
Abstract
The bursitis of the medial collateral ligament (MCL) of the knee is the inflammatory distension of the bursa located between the superficial and deep portions of MCL. Five cases with sonographic findings of suspected MCL bursitis were reviewed. All five cases had fluid collection with distinct and smooth borders between the superficial and deep portions of the MCL. Two of them had the fluid adjacent to the tibia; two of them adjacent to the femur; and one of them spanning the joint. Four of the five patients without recognizable knee injury history and middle third meniscal tear excluded the possibility of injury-related fluid collection. Hence, MCL bursitis is the possible diagnosis. One young adult with a recent knee injury also had a tear in the meniscofemoral ligament of the deep portion of the MCL. The distension of the bursa was interrupted by and directly connected to the tear of the meniscofemoral ligament. Therefore, it is part of the injury but not bursitis. This report describes sonographic characteristics of MCL bursitis that may assist in the diagnosis and differentiate it from other medial knee conditions.
Introduction
Distension of the medial collateral ligament (MCL) bursa of the knee is uncommon. Only 0.1% of magnetic resonance imaging (MRI) of the knee was reported as this pathologic finding. 1 Medial collateral ligament bursitis is the inflammatory distension of the bursa located in the medial knee. Other conditions such as meniscocapsular separation and medial capsuloligamentous injury may also cause distension of the bursa.2,3 Therefore, differentiating the inflammatory condition of the bursa from other conditions is important to guide clinical treatment. Although multiple studies have described diagnosis of MCL bursitis via clinical evaluation and MRI,1,2,4,5 sonographic study is rarely reported. Sonographic detection of the MCL and its related lesion is a well-established diagnostic technique. Low-cost and dynamic scanning are the major advantages of sonography over MRI. The purpose of this study was to investigate the sonographic characteristics of MCL bursitis to assist in the diagnosis and differentiation from other medial knee conditions. Five cases with sonographic findings of distension of the bursa were analyzed, and the tentative sonographic feature of MCL bursitis was deduced. To promote better understanding of this work, bursa anatomy is reviewed, as part of the study.
The MCL of the knee, also known as the tibial collateral ligament (TCL), is the largest and main supporting structure of the medial aspect of the knee. It is part of the medial capsuloligamentous complex, which is composed of three layers.6,7 Layer 1 is the superficial layer, consisting of the deep fascia from the continuity of the fascia overlying the vastus medialis anteriorly and the sartorius posteriorly. Layer 2 is the intermediate layer, which is the superficial portion of the MCL (Figures 1A, 2A). It is a strong, flat, and straight vertical fibrous band in the middle third of the knee with one proximal femoral attachment and two distal tibial attachments. The femoral attachment is located posterior to the medial epicondyle about 5 cm superior to the joint line. 8 The tibial attachments include the proximal one mainly attached to the anterior arm of the semimembranosus tendon and the distal one located just anterior to the posteromedial crest of the tibia within the pes anserine bursa. The distal one is about 6 to 7 cm inferior to the joint line. The superficial portion of the MCL measures 10 to 11 cm in length and 1.5 cm in width.7,8 Layer 3 is the deep layer, which is a thickening of the medial joint capsule. It is the deep portion of the MCL, interlacing with the medial meniscus and attaching superiorly and inferiorly to the articular margins of the joint to form the meniscofemoral and meniscotibial ligaments.6,8 The meniscofemoral ligament is longer in the proximal-to-distal direction than the meniscotibial ligament (Figure 1B), whereas the latter is thicker and attached just distal to the edge of the articular cartilage of the medial tibial plateau. 7 Layers 1 and 2 (superficial portion of the MCL) fuse anteriorly to form the medial patellar retinaculum. 9 The superfacial portion of the MCL does not fuse with the deep portion of the MCL anteriorly but joins the deep portion in the posterior third of the medial side of the knee to form the posterior oblique ligament, which is closely attached to the posteromedial meniscus. 9 The function of the MCL is to go against valgus stress and abnormal external rotation of the knee.
