
Abstract
AQUAfilling® gel has been described as human tissue biocompatible sterile synthetic material. In the literature, there are some cases presenting the complications of gel application. Rupture of implant, leakage, and migration of the gel are the most common complications. The radiologic findings due to gel leaking may mask many breast lesions including malignancy. In this case, the aim was to present the sonographic findings and elastographic features of a histopathologic-proven mucocele-like lesion in breast, due to AQUAfilling® gel injection. This appears to be a rather unique case in the literature.
Augmentation mammoplasty is a popular aesthetic application. It can be performed by either inserting an implant into the breast or applying filler injections into breast tissue, subglandular, and/or subpectoral areas.1,2 In the literature, there are many cases representing implant-related complications and additional revision surgeries. 3 Augmentation mammoplasty can be a safe and successful aesthetic application in experienced surgeons’ hands who use optimal sized, appropriate, qualified, and approved implants and/or filler injections produced by established manufacturers. 3
AQUAfilling® gel (Biomedica, Prague, Czech Republic) is a hydrofilling gel composed of 98% of sodium chloride solution (0.9%) and 2% of cation polyamide (acrylamide-co-N,N0-methylenebisacrylamide). It has been described as a human tissue biocompatible sterile synthetic material. 2 In the literature, there are some cases presenting the complications of AQUAfilling® gel application. There is a spectrum of complications from mild to serious. These complications can be defined as breast deformities, infections, and localized lumps. Gel migration and the loss or ability to breast feed are serious complications. 4 The migration of the gel can be seen in the breast tissue and imagined with radiologic methods such as ultrasonography (US) and magnetic resonance imaging (MRI). However, distant migration sites such as the parasternal region, the deep chest wall area, the lower neck, and the pelvic region have been noted. 4 In one case, gel migration was reported in the pubic region. 4 In the same case, additional long-term mastitis caused the loss of breast-feeding. 4 As the long-term side effects and safety of AQUAfilling® gel are not known, mammoplasty by using large amount of this gel should be considered carefully. 4
Based on a brief review of the literature, this is likely the first case presenting US findings, including elastographic features, of a histopathologic-proven mucocele-like lesion (MLL) in the breast and was the result of complications from a AQUAfilling® gel injection.
Case Report
A 37-year-old female patient reported to the general surgery outpatient clinic with the chief complaints of palpable, semi-soft breast masses at her right breast. In addition, lesions were painful and increased in size by time. In her history, she had received AQUAfilling® gel injection 2 years ago. The injection had been a performed by a medical aesthetician, not by an aesthetic surgeon, and had not been evaluated with any imaging method, before the AQUAfilling® gel injection. As the application of this gel material had not been performed optimally, the dispersion of gel material was not regular. Due to unsystematic, haphazard application, AQUAfilling® gel injection sites and the distribution of gel materials could not be evaluated properly. Six months after the injection, the patient had palpated millimetric breast masses at her right breast. As the masses had increased in size over time, they had become painful. Based on her history, the patient did not have any pre-existing condition which might cause this pain. She had visited another medical center with these findings. There were no abnormal findings in the patient’s laboratory tests. MRI was performed at that hospital. Yet, her MRI images were incomplete by our practice standard, and the general surgeon redirected the patient to our breast-imaging department. Standard, routine breast MRI should include precontrast T1-weighted (without fat saturation) and T2-weighted (fat saturated and/or without fat saturation) images. Other sequences are fat-saturated dynamic T1-weighted, subtracted images and late postcontrast fat-saturated T1-weighted images. In addition, diffusion-weighted images should also be included. MRI images of this particular patient, especially T2-weighted images, were missing.
The radiologic evaluation, within the authors’ department, began with a mammogram (MG). In reviewing the MG images, both breasts were noted to be very dense. There were well-defined nodular breast lesions. There was no sign of calcifications (see Figure 1). Afterward, US evaluation was performed. US images revealed that there were multiple, oval-shaped, circumscribed margined, heterogeneous cystic lesions with low vascularity (see Figure 2). These cystic lesions were located near the subcutaneous fatty tissue. The ductal structures were normal and there were no AQUAfilling® gel in the ducts. Additional elastography was also performed. In elastogram, there were mainly blue/green colors with focal red/yellow areas. These findings showed that the lesion had high elasticity which was compatible with a softer tissue. In shear wave elastography, the highest elasticity value in the lesion was 3.53 m/s, that is, 37.37 kPa (see Figure 3). Low elasticity value in shear wave elastography revealed that the lesion had intermediate malignant potential. When evaluating her previous MRI images, it was noted that there were nodular-enhancing lesions with diffusion restriction, similar to the US findings (see Figure 4). The injection sites and the distribution of nodular lesions due to the migrated gel material are shown in the diagram provided (see Figure 5). The lesions were defined as complex cystic lesions and classified as BI-RADS (Breast Imaging-Reporting and Data System) 4A. She had undergone core-needle biopsy; histopathologic diagnosis was reported as MLL (see Figure 6). In the histopathologic evaluation, there was no sign of atypia in the lesion; however, as a result of pathologic evaluation, surgical excision had been suggested by the pathologist. Unfortunately, the patient did not accept surgical excision and she did not attend any follow-up procedure.
