
Abstract
A plunging or diving ranula is a rare mucous fluid collection in the submandibular or parapharyngeal space resulting from damage or rupture of one or more ducts of the sublingual gland. The most common clinical presentation is a painless, slow-growing, pliable mass in the floor of the mouth, sometimes extending below the mandible through a defect in the mylohyoid muscle. This case report presents a young female patient who was suspected of having a plunging ranula. This case also highlights the role that sonography and other diagnostic tools play in the evaluation of this phenomenon.
Recognized over 1000 years ago during the Byzantine era, the term ranula is derived from the word rana, which is Latin for frog, as the swollen appearance of the sublingual mucous membranes resembles the translucent underbelly of a frog.1–7 There are two types of ranulas: simple and plunging. Sublingual ranulas form underneath the mucous membranes of the floor of the mouth above the mylohyoid, whereas plunging ranulas “plunge” by extending below the mylohyoid into the submandibular or parapharyngeal space, presenting as neck masses.2–3 Multiple surgical techniques have been used, ranging from marsupialization, incision and drainage, excision of the ranula only, excision of the sublingual gland along with ranula, and sclerotherapy. Recurrence rates vary depending on type of procedure performed. It has been noted that because these extravasation cysts originate from the sublingual salivary gland, excision of the sublingual gland along with ranula is the most effective treatment.1,5,6
Case Report
A 25-year-old female patient presented with a 4-month history of a unilateral, nontender, enlarging, soft submental mass, extending to her right submandibular region. There was no history of trauma, infection, or any oral or neck surgical procedures. Physical examination demonstrated a diffuse, oval, soft tissue prominence with normal overlying skin extending from the right mandible to the submental region. A sonogram was ordered to further characterize the mass (see Figures 1 and 2).

Anterior view of submental mass.

Longitudinal view of submental mass.
The patient’s area of diffuse swelling was scanned using a submental approach with a high-frequency ML6-15 linear-array transducer (GE Logiq 9; GE Healthcare, Waukesha, WI). Sonographic findings included a large cystic mass with two components. The more superficial component measured 3.6 × 1.3 × 2.9 cm. The deeper component measured 3.7 × 2.9 × 1.3 cm and extended along the medial aspect of the mandible. Communication between the two components was identified during sonography. A portion of the sac plunged through the muscle fibers of the mylohyoid into the submental space, consistent with a diving or plunging ranula. Color Doppler was used and demonstrated no vascularity associated with the mass. There was no associated lymphadenopathy in the area of the mass (see Figures 3 and 4).
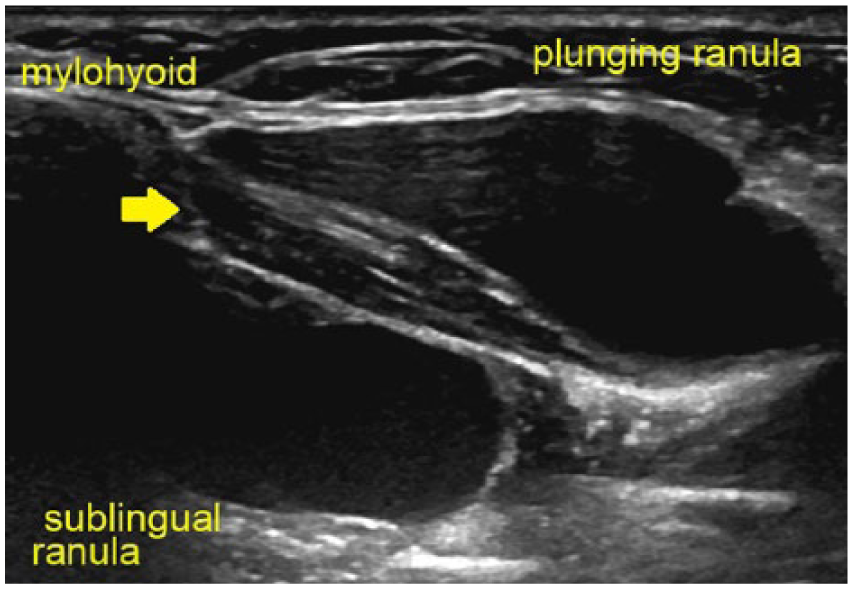
Longitudinal sonogram demonstrating cystic fluid collections on both sides of the mylohyoid (arrow).