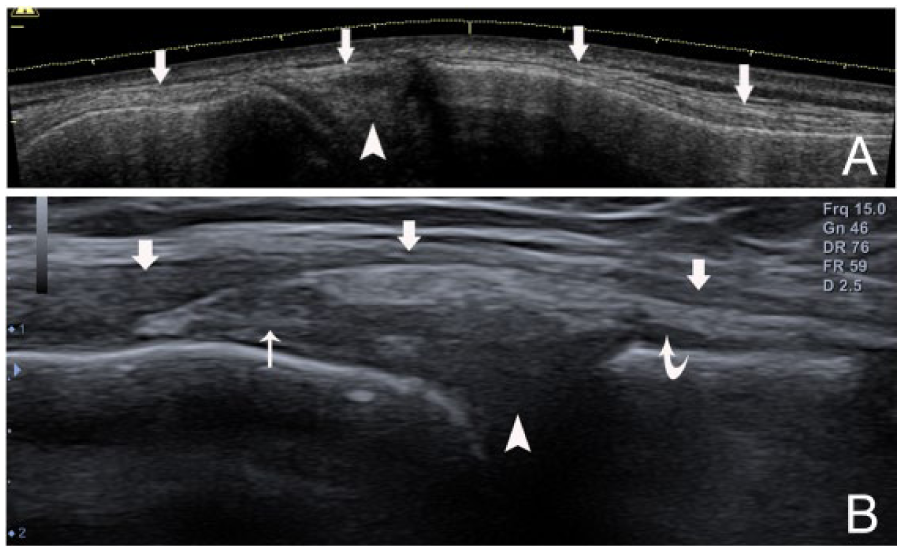
Sonographic anatomy of the medial collateral ligament (MCL). (A) Panoramic coronal view of the MCL (arrows) and the medial meniscus (arrowhead). (B) Coronal view of the MCL structure: the thin superficial portion of the MCL (arrows), the thick deep portion of the MCL and its proximal meniscofemoral ligament (thin arrow), and its distal meniscotibial ligament (curved arrow). The medial meniscus (arrowhead) is deep to the deep portion of the MCL.
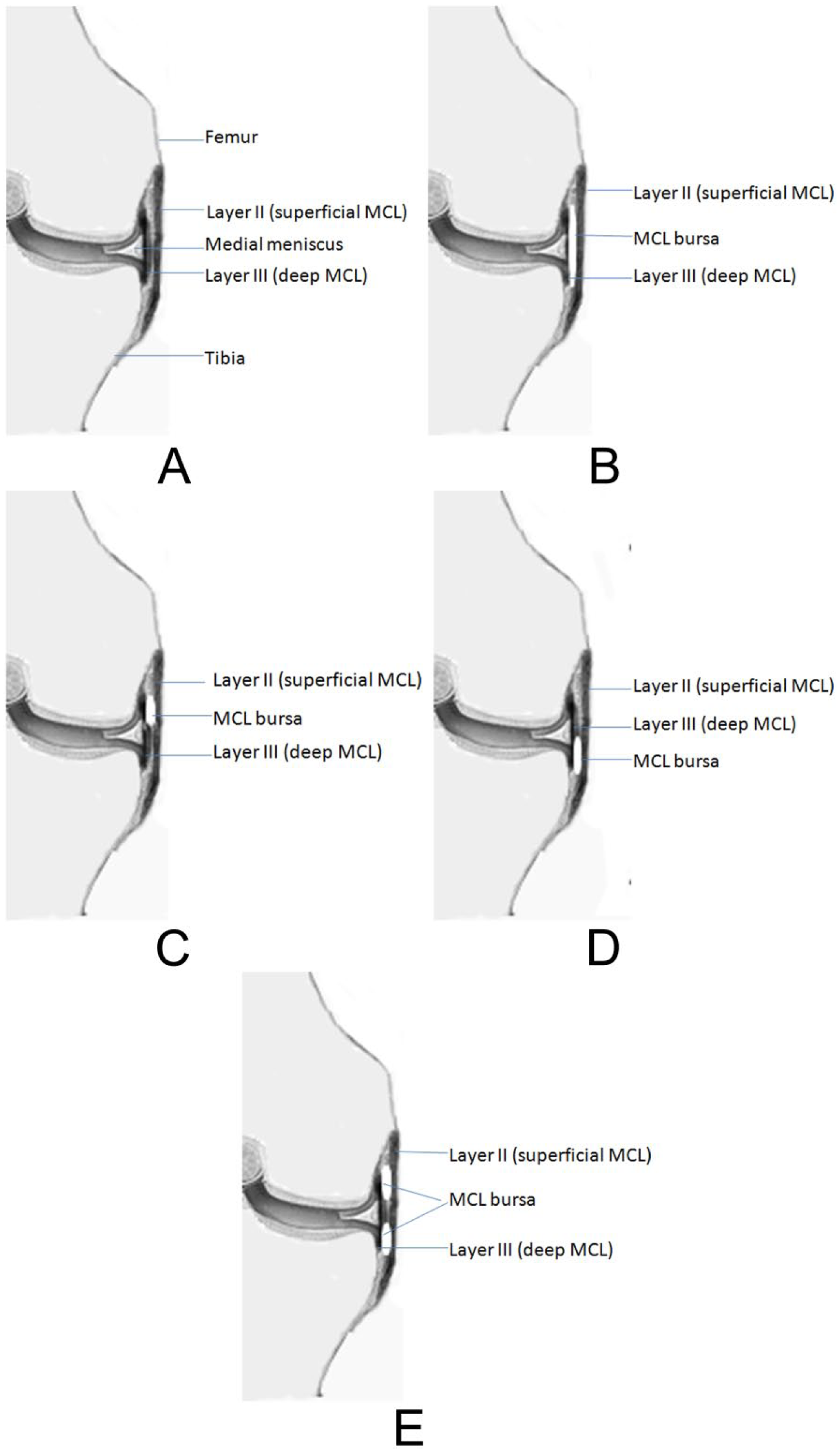
Coronal view of the medial structures of the knee. (A) Superficial and deep portions of the medial collateral ligament (MCL). (B) MCL bursa between the superficial and deep portions of the MCL spanning the joint from the femoral aspect to the tibial aspect. (C) MCL bursa with only the femoral compartment. (D) MCL bursa with only the tibial compartment. (E) MCL bursa consisting of two separate compartments: the femoral compartment and the tibial compartment.
Between the superficial and deep portions of the MCL, a bursa is located along the middle third of the medial knee. When the knee is in flexion, the bursa allows the MCL to glide over the bony surfaces of the tibia and femur without friction. Bursal sacs were first reported with five different locations deep to the MCL by Brantigan and Voshell. 10 Later, the detailed anatomy of the bursa with MRI, in patients and cadavers, was reported. 1 Its anterior margin is adjacent to the anterior edge of the superficial layer, whereas the posterior margin is outlined by the junction of the superficial and deep portions of the MCL. 1 The bursa is often separated into femoral and tibial compartments (Figures 2B, 2C, 2D, 2E). The femoral compartment is superiorly located adjacent to the femoral cortex, whereas the tibial one is inferiorly located adjacent to the tibial cortex. The bursa presenting in only the femoral compartment is frequently seen, and the next is the tibial compartment only. Having both separate femoral and tibial compartments, or having one bursa spanning the joint without separation between the femoral and tibial compartments, is less common. 1
Patients and Methods
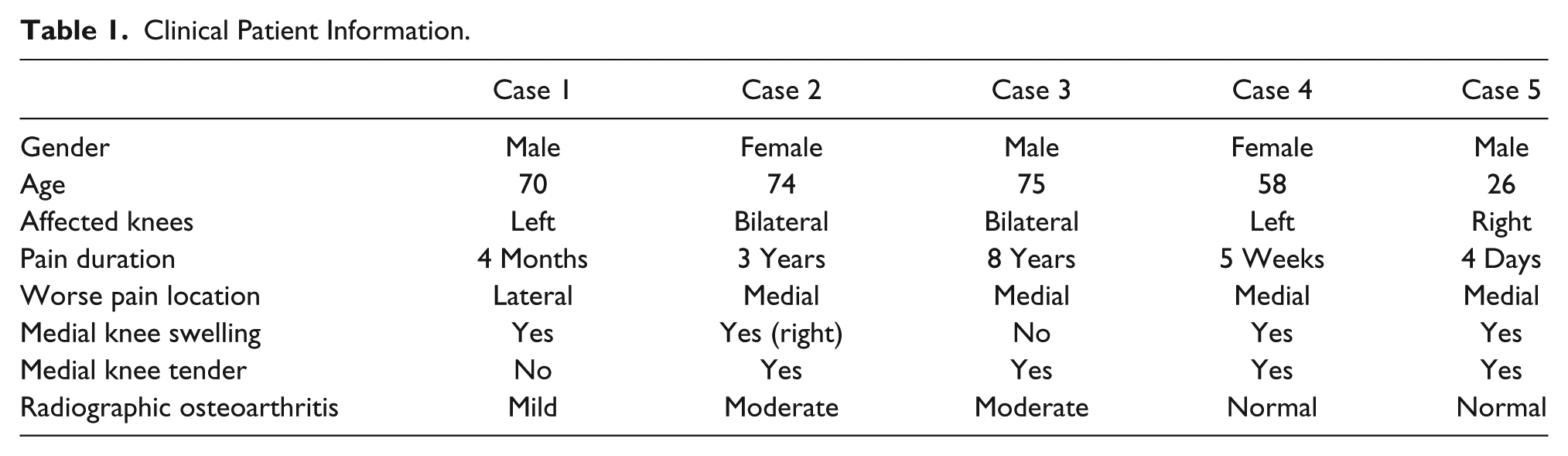