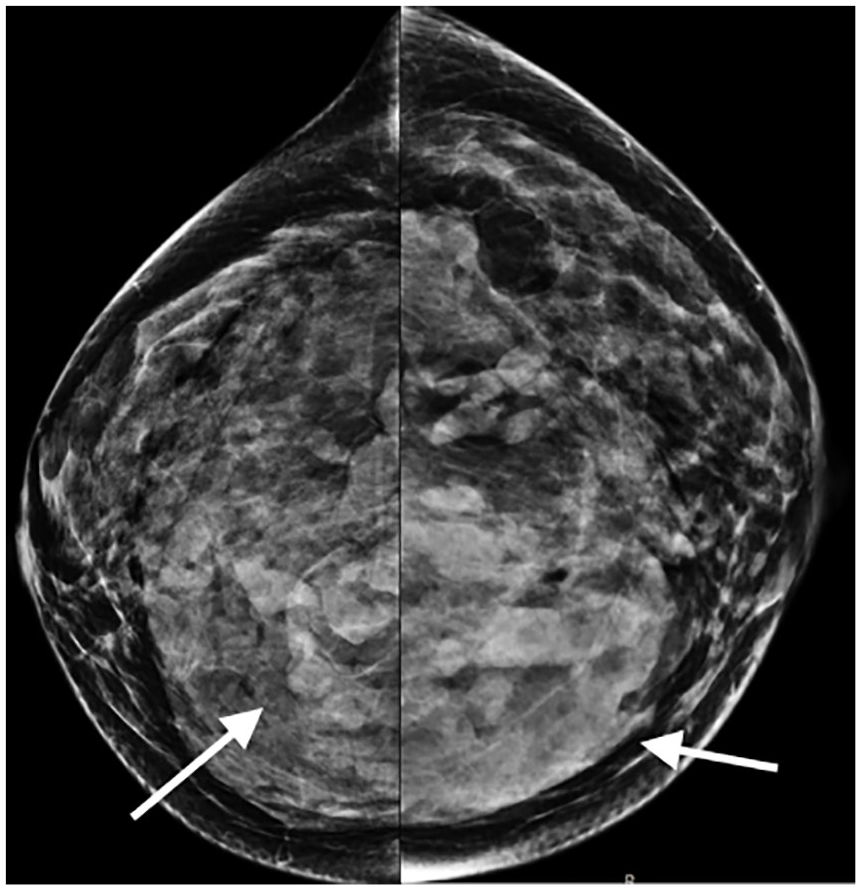
Cranio-caudal mammography images. Both breasts are noted to be very dense. There are well-defined nodular breast lesions (arrows).