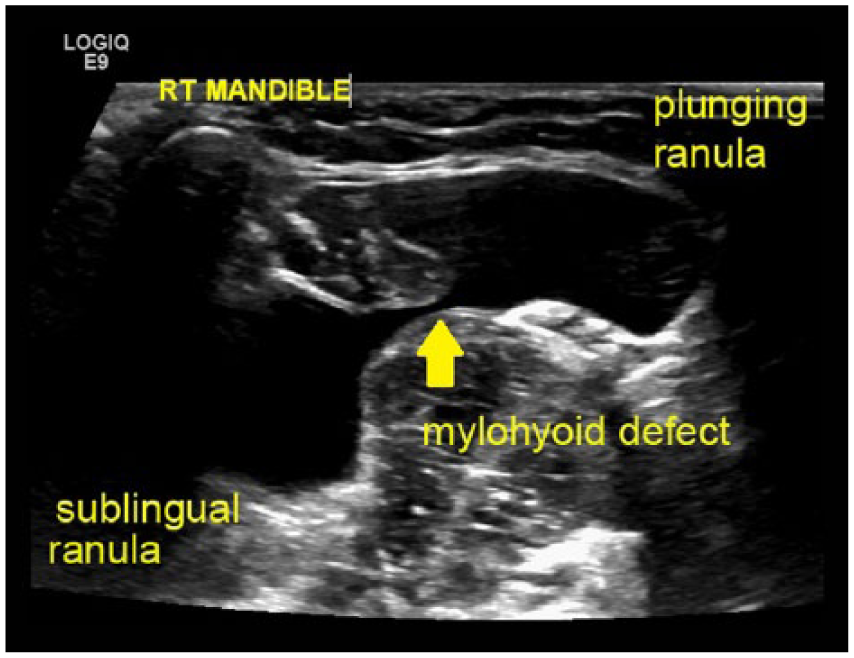
Transverse sonogram of the sublingual and plunging ranula through a defect of the mylohyoid (arrow).
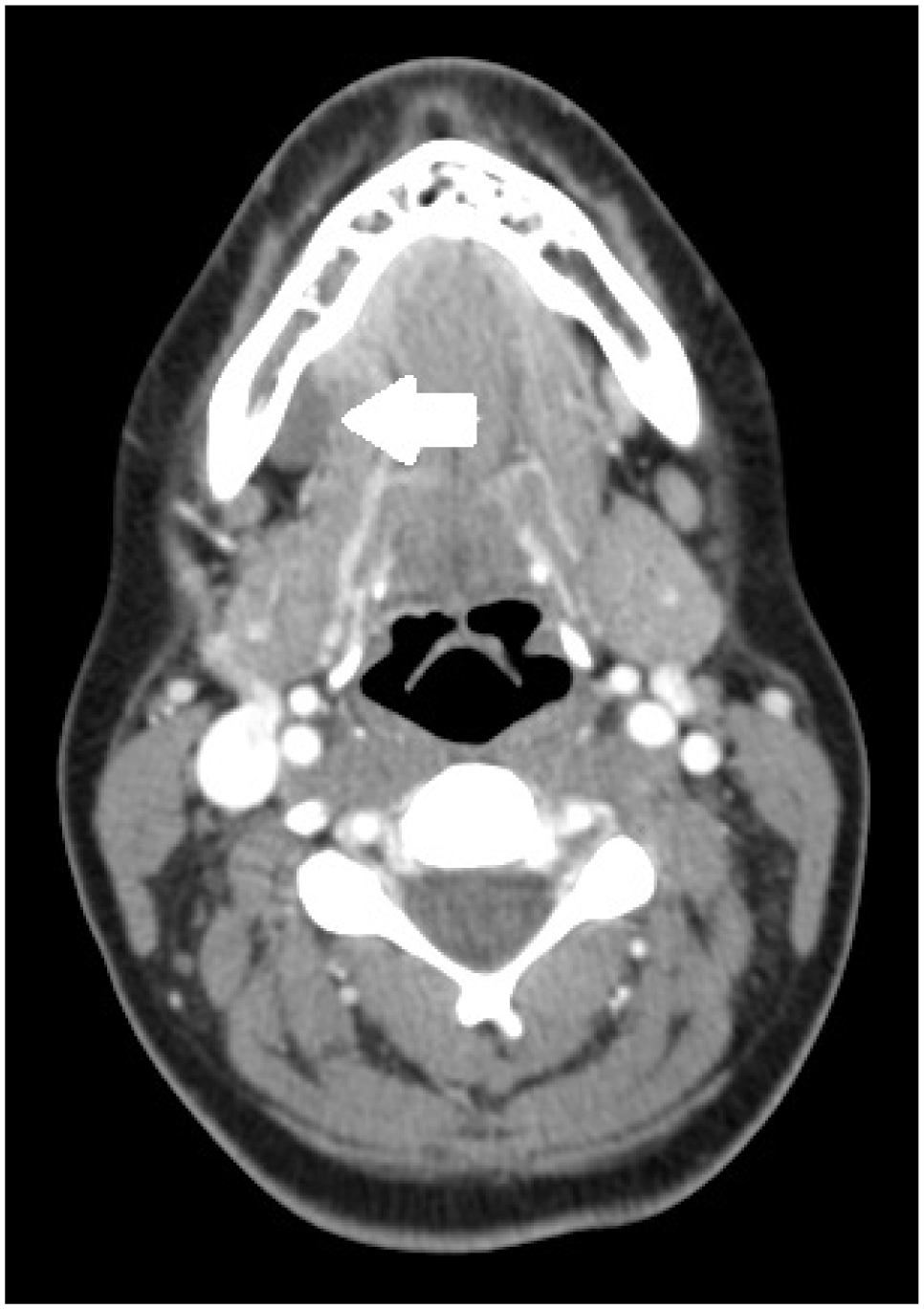
A computed tomography (CT) examination, performed 3 weeks later, confirmed the sonographic findings. A marker was placed on the region of clinical concern and corresponded to a cystic-appearing lesion in the submental space, level 1A, projecting to the right of midline. The submental component communicated through the floor of the mouth with the sublingual component, which was medial to the mandible and immediately posterior to the right sublingual gland. No other soft tissue or bony abnormality was observed (see Figures 5–8).

Contrast-enhanced longitudinal computed tomography image of the plunging ranula (arrow).
Contrast-enhanced axial computed tomography image of the sublingual ranula (arrow).

Contrast-enhanced axial computed tomography image of the plunging ranula (arrow).