Five cases with sonographic findings of suspected MCL bursitis were reviewed. Four patients had no recognizable knee injury history; they included two male and two female patients, ranging in age from 58 to 75 years. Two of them had bilateral knee pain and two had only left knee pain. The pain had lasted from 5 weeks to 8 years. None of them had a history of gout, rheumatoid, or other systematic disease related to a knee disorder. Physical examination revealed mild swelling in the medial aspect of the knees for three of the patients. No skin color change was noticed in the area of swelling. Tenderness in the swollen area was identified in three of them. Routine knee radiographs diagnosed mild osteoarthritis in one patient, moderate osteoarthritis in two patients, and one normal. The fifth patient was a 26-year-old male. He had a right medial knee injury that occurred during a soccer game, 4 days before being referred for sonography. After the injury, the medial knee appeared swollen and painful. No local treatment was given to this patient. Medial knee tenderness was revealed in the swollen area, at the time of the physical examination. The diagnosis of the knee radiograph was normal. Table 1 summarizes the clinical information of the five patients.
Clinical Patient Information.
Sonograms of the patients were performed by the principal investigator with a linear high-frequency transducer of the Alpinion E-CUBE 9 ultrasound machine (Alpinion Medical Systems USA, Bothell, Washington) (8-17 MHz) at a frequency of 15 MHz, or high-frequency transducer of the GE Voluson 730 Pro ultrasound machine (GE Ultrasound, Waukesha, Wisconsin) (6-12 MHz) at a frequency of 11 (only case 4 was scanned with this transducer). Two of the patients had bilateral knee sonography, and three of them had sonography of the complained knee as requested.
For examination of the knee, the anterior aspect including the suprapatellar and the patellar region was scanned first, followed by the medial, lateral, and posterior aspects. The specific protocol followed the musculoskeletal protocol outlined by the European Society of Musculoskeletal Radiology. In the suprapatellar area, if suprapatellar synovial recess effusion was identified, 3D measurement of the fluid collection was recorded. For medial knee scanning, the leg was in the position with 20 to 30 