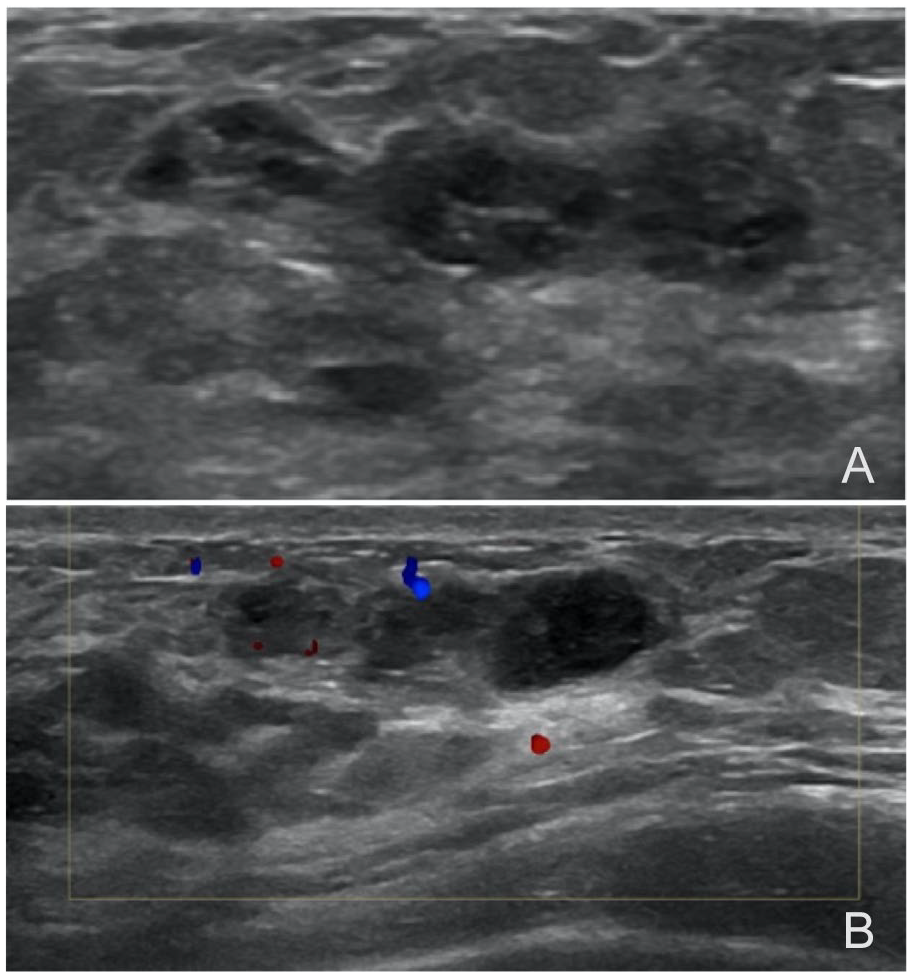
(A) Transverse ultrasonographic images show the largest one of multiple cystic nodular lesions in the breast. It was an oval-shaped, circumscribed margined, multicystic nodular lesion, and (B) color Doppler evaluation demonstrated low vascularity in the lesion.
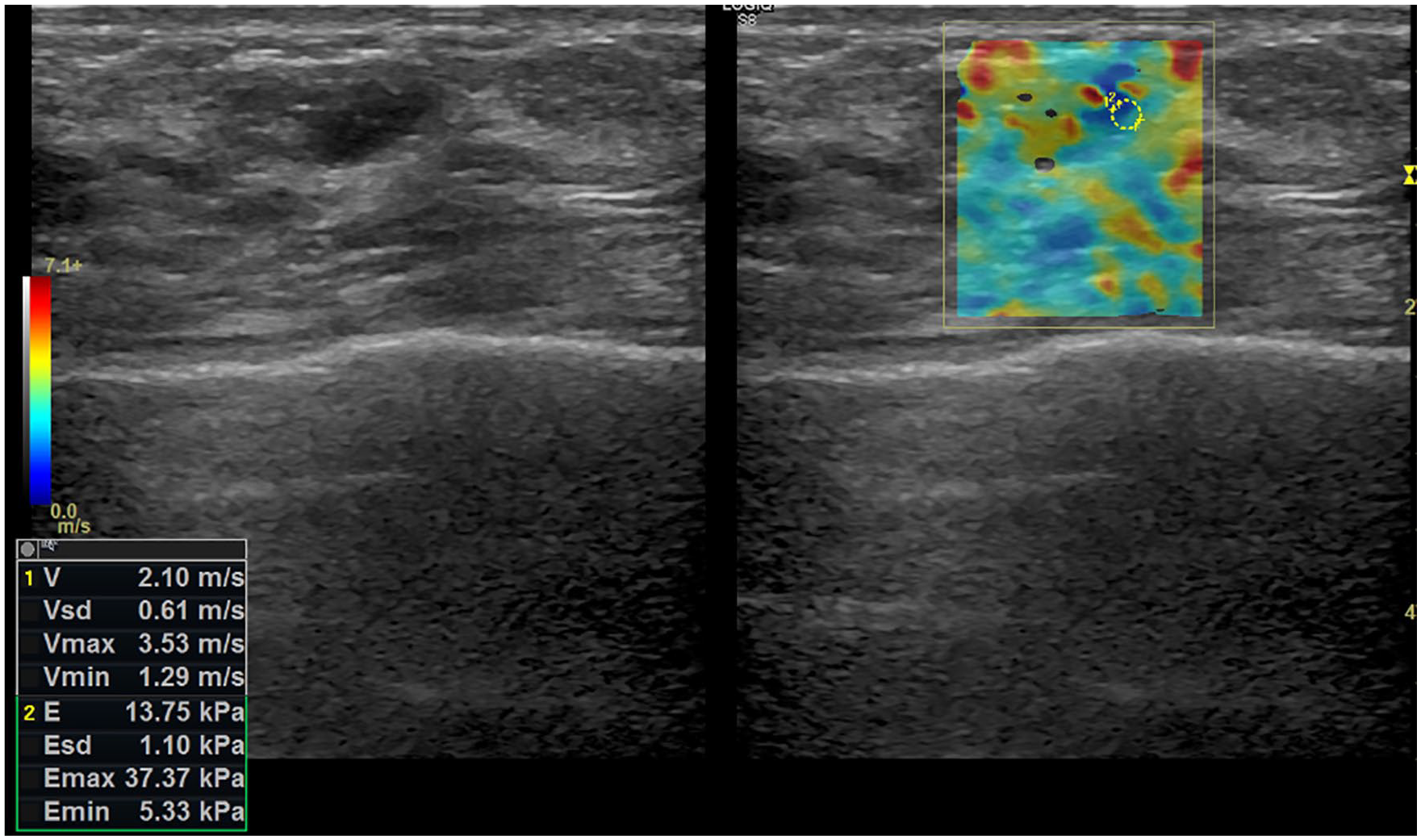
The elastogram reveals that the lesion includes mainly blue/green colors