anywhere, in the upper or lower limbs. Extradigital glomus tumors can be misdiagnosed for years because of their atypical position and presentation. Being aware of an extradigital glomus tumor is important because they can be encountered during imaging studies and may be the cause of the patient’s symptoms. This report presents a case of an extradigital glomus tumor, of the forearm, diagnosed during neuromuscular sonography, in a patient with chronic intractable neuropathic-like pain, along the medial side of the left forearm. Sonographic imaging of the nerves, muscles, and tendons did not reveal any abnormalities. However, meticulous imaging of all tissue layers detected a subcutaneous vascular nodule. Subsequent excision biopsy and histopathologic assessment revealed a glomus tumor. After surgery, the patient experienced dramatic relief of pain. This case report highlights the importance of careful sonographic examination of all the tissues, including skin and subcutaneous tissue layers, to avoid missing non-neuromuscular pathologies that impact patient’s management.
Keywords
Glomus tumors are rare benign soft tissue neoplasms that account for less than 2% of soft tissue tumors. They develop from the glomus body, a cutaneous structure that has a thermoregulatory function. 1 Most glomus tumors develop in the subungual region of the digits. However, extradigital tumors can be encountered. 2 The clinical diagnostic hallmark is a triad of focal pain, localized tenderness, and cold intolerance, but misdiagnosis and delayed diagnosis are common, when patients present with atypical symptoms.3,4 In such atypical cases, diagnostic imaging is usually recommended. Both magnetic resonance imaging (MRI) and diagnostic medical sonography can be helpful in making the diagnosis. MRI can confirm the diagnosis and localize the lesion, but it may not be highly sensitive for the detection of small tumors and may require the use of intravenous contrast agent. 5 Sonography can identify glomus tumors, even those that are small and can accurately determine their sizes and locations. 6 In contrast to MRI, sonography does not need intravenous administration of contrast agent 5 and has the advantage of being a readily available, affordable, bedside diagnostic tool, with added dynamic ability. Therefore, sonography is well suited for the diagnosis and preoperative assessment of glomus tumor.
This report presents a case of an extradigital glomus tumor of the forearm diagnosed via high-resolution sonography in a patient with chronic intractable forearm neuropathic-like pain. The patient was primarily referred for neuromuscular sonography of the ulnar nerve. An informed consent was obtained from the patient and his privacy rights were preserved. The case report is in compliance with the Declaration of Helsinki.
Case Report
A 64-year-old man consulted a pain specialist because of chronic intractable left forearm pain. The condition started 9 years ago with severe pain along the distal aspect of the left forearm and hand. The pain was burning and electric in character, which radiated along the entire upper limb. The pain was provoked by minimal skin touch, exaggerated during cold weather, and limited the patient’s daily activities. The patient’s medical and family history were irrelevant to his clinical presentation. The patient sought medical advice several times over the years and received analgesics, antiepileptics, antidepressants, and local injection of an unknown drug without any improvement. An MRI of the forearm showed no pathologies, and a cervical MRI revealed multiple minimal disk lesions, but these imaging studies were of no clinical significance.
Full neurologic and musculoskeletal assessment of the left upper limb was not possible because the patient could not tolerate the examination. However, a tiny rounded tender subcutaneous nodule could be felt at the volar medical aspect of the distal third of the forearm. On gentle palpation of the nodule, the patient experienced severe electric-like pain along the entire limb. Given the character and the distribution of pain, the pain specialist suspected ulnar neuropathy. Therefore, electrodiagnostic testing was ordered, which was performed on the next corresponding week. Nerve conduction and electromyography studies of the ulnar and median nerves yielded normal diagnostic results. The patient was subsequently referred that same week for neuromuscular sonography of the left ulnar nerve and forearm.