degrees of knee flexion. The transducer was placed in an obliquely oriented plane over the long axis of the MCL to obtain coronal images. Dynamic scanning started from the proximal end of the MCL and gradually moved to the distal end, covering the entire length of the ligament. Sonographically, the MCL appears as a hyperechoic band with two layers representing the superficial and deep portions of the ligament separated by slight hypoechoic fatty tissue (Figure 1). 8 Its echotexture and thickness were compared with the correspondent MCL in the other knee when any abnormality was suspected, especially the proximal deep portion of the ligament, where an MCL tear commonly occurs. If an anechoic area between the superficial and deep portions of the MCL was identified, its specific location relative to the joint was noted, such as superior or inferior to the joint (or adjacent to the femoral condyle or tibial plateau), and 3D measurements were made. Color Doppler was used to determine whether the anechoic area was fluid or a vascular lumen. The medial meniscus was imaged coronally with the probe perpendicular to its base, whereas the femoral condyle and tibia plateau were imaged. Sonographically, the medial meniscus appears as a triangular hyperechoic structure located in the center of the femorotibial joint. Its base is located superficially with the margin running continuous with the deep portion of the MCL. Its apex points toward the deep joint, which is difficult to observe. 8 If the medial meniscus had external displacement (extrusion), the displacement was recorded by measuring the distance from the outermost edge of the meniscus to a line connecting the femoral condyle and tibial plateau cortices. 11 To determine how much meniscus was extruded, another measurement of the longest superior to inferior edge of the meniscus outside the joint was recorded. The area of the extruded meniscus was calculated by multiplying the two measurements. During the evaluation of the posterior knee or the popliteal fossa, a Baker cyst, located between the medial head of the gastrocnemius and the semimembranosus tendon in the medial aspect of the fossa, required a 3D measurement. Color Doppler was also used to exclude focal vascular enlargement or presence of an aneurysm.