with focal red/yellow areas. This finding shows that the lesion has soft structure. In shear wave elastography, the highest elasticity value in the lesion was measured as 3.53 m/s, that is, 37.37 kPa.
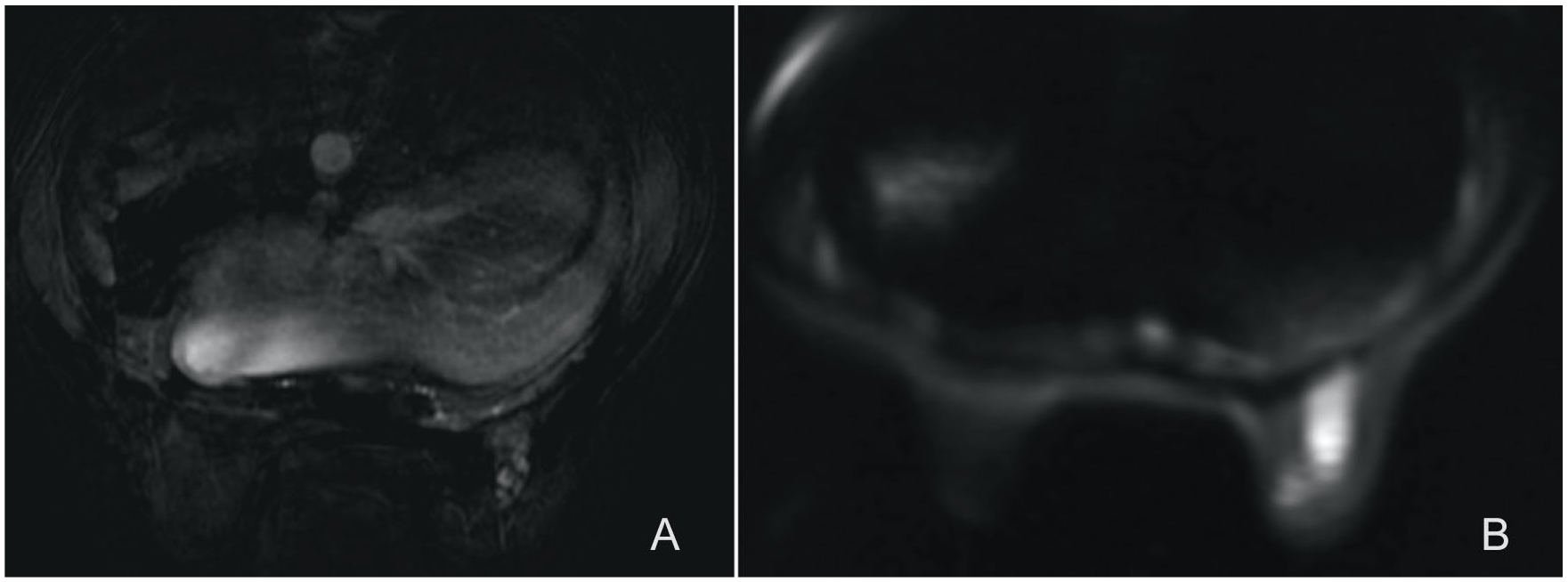
Magnetic resonance images of the patient: (A) dynamic subtracted image and (B) diffusion-weighted image. There are nodular-enhancing lesions with diffusion restriction.