Neuromuscular sonography was performed using an Esaote Ultrasound Equipment system (Biosound MyLab Alpha; Esaote Group, Genoa, Italy) and a 19-MHz linear-array transducer. The ulnar and median nerves were sonographically traced from the wrist to the axilla and the muscles of the anterior compartment of the forearm, as well as the associated tendons. The cross-sectional areas of the left median and ulnar nerves were measured at different levels with side-to-side comparison, and their echotexture, mobility, and vascularity were assessed. The sonogram did not identify any abnormality in the nerves, muscles, or tendons (Figures 1 and 2). However, careful sonographic examination of the most painful area revealed a well-defined small oval nodule in the subcutaneous tissue layer. The nodule was located at the volar medial aspect of the forearm, at a level 5 cm proximal to the distal wrist crease (Figure 3A). The nodule was homogeneous, hypoechoic with no evidence of calcification, and no evidence of acoustic enhancement or shadowing (Figure 3A). It was noncompressible, and nonpulsating, but demonstrated a Doppler signal (Figure 3B). The nodule measured 4.4 mm × 7.1 mm in the axial view with a cross-sectional area of 22 mm2, reached a depth of 0.5 cm, and was not directly lying over the ulnar or median nerves (Figure 4). Based on the sonogram, the diagnoses of extradigital glomus tumor, angiolipoma, angioleiomyoma, or vascular malformation like hemangioma were considered. Based on this list of diagnostic differentials, an excision biopsy was recommended.
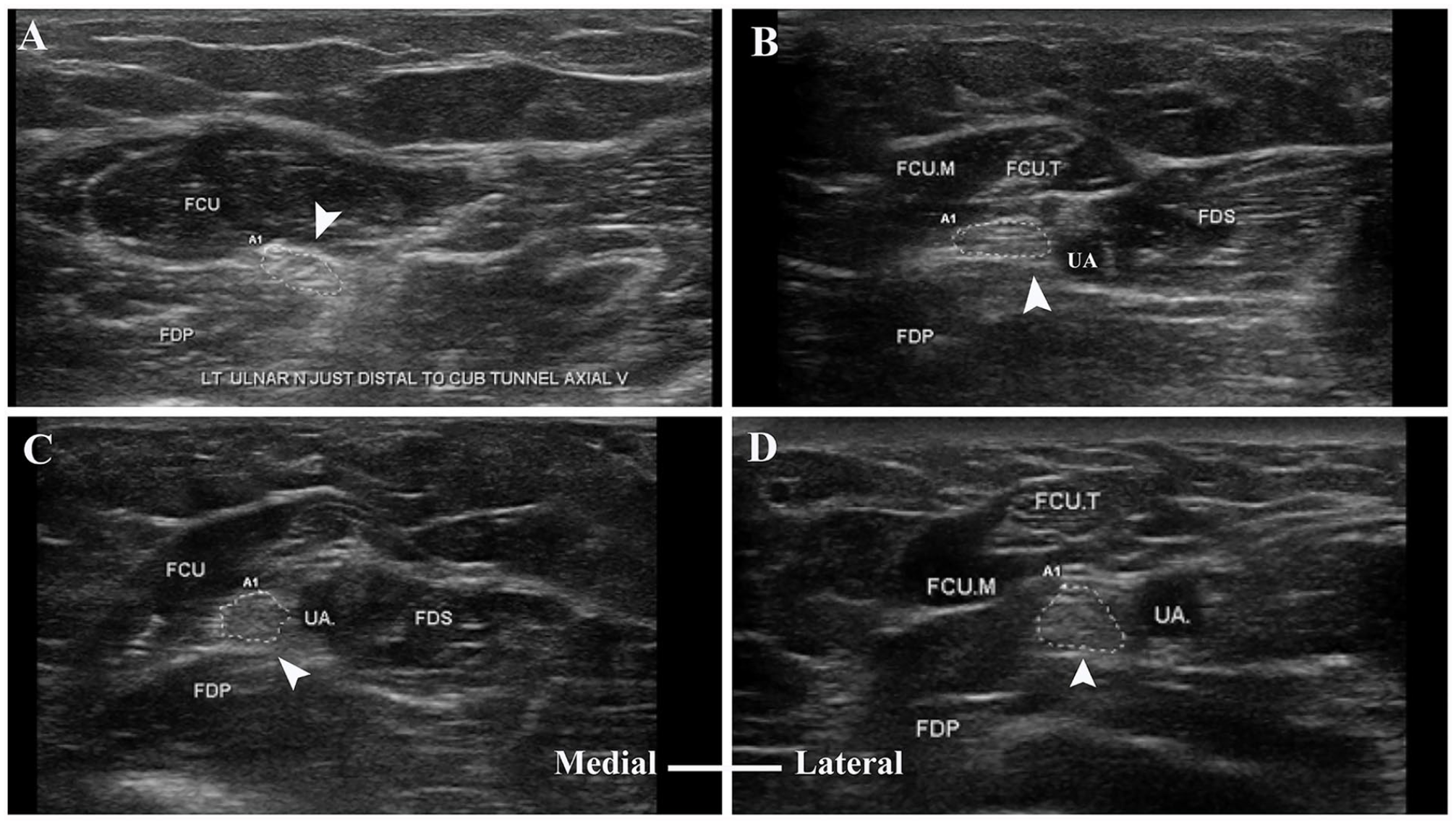
Gray-scale axial sonogram of the ulnar nerve (arrowhead) and the surrounding muscles at different forearm levels: (A) just distal to the cubital tunnel, (B) 10 cm proximal to the distal wrist crease, (C) 7 cm proximal to the distal wrist crease, and (D) 4 cm proximal to the distal wrist crease. FCU, flexor carpi ulnaris; FCU.M, flexor carpi ulnaris muscle; FCU.T, flexor carpi ulnaris tendon; FDP, flexor digitorum superficialis; FDS, flexor digitorum superficialis; UA, ulnar artery.