Results
Suprapatellar effusion was identified in all of the knees examined from the five patients. All scanned knees of the three patients older than 70 years displayed medial meniscal extrusion, the overlying superficial portion of the MCL bowing, and the joint narrowing. Prominent osteophytic spurs from both the femur and the tibia at the medial aspect of the joint could be seen (Figures 3A, 3B, 3C). All five cases had fluid collection between the superficial portion and the deep portions of the MCL (Figures 4, 5, 6, 7, 8A, 8B). Two of them had fluid collection inferior to the joint and adjacent to the tibia (Figures 4, 5), two of them had fluid collection superior to the joint and adjacent to the femur (Figures 6, 8A, 8B), and one of them had fluid collection spanning the joint from superior to inferior and adjacent to the femur and the tibia (Figure 7). The fluid collection in all of the cases had distinct and smooth borders. No meniscal tears, in the middle third, were identified in any of the five patients. The four patients between ages 58 and 75 years showed no signs of sprain or tear of the MCL. However, the young patient with medial knee injury displayed a hypoechoic texture and remarkable thickening of the proximal MCL compared with the contralateral knee, implying ligament sprain (Figure 8C). The meniscofemoral ligament of the deep portion of the MCL had an obvious tear which reached the deep edge of the superficial portion of the MCL, dividing the fluid collection into proximal and distal parts (Figures 8A, 8D). Only one patient also had a Baker cyst in the popliteal fossa. Table 2 summarizes the sonographic findings of the five patients.
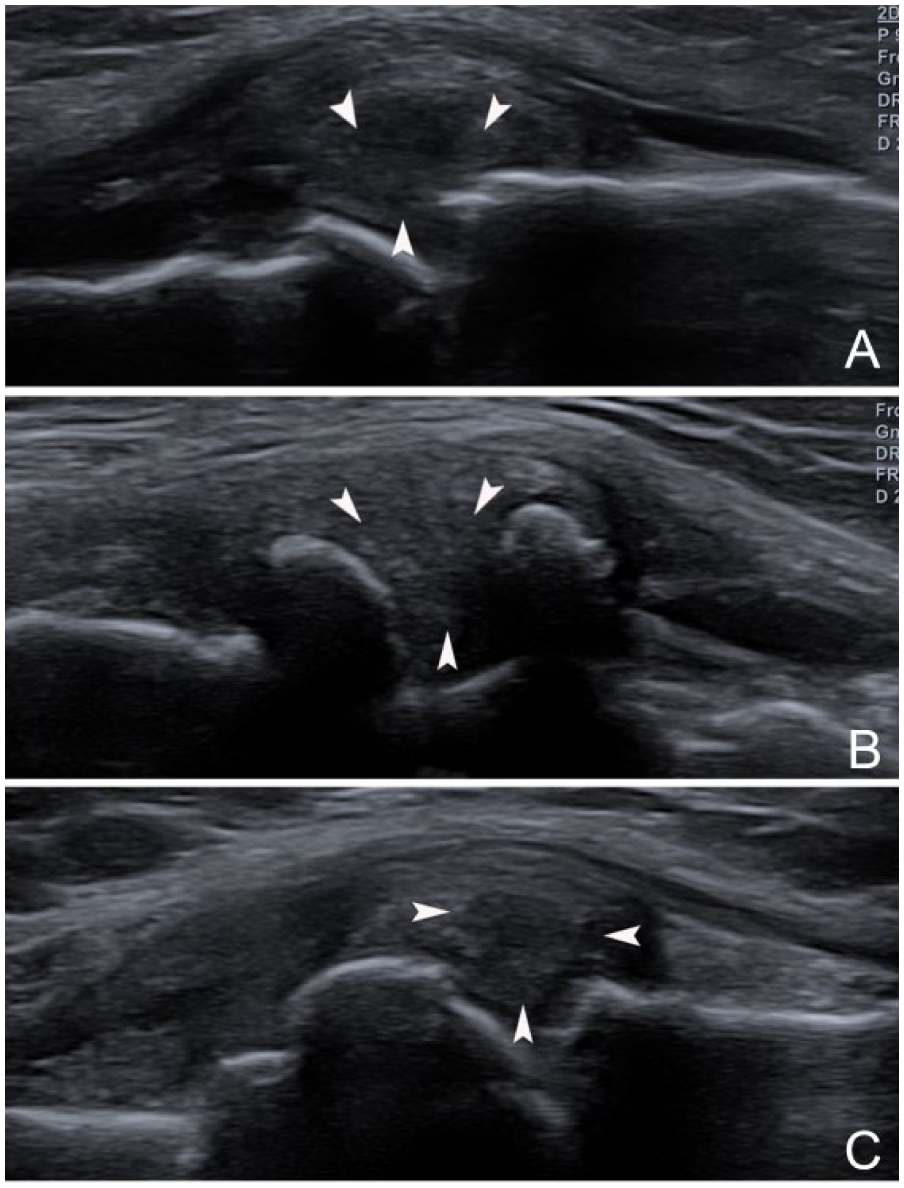
Extrusions of the medial menisci in coronal views. (A) Case 1. (B) Case 2. (C) Case 3. The extruded menisci (arrowheads), medial collateral ligament bowing, narrowed joint spaces, and osteophytes from the femurs and tibias can all be seen in these cases.
