
Abstract
Medial meniscocapsular separation (MCS) is an uncommon knee injury. No dedicated sonographic study on medial MCS has been reported thus far. This article retrospectively analyzes the sonogram of two patients with medial MCS confirmed by either magnetic resonance imaging (MRI) or surgery. Both patients are in their 30s with sports-related medial knee injuries. Sonograms of their medial knees displayed similar features of fluid collection between the medial meniscus and the deep portion of the medial collateral ligament (MCL), and an unsmooth outer surface of the meniscus. Meniscal tear and MCL injury were also found in both of these patients. Sonographic diagnostic criteria for the medial MCS are proposed based on the two patient cases. The differentiation of medial MCS from other cystic lesions in the medial parameniscal area is also discussed.
Keywords
Meniscocapsular separation (MCS) is the detachment of the meniscus from its outer capsular attachment.1,2 It is usually due to a twisting injury of the knee. 1 This injury is uncommon. It happens more often in the medial knee than in the lateral knee. 2 The symptoms and signs are nonspecific, which include knee pain, instability, swelling, and tenderness. Imaging diagnosis of MCS by magnetic resonance imaging (MRI) has been described in multiple studies.1,3- 7 However, there is only one published sonographic case of posterior lateral MCS, and one case using arthroscopy combined with sonography for the diagnosis and treatment of MCS.8,9 The current presentation describes two cases of medial MCS with an attempt to explore the sonographic diagnostic criteria of medial MCS. To help understand this report, a review of the anatomy of the medial capsuloligamentous complex is provided.
The supporting structure of the medial knee is the medial capsuloligamentous complex, which is composed of three layers.1,10,11 Layer 1 is the superficial layer, consisting of the deep fascia from the continuity of the fascia overlying the vastus medialis anteriorly and the sartorius posteriorly. Layer 2 is the intermediate layer, which is the superficial portion of the medial collateral ligament (MCL) (Figure 1A and B). It is a strong, flat, and straight vertical fibrous band in the middle third of the knee with one proximal femoral attachment and two distal tibial attachments.11,12 Layer 3 is the deep layer, which is the deep portion of the MCL and is a thickening of the medial joint capsule. It interlaces with the medial meniscus (meniscocapsular area) and attaches superiorly and inferiorly to the articular margins of the joint to form the meniscofemoral and meniscotibial ligaments (Figure 1A and B).1,10,12 With medial MCS, these two ligaments may be involved in injuries, such as tears. 1 Layers 1 and 2 fuse anteriorly to form the medial patellar retinaculum.1,10 Layer 2 also joins layer 3 in the posterior third of the medial aspect of the knee to form the posterior oblique ligament, which is closely attached to the posteromedial meniscus.1,10 Between layers 2 and 3 (the superficial and deep portions of the MCL), a bursa is located along the middle third of the medial knee. When the knee flexes, the bursa allows the MCL to glide over the bony surfaces of the tibia and femur without friction. 13 The function of the MCL is to prevent valgus stress and abnormal external rotation of the knee.