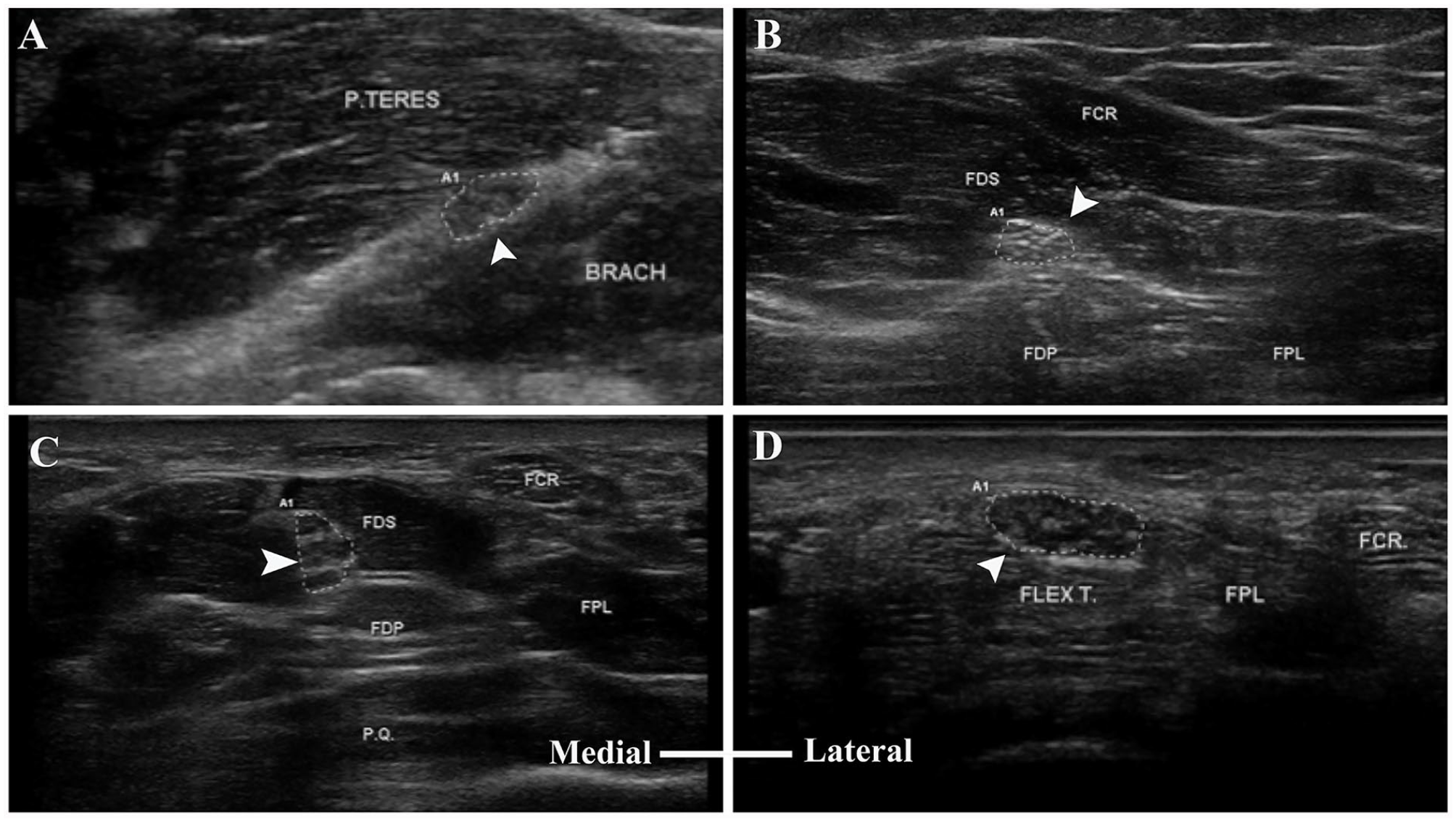
Gray-scale sonogram of the median nerve (arrowhead) and the surrounding muscles at different forearm levels: (A) just distal to the elbow, (B) midforearm, (C) distal third of the forearm, and (D) distal wrist crease. BRACH, brachialis; FCR, flexor carpi radialis; FDP, flexor digitorum profundus; FDS, flexor digitorum superficialis; Flex T, flexor tendons; FPL, flexor pollicis longus; P.Q., pronator quadratus; P.TERES, pronator teres.