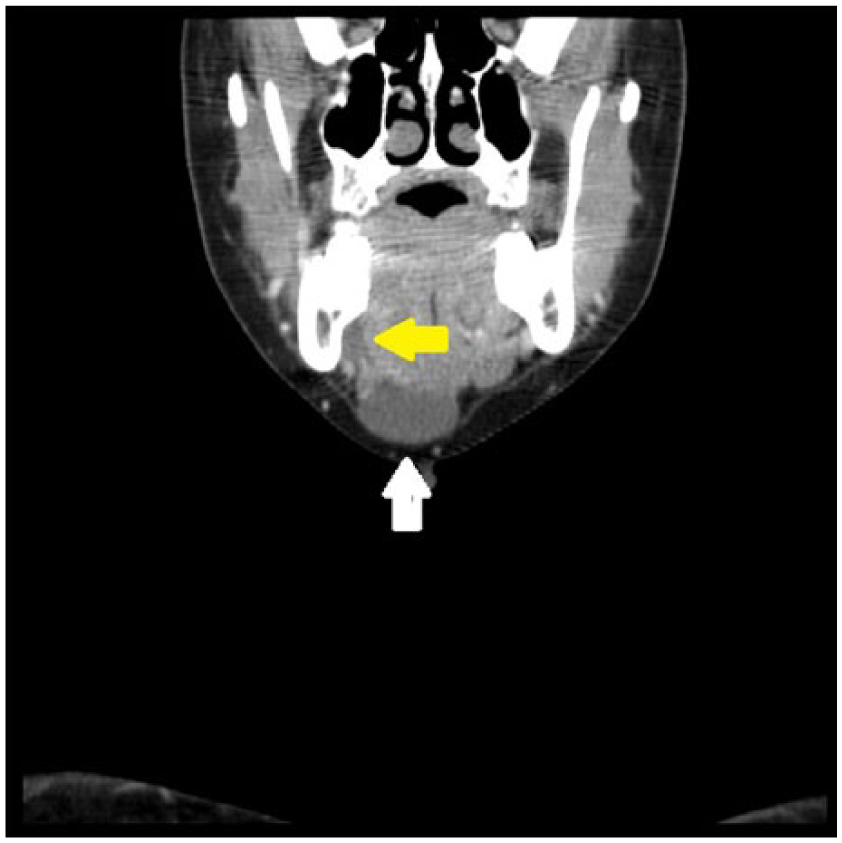
Contrast-enhanced coronal computed tomography image of the sublingual ranula (yellow arrow) and plunging ranula (white arrow).
The patient underwent surgical excision of the right sublingual gland and associated ranula with no complications. Pathology demonstrated a normal sublingual gland with mucocele and no other associated abnormality.
Discussion
Lying within the floor of the oral cavity, inferior to the tongue, medial to the body of the mandible, and anterior to the submandibular glands, are a pair of sublingual glands. These glands are the smallest, weighing about 2 g and shaped like an almond. Each gland drains into a row of 12 to 20 short excretory ducts, known as ducts of Rivinus, that open into the floor of the mouth along the summit of the sublingual fold2,3,6 (see Figure 9).
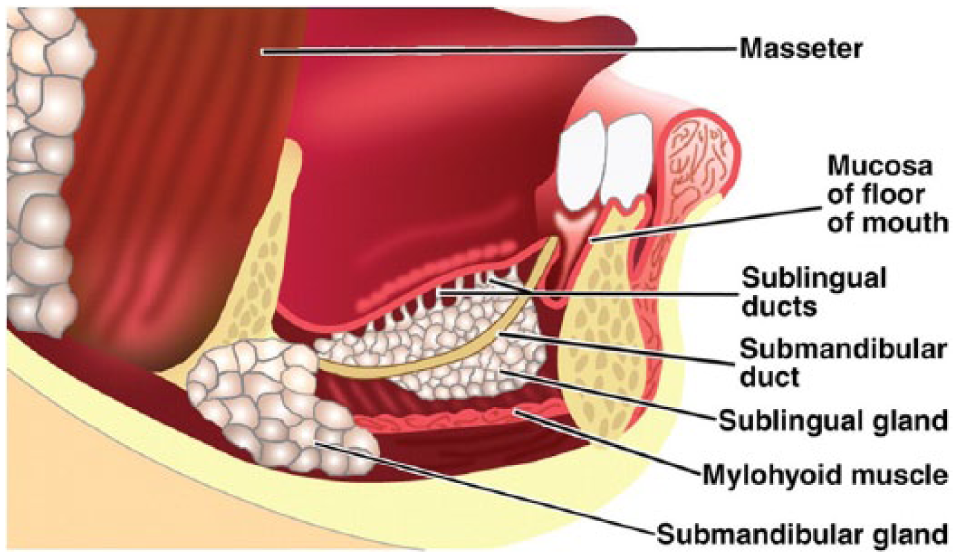
Salivary gland anatomy. Copyright ©2010 Radiological Society of North America, Inc. (RSNA). Reproduced with permission from the RSNA. All rights reserved.