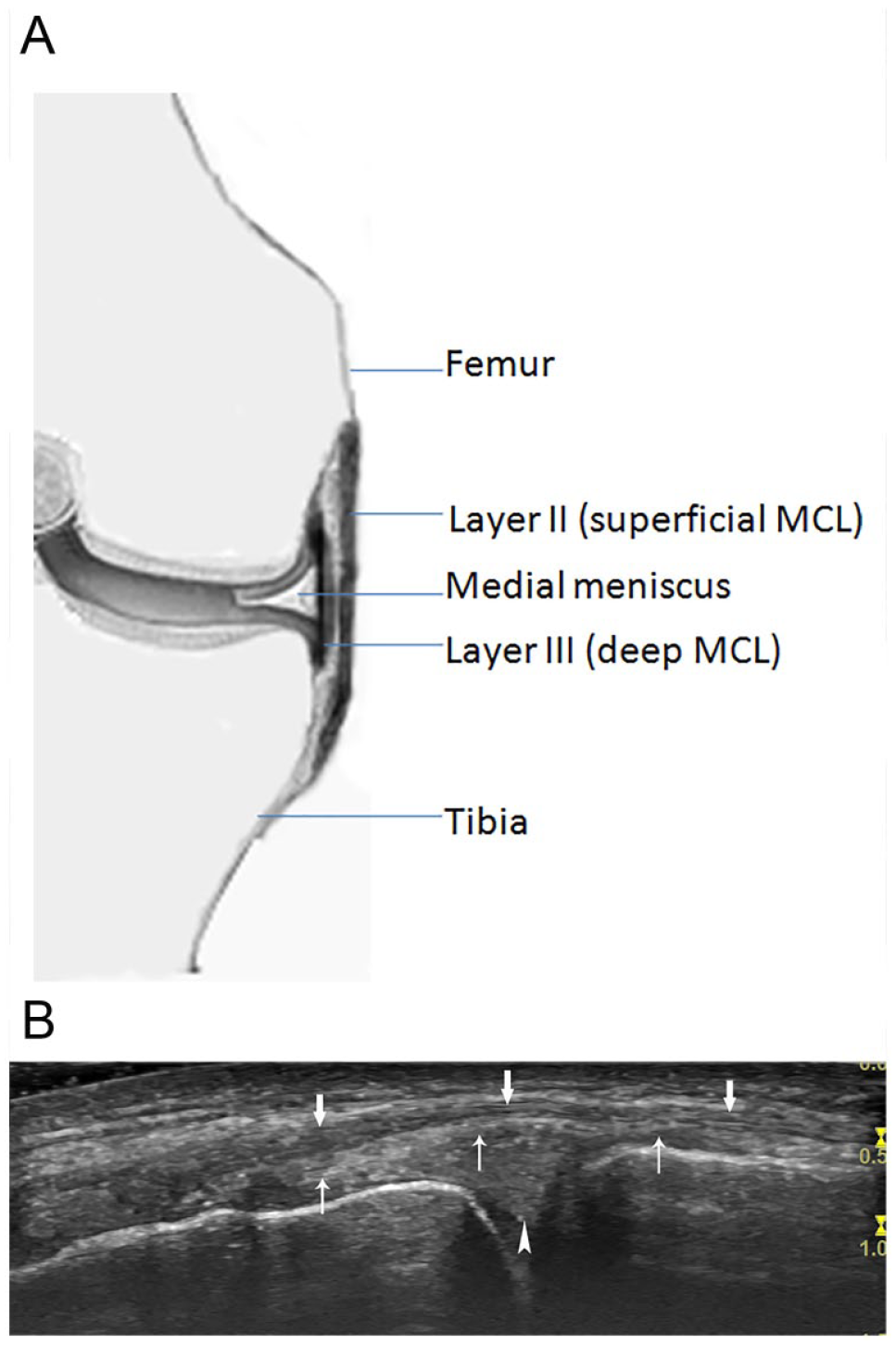
Coronal view of the medial structures of the knee. (A) Diagram of the superficial and deep portions of the MCL and the medial meniscus. (B) Sonography of the superficial portion (arrows) of the MCL, the deep portion (thin arrows) of the MCL, and the medial meniscus (arrowhead). MCL, medial collateral ligament.
Case 1
A 32-year-old man was referred for a sonographic examination due to persistent pain in the left medial knee. Three months prior, he fell off his snowboard while boarding down a steep hill. He felt sharp pain in the left medial knee. Later, the medial knee became swollen and tender. Rest and ice was applied locally, but the pain did not improve significantly in the medial aspect of the knee. Despite one session of physiotherapy, the pain still bothered him when walking. He also felt instability of the left knee. He did report having chronic bilateral knees pain over the last 3 years, due to prior injuries. Physical examination revealed mild swelling and palpable tenderness in the left medial knee without any focal skin color changes. A left knee radiograph was interpreted as normal.