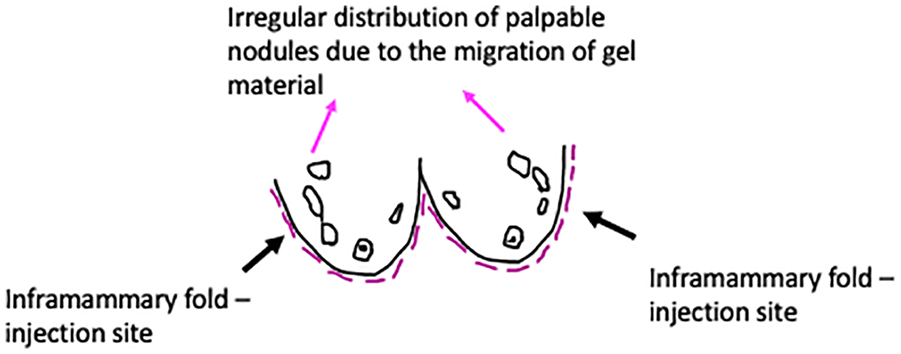
This diagram shows the injection sites and the distribution of nodular lesions due to the migrated gel material.
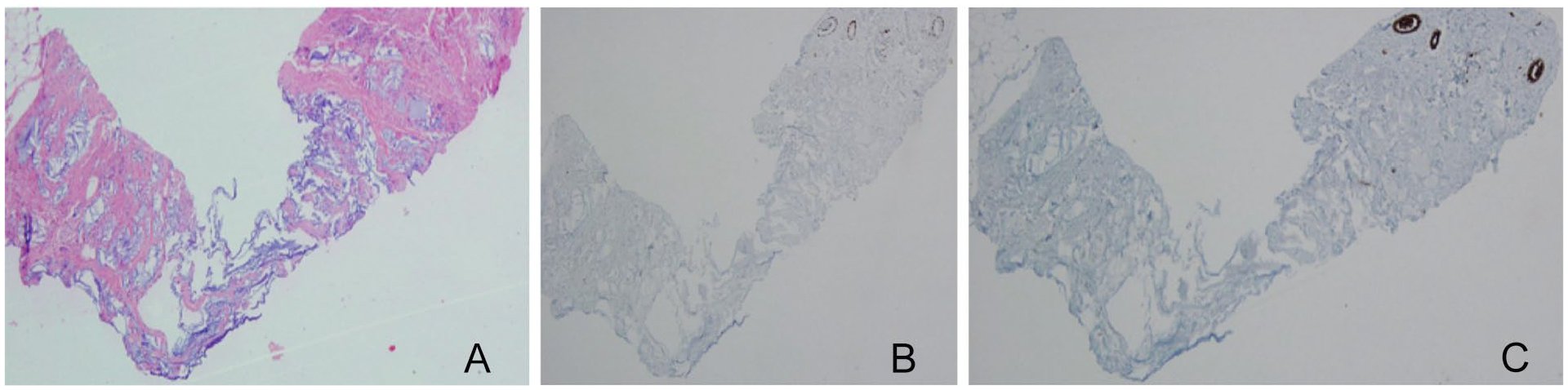
Evaluation of the core-needle biopsy specimen: (A) H&E stain, (B) p63 stain, and (C) pancreatin stain. Histopathologic evaluation shows mucocele-like lesion. Dilated ductus is filled with mucin. The lesion is not stained by p63 and pancreatin stains.