Trauma, obstruction, or inflammation can damage one or more ducts, causing leakage of salivary contents into the surrounding tissue, inducing a fibroblastic reaction that seals the mucus in a connective tissue sac, referred to as an extravasation pseudocyst. This is the most common type of ranula.1–4,8 In less than 10% of all ranulas, congenital obstruction, by either an imperforate salivary duct or an ostial adhesion, leads to the formation of a retention cyst.5–7
The typical clinical manifestation of a ranula is a slow-growing (usually unilateral but can be bilateral), pliable, painless mass in the floor of the mouth. Reported dimensions range from 4 to 10 cm, and they account for 6% of salivary mucoceles (also called sialocysts), with a prevalence of about 0.2 cases per 1000 persons.1,5,9 There seems to be a higher frequency among young adults in their second and third decades as well as in children younger than 10 years, with a slight female preponderance.7,10–12
Sublingual ranulas form above the mylohyoid muscle, within the sublingual space, and are most commonly observed as a bluish cystic lesion below the tongue. When the fluid pressure of the mucocele ruptures and dissects through the mylohyoid muscle into the submandibular or submental space, it is termed a plunging or diving ranula.1–6,9,11–12 These extravasation cysts tend to extend into the submandibular triangle but have been observed to extend superiorly into the parapharyngeal space as far as the skull base, inferiorly into the supraclavicular area and upper mediastinum, or posteriorly into the retropharyngeal space.2,7,12
Some physiologic mechanisms that contribute to plunging ranulas have been proposed5–7,13:
Projection of the sublingual gland through the mylohyoid muscle or the development of an ectopic sublingual gland on the cervical side of the mylohyoid could explain the etiology of plunging ranulas without an oral component.
In 27% to 45% of cadavers, a congenital dehiscence in the mylohyoid muscle, known as the boutonnière of Gaughran, has been noted. This could provide a route of egress for a simple ranula through the defect.
An aberrant sublingual gland duct may join a submandibular duct (or the submandibular gland), allowing ranulas to form in continuity with the submandibular gland and accessing the neck beyond the mylohyoid muscle.
Approximately 45% of plunging ranulas form following surgical intervention of sublingual ranulas or secondary to surgical procedures.
Plunging ranulas are usually seen in conjunction with a sublingual ranula and rarely form independent of the oral component. 10 In 45% of cases, the first presentation is intraoral swelling; 34% of those reported cases are associated with plunging ranulas. However, 21% of plunging ranulas occur without oral involvement. 5
Arunachalam et al. 12 suggested that infantile and pediatric ranulas may be secondary to duct agenesis or hypoplasia or due to birth trauma. A retrospective analysis performed by Sigismund et al. 14 demonstrated a mean age of 33 years at the time of surgical intervention.
Some examples of surgical intervention procedures include the following1,6,12–14:
Excision of the plunging ranula along with the involved sublingual gland is considered the most accepted method with almost zero recurrence rate.
Marsupialization with or without packing, and with or without cauterization of the lesion, has been a less favorable option because of the reported recurrence rate, which can vary from 61% to 89%.
Incision and drainage via intraoral approach (or excision and drainage via extraoral approach) of ranula alone demonstrates limited success, with an 85% recurrence rate.
Sclerotherapy with OK-432 (streptococcal preparation) is the least invasive procedure, with a 100% cure rate. However, multiple treatments (of up to three injections) may be required before clinical resolution.