A systematic sonogram of the left knee was performed with a linear high-frequency transducer (6–15 MHz) using the GE (General Electric) LOGIQ S8 ultrasound equipment (GE Ultrasound, Waukesha, Wisconsin). The sonographic scanning protocol followed the “Musculoskeletal ultrasound technical guidelines” issued by the European Society of Musculoskeletal Radiology. On the coronal imaging of the medial knee, an anechoic area (0.8 × 0.2) was found in the medial parameniscal region between the meniscus and the deep portion of the MCL. The superficial edge of the meniscus was unsmooth (Figure 2A). A vertical hypoechoic cleft could be seen from the superficial surface of the meniscus toward the deep joint (Figure 2B). The proximal deep layer of MCL (meniscofemoral ligament) had a hypoechoic interruption (Figure 2B), which connected to the anechoic area between the deep layer of middle MCL and the meniscus. No other imaging abnormality was found in the knee.
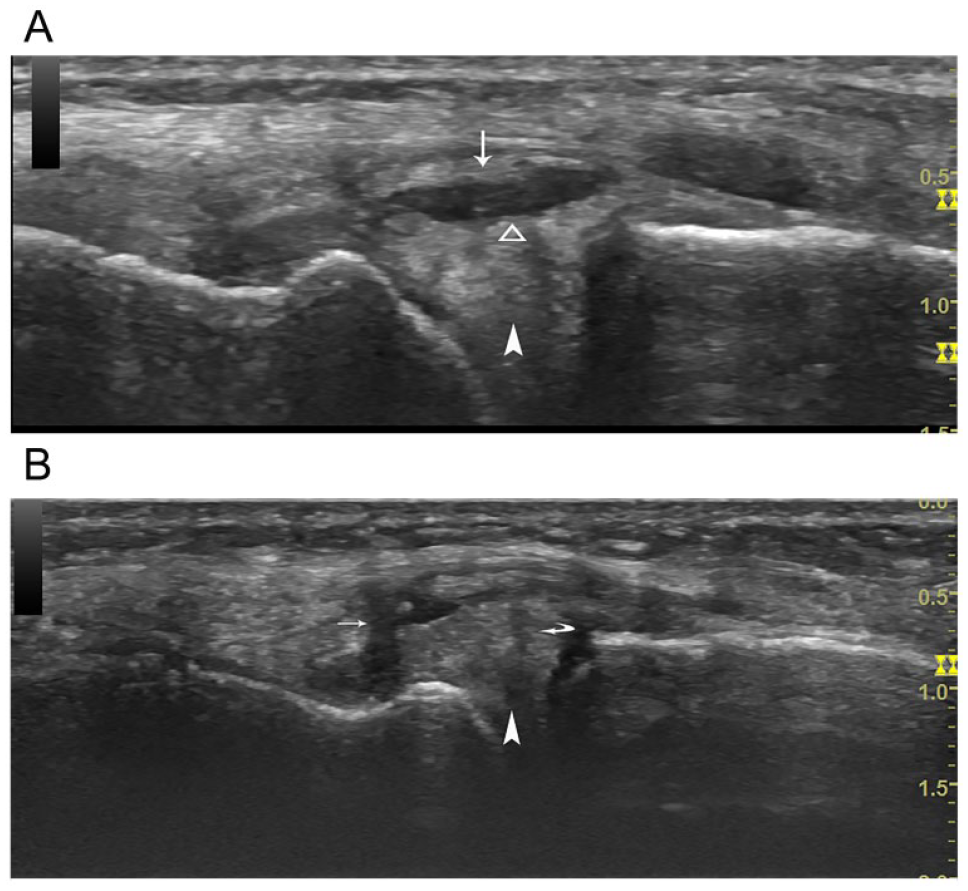
Case 1 coronal view of the left knee. (A) An anechoic area represents fluid collection between the deep portion of the MCL (thin arrow) and the meniscus (arrowhead). The superficial edge of the meniscus is unsmooth (triangle frame). (B) A vertical hypoechoic cleft (curved arrow) in the meniscus represents a meniscal tear. A hypoechoic interruption (thin arrow) in the proximal meniscofemoral ligament represents a tear in the deep portion of the MCL. MCL, medial collateral ligament.
A follow-up examination was done by the patient’s general practitioner. Four and half months after his sonogram, this patient had an MRI examination. The report indicated a meniscal tear starting from the medial posterior horn and spanning a length of 2.7 cm, and a small collection of fluid superficial to the medial meniscus. A parameniscal cyst could not be excluded. No MCL abnormality was found. Later, this patient had left knee surgery. The post-surgical diagnosis was medial MCS with meniscal tear.