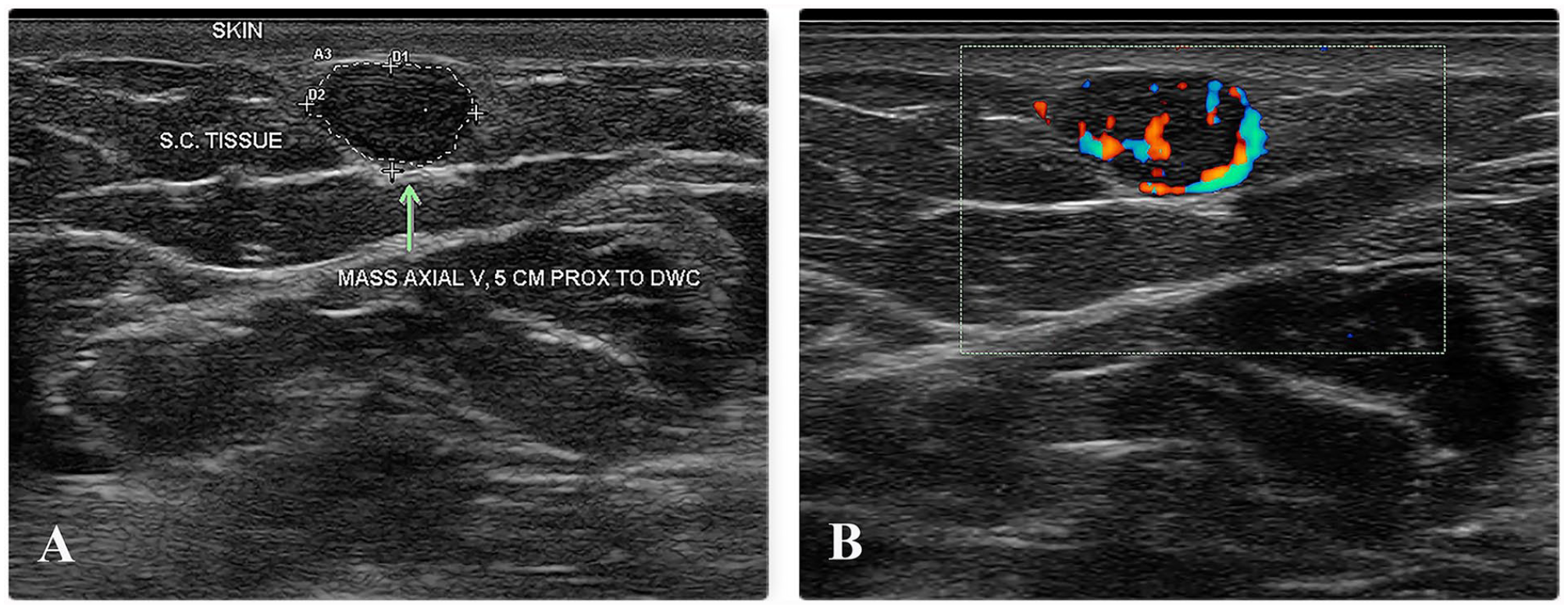
Axial images of the glomus tumor in gray-scale and power Doppler mode. (A) Axial view of the tumor with gray-scale sonography. The nodule (arrow) appeared as a well-defined hypoechoic, homogeneous, oval, subcutaneous nodule with no evidence of calcification and no evidence of acoustic enhancement or shadowing. (B) A zoom image showing vascular signal, within the nodule, on power Doppler.