Discussion
Breast tissue is formed by a mixture of fibroglandular and fatty tissues. The amount of fibroglandular tissue is more at the upper lateral quadrant. As a result of hormonal fluctuation, fibroglandular tissue shows changes. Fibroglandular tissue decreases as the age increases. In a sonographic examination of normal breast tissue, fatty tissue is seen as a dark or hypoechoic echo pattern, whereas the echo patterns of fibroglandular tissue are light gray or hyperechoic. 5
AQUAfilling® gel is a dermal filling material correcting and filling the lips to increase the volume and to reform lip shape, facial asymmetry, and wrinkles. 6 This gel is also used for breast augmentation. Application of AQUAfilling® gel is administered under local anesthesia. The gel materials are injected into the retroglandular site of the breast through an incision at the lateral side of inframammary fold without the guidance of an imaging method. 2 The application of this material requires experience and attention. In an US evaluation, AQUAfilling® gels are seen as heterogeneous-hypoechoic fluid collections. These collections are seen symmetrically at retroglandular sites when the applications are performed appropriately. 7
AQUAfilling® gel has not been approved by Food and Drug Administration because of various complications. In fact, it was prohibited in some countries because of complications.6,8 However, this gel was approved in Europe in 2008 and is still in use in some countries such as Turkey, Serbia, Malaysia, Japan, and Korea. 4 In the literature, it has been reported that there are some adverse effects of the polyacrylamide material. These effects can be classified as gel migration, infection, breast deformities, asymmetry, tenderness, breast swelling, pain, deficiency in breast-feeding ability, and even systemic pain. 9
The radiologic findings due to leaking gel may mask many breast lesions including malignancy; it is very important to diagnose this complication. 10 The migration is commonly seen in the neighborhood soft tissue such as between the pectoral muscle fibers and subpectoral components. 7 Gel migration can be to the parasternal area, the deep site of the chest wall, and lower neck; it can also be to the pelvic area. Radiologic findings of gel leakage and migration differ. 11 MG findings are nonspecific, and most MG images are not diagnostic as the breasts have very dense characteristics after gel injection. 10 Additional imaging methods including MRI and US must be applied for optimal and correct diagnosis.
On MRI, the signal of gel collections is hyperintense on T2-weighted images and hypointense on T1-weighted images. Also, hypointense T2 signals may be seen. 10 If there is inflammation, signals on T1- and T2-weighted images change. Contrast enhancement is seen additionally. 12 Both MRI and US provide optimal guidance to show the exact injection site where a large amount of injected gel can be imagined. In addition, MRI helps to evaluate normal residual breast tissue. 13
Ultrasonography is a useful diagnostic method. It reveals heterogeneous, hypoechoic, and/or anechoic liquid collections of different sizes. These liquid collections have thickened capsules. 12 Elastography has a high specificity in discriminating between malignant and benign lesions. Lesions with soft tissue characterization like in the present case report have less stiffness and color distribution compatible with the less stiffness in elastograms. 14 Because of the liquid and soft content of the lesions in this case, the lesions were soft with low elasticity rates.
MLL is one of the rare lesions of the breast. It is characterized as mucin-containing dilated epithelium-lined ductal structures.15,16 As a large spectrum of pathologies from atypic ductal hyperplasia to ductal carcinoma in situ have similar histologic structures, further evaluations are important in the exact diagnoses of dilated epithelium-lined ducts. 15 In addition, it has been stated that MLL can be a precursor lesion, including mucinous ductal carcinoma in situ and invasive mucinous carcinoma. 17
In MLLs, MG findings are commonly associated with coarse calcifications. Nevertheless, mass images can also be seen. 18 Ultrasonography findings have a wide spectrum. Generally, lesions have complex cystic lesion characteristics. 19 MRI shows focal enhancement areas. 19 In the literature, radiologic findings of MLL lesions to discriminate benign lesions from malignant ones are described as nonspecific findings. Only a few specific imaging characteristics of malignant MLLs have been reported. 20 In MG examinations, wider extended microcalcifications are more frequent in malignancy-associated MLLs than benign MLLs. 20 In one study, ultrasonography findings of malignancy-associated MLL are reported as cysts with thick septations, complex cystic lesions, and clustered cysts. 20 MG findings in our case were nonspecific, whereas US and MRI findings in our case had similar features with the literature.
It would appear that this is the first case reporting elastography findings of MLL in the literature. In addition, in this case, another important characteristic was the histopathologic diagnosis. This is the first case in the literature presenting histopathologic-proven MLL after AQUAfilling® gel injection.
Conclusion
AQUAfilling® gel injections performed by unsafe and inexperienced hands may cause many complications. As the current aesthetic application numbers increase, the possibility of these complications increases also. Once a complication occurs, diagnosis and corrective treatments are difficult. As the material has high toxicity, the leakage of this gel material has high influence on the surrounding breast tissue. The structure of normal breast tissue is disturbed. Radiologic evaluation is very important. The diagnoses of the nature and the sites of the complications can be realized with radiologic evaluations, especially with US examination. In addition, radiologic features enable us to diagnose exact sites of the complications and the decision of the appropriate treatment options. To determine the best approach in managing symptomatic patients, clinicians must be aware of the complications caused by AQUAfilling® gel. Radiologists should also be aware of the specific imaging findings of MLL as a possible differential diagnosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient for the publication of the case report and the accompanying images.