Case 2
A 37-year-old man came for a follow-up sonographic examination of the left knee. He claimed that the left medial knee was still painful and he required a cane for ambulation. One month prior, his left knee was severely twisted, during a baseball game. The whole knee was swollen after the injury, especially the medial aspect. Pain and tenderness were also mainly in the medial aspect of the left knee. He saw a general practitioner the next day after his injury and was referred for the left knee imaging. Left knee three view radiograph demonstrated no abnormality of the bones and joints. Sonography showed a hypoechoic area superficial to the medial meniscus. MCL partial tear was also suspected. The reading radiologist suggested a follow-up sonogram if the left knee pain does not improve. The patient did not seek professional treatment but took nonsteroidal anti-inflammatory drugs to relieve pain. He had no other recognized left knee injury prior. Physical examination revealed mild swelling and palpable tenderness to the medial aspect of the left knee. No other abnormality was noted as part of that examination.
The sonographic equipment and scanning protocol used were the same as that used in the first patient case. On the sagittal image of the suprapatellar region of the left knee, mild effusion was identified. On coronal image of the medial knee, an anechoic area (0.9 × 0.14) could be seen in the medial parameniscal region between the meniscus and the deep portion of the MCL. The superficial edge of the meniscus was unsmooth (Figure 3A). A vertical hypoechoic cleft was also identified in the medial meniscus (Figure 3B). The proximal MCL appeared more hypoechoic, and thicker than the one in the contralateral knee (Figure 3C and D). No other abnormality of the left knee was found. An MRI examination was suggested by the reading radiologist, to verify the sonographic findings.
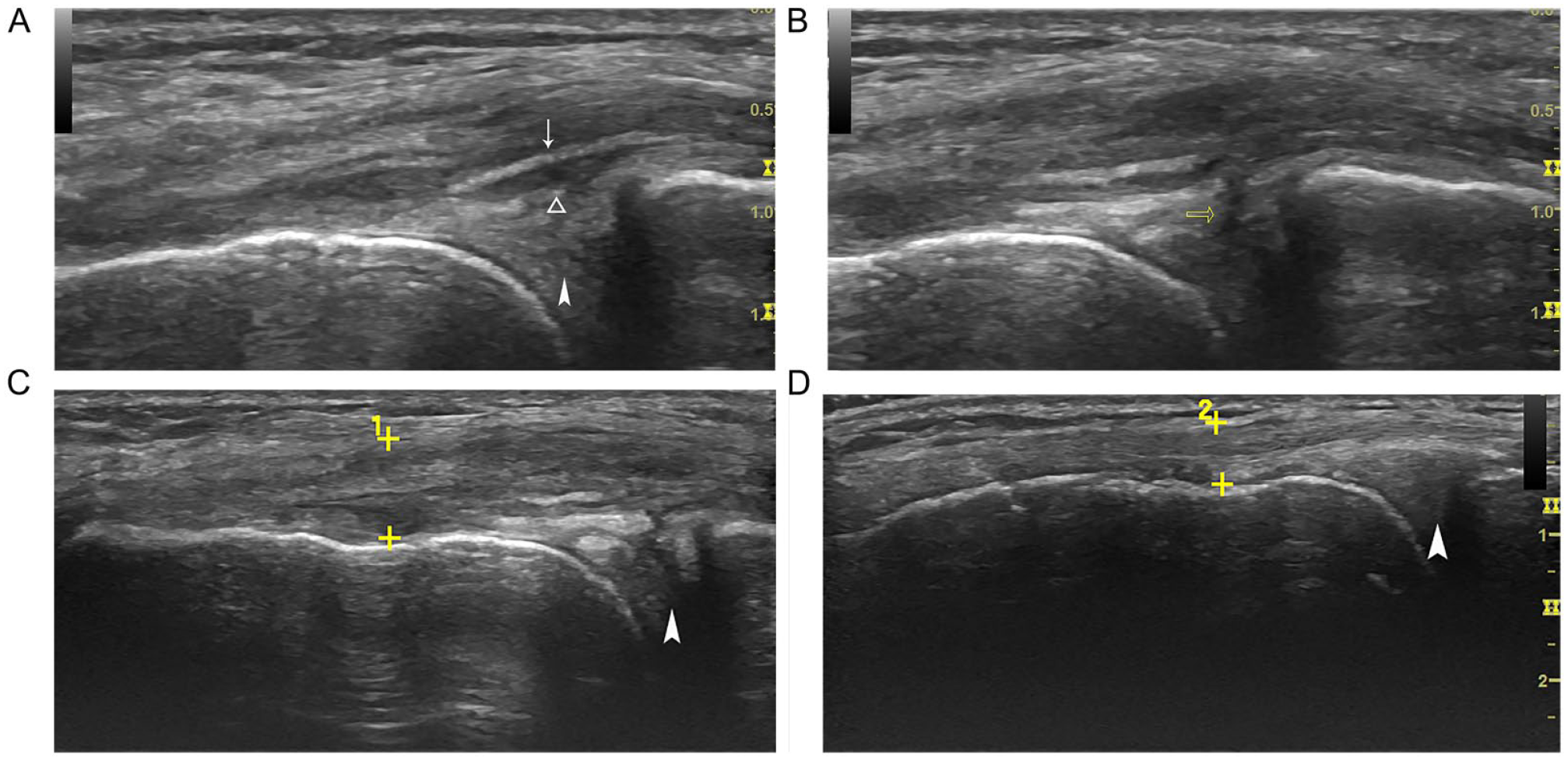
Case 2 coronal view of the left knee. (A) An anechoic area represents fluid collection between the deep portion of the MCL (thin arrow) and the meniscus (arrowhead). The superficial edge of the meniscus is unsmooth (triangle frame). (B) A vertical hypoechoic cleft (empty arrow) in the meniscus represents a meniscal tear. (C) The proximal MCL appears more hypoechoic, and thicker (between the two calipers, 0.67) than the one (between the two calipers, 0.42) in the contralateral knee (D). MCL, medial collateral ligament.
A follow-up was done through his general practitioner. Three months after the sonogram, this patient had an MRI examination. The findings were similar to the sonogram, except no proximal MCL pathology. The MRI was interpreted as left knee medial MCS and meniscal tear.
Discussion
MCS is a tear of the knee capsule from its junction with the meniscus. It is usually found in young athletes with sports-related injury to the knees. The above two patients both were in their 30s and had sports-related knee injuries. They both presented with medial knee pain, swelling and palpable tenderness. However, like other medial knee pathologies, these symptoms and signs are nonspecific. Therefore, the diagnosis of MCS has to depend on imaging modalities.