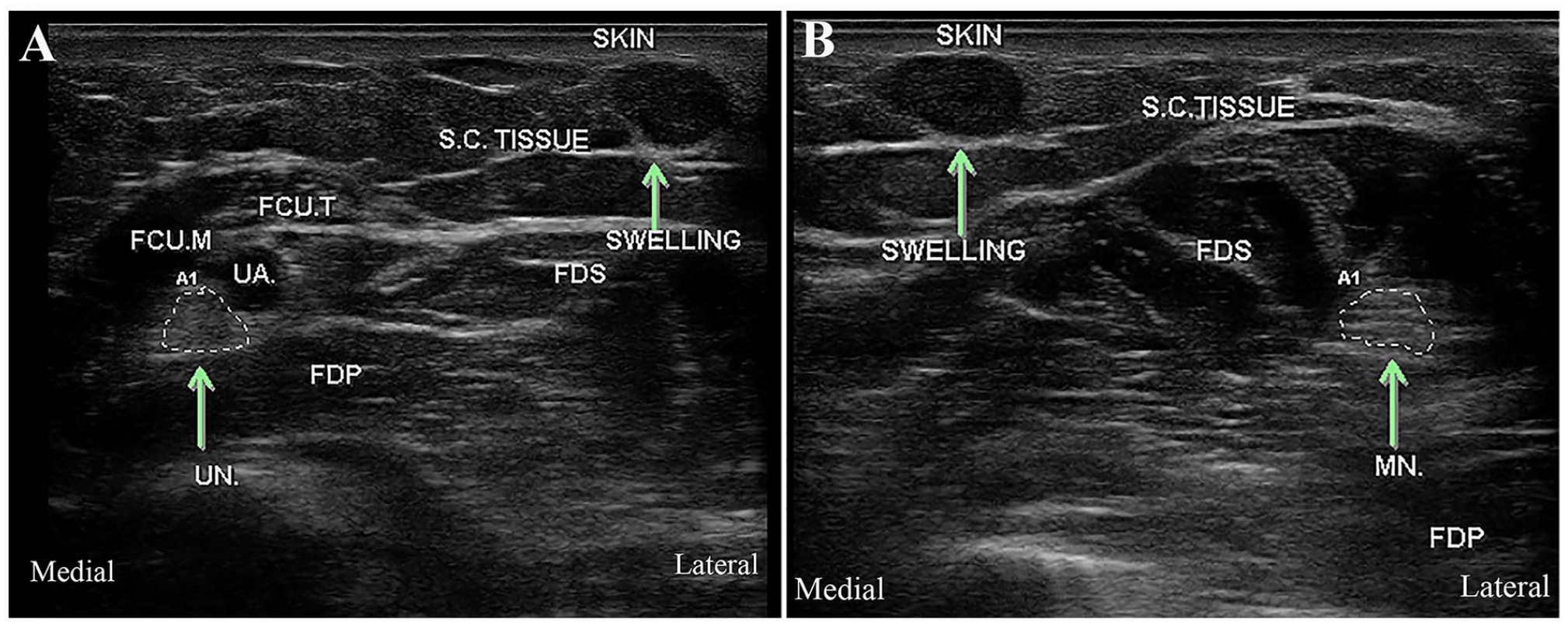
Gray-scale axial sonographic images of the forearm at the level of the nodule showing the location of the glomus tumor (arrow pointing to the hypoechoic swelling of the subcutaneous tissue) relative to the UN in (A) and to the MN in (B). The glomus tumor did not lie directly over either nerve. It lies in the region between ulnar and median nerves (lateral to the ulnar nerve and medial to the median nerve). FCU.M, flexor carpi ulnaris muscle; FCU.T, flexor carpi ulnaris tendon; FDP, flexor digitorum profundus; FDS, flexor digitorum superficialis; MN, median nerve; S.C., subcutaneous; UA, ulnar artery; UN, ulnar nerve.