Histopathologically, plunging ranulas are pseudocysts with no epithelial lining.1,3,4,6 The walls are composed of fibroconnective tissue resembling granulation tissue, formed in response to the inflammatory effects of salivary secretion. Fluid aspirate cytology demonstrates yellowish mucus with histiocytes. Biochemical analysis will reveal a higher content of amylase and protein compared with serum, which validates that the origin is from the sublingual gland instead of submandibular gland secretions, which have lower protein content.1,2,6,15 In contrast to the submandibular and parotid glands, the sublingual gland is uniquely characterized by permanent mucus excretion, with or without the presence of stimuli, that contributes to its vulnerability in developing extravasation cysts.6,7,10,16
A palpable mass in the neck is a common clinical presentation. If the patient is younger than 40 years and presents with a unilateral, soft, slow-growing, poorly defined, painless swelling in the submandibular triangle, a plunging ranula should be the first suspect. 17 Clinical diagnosis is based on the presence of amylase in fluid aspirate. 17 Imaging studies such as sonography, CT, or magnetic resonance imaging (MRI) can be performed to confirm the clinical diagnosis and outline the extent of involvement before treatment.1,2,4,5,8 Jain et al. 17 reviewed 33 plunging ranula cases in a 4-year period with high resolution sonography and was able to demonstrate a dehiscence in the mylohyoid in 100% of their cases. In a separate summary by O’Connor et al., 6 90% of patients with a plunging ranula had an associated mylohyoid defect.
In this case, the patient’s plunging ranula was located on the right side. Sigismund et al. 14 and Patel et al. 18 reported an equal distribution between right and left oral ranulas. In contrast, for plunging ranulas, a 70% right-side preponderance was observed during analysis of retrospective data. 18
Sonographically, the sublingual glands are difficult to image because of their location. A plunging ranula is more easily visualized because of its more superficial location and appears as an anechoic, avascular structure with thin walls, incomplete septae, and possibly fine internal echoes representing debris. Cross-sectional imaging such as CT or MRI is a helpful supplement in evaluating the deeper tissue layers that sonography cannot completely assess. The presence of a homogeneous cystic structure within the submandibular or parapharyngeal space that abuts the sublingual space is strongly suggestive of a plunging ranula. If a tail extending into the sublingual space is observed, this feature is almost pathognomonic for plunging ranulas.3,6,9,12,14,15
Although the floor of the mouth is a small region, a myriad of pathologic processes can occur: cystic lesions, inflammatory conditions, vascular lesions, and benign and malignant neoplasms. Differentials of cystic lesions that manifest within the same region include lymphatic malformation (cystic hygroma), thyroglossal duct cyst, dermoid or epidermoid cyst, lipoma, laryngocele, hemangioma, and lymphadenopathy.1,5,16,19–21 On cross-sectional imaging, certain lesions such as an epidermoid or dermoid cyst with homogeneous internal content can be indistinguishable from a plunging ranula. Confirmation can be made by fine needle aspiration cytology, which will demonstrate putty-like keratin content. 20 Cystic hygromas tend to be infiltrative and multiloculated, with thin septae, and involve anatomic regions not typically occupied by ranulas.9,17,22 Aspirated fluid from these lymphatic malformations appears milky or watery and contains cholesterol crystals, protein, lymphoid, and endothelial cells. 6 Congenital cysts such as thyroglossal duct cysts are typically situated midline just superior to the hyoid bone.15,17 Abscesses are usually associated with pain and tenderness. 17 Bimanual palpation by the provider coupled with conventional radiography is not helpful in differentiating the lesions. A detailed patient history along with sonography, CT or MRI, and cytology of the aspirated fluid can play a significant role in making a correct diagnosis.
Conclusion
Neck masses are a common clinical presentation and can present a diagnostic dilemma for clinicians, as several benign and malignant lesions share similar imaging features. Sonography is the preferred tool in many practices for the evaluation of superficial neck masses. Sonography is a preferred modality because it is inexpensive, noninvasive, and nonionic and provides excellent soft tissue delineation of the tissues of the neck. In addition to reliably distinguishing between solid and cystic masses, high-resolution sonography is capable of assessing the integrity of the mylohyoid muscle, determining the extent of a plunging ranula, and as observed in this rare case, demonstrating the extension of the mucocele through a mylohyoid defect into the submental region.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.