Imaging diagnosis of MCS was first reported by using MRI, but the positive predictive value was very low (less than 10%). 3 Later, more MRI research on MCS was done, and diagnostic criteria for MCS were proposed.1,4–6 For medial MCS, the main MRI signs for diagnosis are the presence of perimeniscal fluid and an irregular meniscal outline. Meniscal inward displacement can also be seen.1,4 However, a retrospective study of six consecutive patients with arthroscopically confirmed medial MCS between 2007 and 2009 found that MRI did not identify the pathologies in any of them. 7
Sonography has been widely applied to the diagnosis of knee abnormalities. The medial capsuloligamentous complex and the peripheral middle third of the medial meniscus are relatively superficial in the medial knee. A high-frequency linear transducer is suitable to detect pathologies in these structures, such as MCL injury, MCL bursitis, meniscal peripheral tear, or meniscal cysts.9,13 The sonographic findings of the medial knees from both of the patients above had similar features: an anechoic area representing a fluid collection was seen in the medial parameniscal region between the meniscus and the deep portion of the MCL; and the superficial surface of the medial meniscus was unsmooth. These features match the MRI diagnostic criteria of medial MCS.1,4 Furthermore, the post-surgical diagnosis in the first case and the MRI diagnosis in second support the sonographic diagnosis of medial MCS. Isolated MCS is uncommon, and the associated injury may involve the deep portion of MCL (meniscofemoral and meniscotibial ligaments) or the peripheral portion of the medial meniscus. 1 The deep portion of the proximal MCL (meniscofemoral) is more commonly involved in this injury. In severe situations, the coexistence of a meniscal or anterior cruciate ligament tear is possible. 12 In case 1, the hypoechoic interruption of the deep portion of the proximal MCL representing the meniscofemoral ligament tear was detected. In case 2, the hypoechoic and thicker proximal MCL representing ligament strain was identified. In both cases, the vertical hypoechoic cleft in the medial meniscus representing a meniscal tear was detected. MRI did not find the meniscofemoral ligament tear in the first case or the MCL strain in the second case. The reason may be that by the time the two patients had their MRI examinations, it had been 4 to 5 months after the injuries, and the MCL tear or strain might have healed. For the current sonographic cases presented, MRI diagnosed one and misdiagnosed the other. This suggests that MRI may not be as effective as sonography in diagnosing medial MCS, as a previous report has concluded. 9
Based on the analysis of the clinical findings, sonographic characteristics, and post-surgical and MRI reports, sonographic diagnosis criteria of medial MCS are proposed: (1) patient has a history of sports-related medial knee trauma; (2) affected medial knee has focal pain, swelling, and tender; (3) ultrasound of the medial knee demonstrates fluid collection between the medial meniscus and the deep portion of the MCL, and an unsmooth surface of the meniscus; (4) MCL injury (strain or meniscofemoral ligament tear) and/or meniscal tear are supportive signs for assessment of the severity of the trauma.