The patient underwent surgical excision of the nodule under local anesthesia with infiltration of saline/adrenaline 1:200 000. A 1-cm longitudinal incision was made over the demarcated area, and a well-defined nodule in subcutaneous tissue was dissected out with complete excision (Figure 5). Subsequent histopathologic examination revealed glomus tumor. After surgery, the patient experienced dramatic and complete pain relief, which allowed the patient to resume his daily activities, without limitations.
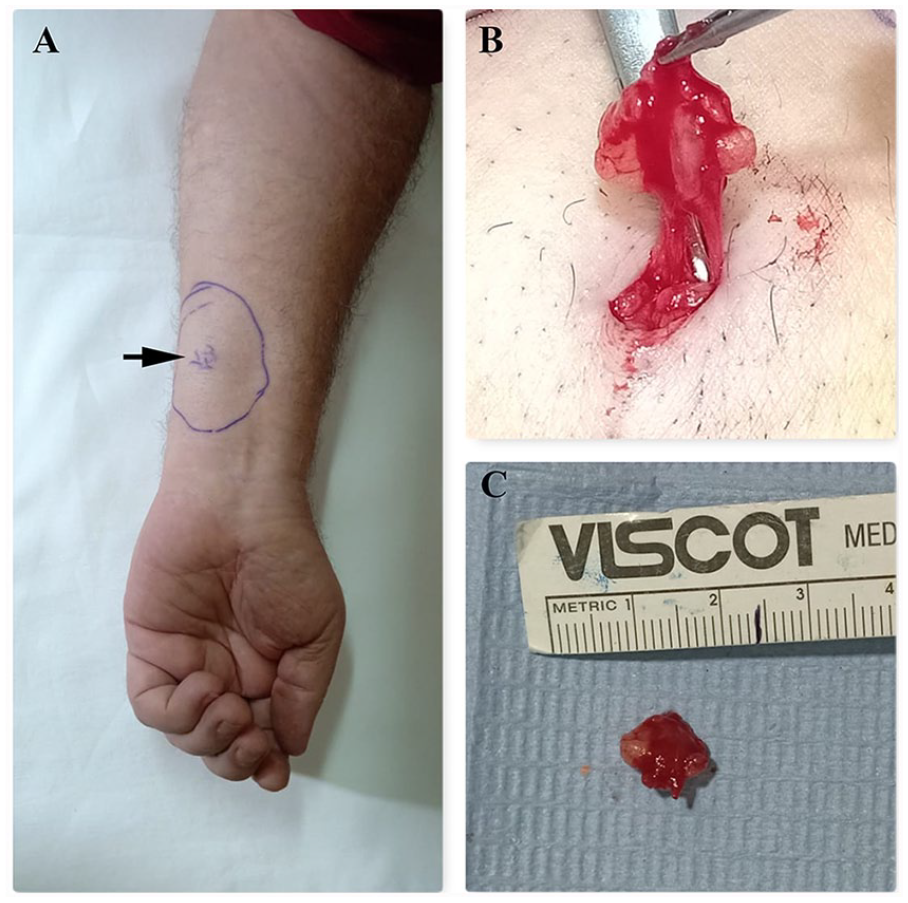
Surgical excision of the nodule. (A) Preoperative demarcation of the nodule (black arrow points to the nodule), (B) nodule dissection, and (C) the excised nodule.