Fluid collection between the medial meniscus and the deep portion of MCL is a critical sonographic sign of medial MCS. However, in the situations of a special MCL bursitis or medial meniscal cyst, similar appearances may also be seen. Therefore, these pathologies need to be carefully differentiated.
Meniscal cysts are common disorders of the knee. A meniscal cyst is a collection of fluid found adjacent to the meniscus. One consensus theory about the formation of a meniscal cyst is that it is developed from the collection of the synovial fluid through a tear in the articular surface of the meniscus.12,14 Hence, a meniscal tear can often be found connected to a meniscal cyst during sonography. The shape of a meniscal cyst may be unilobular or multilobular. The location of the medial meniscal cyst may be adjacent to the meniscus or develop at some distance through a pedicle from the meniscus because of the restriction of the MCL. 12 If a unilobular meniscal cyst occurs in the middle third of the medial meniscus, it is an important pathology to consider in the differential. The following sonographic characteristics may help to differentiate a meniscal cyst from a medial MCS. A medial meniscal cyst tends to be round and may not be horizontal to the meniscus or parallel to the MCL. There is no clear separation between the deep portion of the MCL and the medial meniscus. The shape of a meniscal cyst does not change with knee movement or with applied pressure, while the shape of a fluid collection of MCS may change.13,14 Other important clinical factors are that most patients with meniscal cysts are asymptomatic and have no history of sports injury.
As we mentioned earlier, the MCL bursa is located between the two layers (portions) of the MCL ligament. The bursa is often separated into femoral and tibial compartments. 13 The femoral compartment is located superiorly and adjacent to the femoral cortex, whereas the tibial one is located inferiorly and adjacent to the tibial cortex. There is another type of MCL bursa, which spans the joint from the femoral compartment to the tibial compartment. Normally MCL bursa cannot be visualized with sonography or MRI. The distension of fluid in the MCL bursa is usually a sign of bursitis caused by inflammation of the bursa. If the bursa spanning the joint is small and limited to the parameniscal region, it may appear as a fluid collection similar to medial MCS. A feature of MCL bursitis is that it has a smooth inner border on sonography, and usually no meniscal tear could be found. 13 Clinically, some patients may have symptoms while some may not, and again, there is usually no history of sports-related trauma.
Conclusion
The diagnostic criteria of the medial MCS were proposed based on the study of the above two patient case reports. The most important sonographic signs are fluid collection between the medial meniscus and the deep portion of the MCL, and an unsmooth surface of the meniscus. Sonography may be more effective in diagnostic accuracy of a medial MCS than MRI.