Discussion
This case report documents the diagnosis of extradigital forearm glomus tumor via high-resolution sonography, in a patient with a provisional diagnosis of ulnar neuropathy. An extradigital glomus tumor can be difficult to diagnose because of its atypical location and symptoms. In this case report, the tumor atypically presented with neuropathic-like pain along the medial side of the left forearm and hand, which mimicked C8, T1 roots/ulnar nerve distribution. Similarly, previous reports described cases presented with neuropathic-like pain along the anterior thigh and tarsal tunnel3,7 The final diagnosis of both cases was extradigital glomus tumor which was detected with sonography and MRI, respectively.3,7Although MRI proved to be useful for tumor localization, 2 it may fail to diagnose some cases. 8 High-resolution sonography, with its dynamic ability and Doppler mode, can detect small tumors and determine its location, depth, size, vascularity, and relation to the surrounding structures.3,4,7
Glomus tumor typically appears on a sonogram, as a well-defined, oval or rounded, homogenously hypoechoic, noncompressible subcutaneous nodule, with a Doppler signal.2,5,9,10 Similar sonographic images can be seen in other vascular subcutaneous tumors such as angiolipoma, angioleiomyoma, or hemangioma, with some notable differences. Angiolipoma has well-defined margins and shows blood flow, but it is mostly hyperechoic and heterogeneous. 11 Angioleiomyoma can exactly resemble glomus tumors appearing as well-circumscribed, homogenously hypoechoic, and vascular nodule, but may rarely show intratumoral calcification. 12 In contrast, hemangioma may appear as hypoechoic or hyperechoic swelling, but it is usually not as homogeneous as glomus tumor, its margin is less well defined, and it may display posterior acoustic shadowing.13,14 Despite sonographic imaging difference between a glomus tumor and other aforementioned vascular tumors, these should be considered as part of the diagnostic differential of hypoechoic vascular subcutaneous masses, due to nonspecific imaging features.1,3 Thus, a histopathologic assessment is the gold standard to make the final diagnosis.
The differential diagnosis of glomus tumor does not only include other vascular subcutaneous nodules but also includes the common entities such as a neuroma, lipoma, ganglion cyst, and abscess. The differentiation between glomus tumor and these lesions with sonography is easier due to the lack of a Doppler signal. In addition, the gray-scale sonographic imaging features of those lesions are quite different from glomus tumors. The clinical features of these analogous lesions are quite different. A neuroma-in-continuity develops after nerve axonal lesion. It can cause severe neuropathic pain that increases with tactile contact. This symptom is quite similar to the pain reported by the patient, in this report. However, a neuroma-in-continuity has distinct sonographic features. In the axial view, the neuroma appears as a well-defined hypoechoic swelling in continuity with a nerve.15,16 Light pressure with the transducer, on the neuroma, usually provokes symptoms, often referred to as the ultrasound Tinel’s sign. In the longitudinal view, the neuroma appears as a focal fusiform nerve swelling. 15 Subcutaneous lipoma is most often asymptomatic. On palpation, it is felt as a soft, freely mobile subcutaneous mass with a characteristic slippery edge. The sonographic appearance of lipomas can be highly variable, but it commonly appears as a well-defined isoechoic or hyperechoic avascular elliptical or lobulated subcutaneous mass with no acoustic shadow. 17 Doppler flow may be indicative of liposarcoma. Similar to lipoma, ganglion cysts are usually painless but may occasionally cause mild pain. They commonly develop near a joint or tendon sheath and felt as cystic swellings on palpation. On a sonogram, a ganglion cyst may resemble glomus tumor and appears as a hypoechoic or anechoic noncompressible swelling with well-defined margins, but it often demonstrates internal septations and acoustic enhancement.17–19 In contrast to simple cysts, abscesses typically appear as anechoic or hypoechoic compressible swelling with thick poorly defined wall and internal septation. 17 Neurofibroma and schwannoma, the most common nerve sheath tumors, may mimic glomus tumor and manifest as a painful palpable lump. On sonography, they commonly appear hypoechoic and show internal blood flow, but they are easily distinguished from glomus tumor by their continuity with a nerve. 20 Neuroma, lipoma, ganglion cyst, abscess, and nerve sheath tumors were all ruled out in this reported case based on the clinical presentation and examination, and the absence of their characteristic sonographic features.
Conclusion
Extradigital glomus tumor can present with neuropathic-like pain and can be encountered during a neuromuscular sonogram. Thus, neuromuscular sonographers should be mindful of the sonographic appearance of glomus tumor to provide optimal care to their patients. This case report highlights the importance of careful sonographic examination of all tissue layers, including the skin and the subcutaneous tissue layers, to avoid missing non-neuromuscular pathologies. The case report also demonstrates the impact of multidisciplinary discussion in the diagnosis and management of an atypical diagnostic case.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.