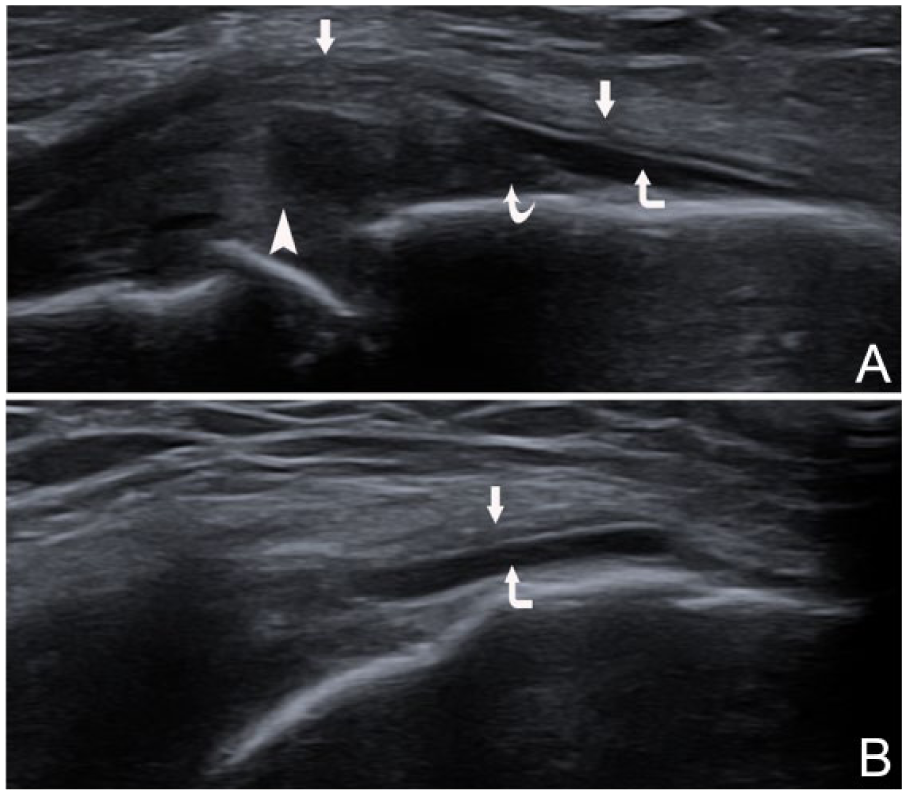
Case 1 medial collateral ligament (MCL) bursa distension. (A) Longitudinal coronal view of the bursa (corner arrow) between the superficial portion (arrows) bowed by the extruded meniscus (arrowhead) and the deep portion (meniscotibial ligament) (curved arrow) of the MCL. (B) Medial transverse view of the bursa.
Case 2 medial collateral ligament (MCL) bursa distension. (A) Longitudinal coronal view of the bursa (corner arrow) between the superficial portion (arrows) bowed by the extruded meniscus (arrowhead) and the deep portion (meniscotibial ligament) (curved arrow) of the MCL. (B) Medial transverse view of the bursa.
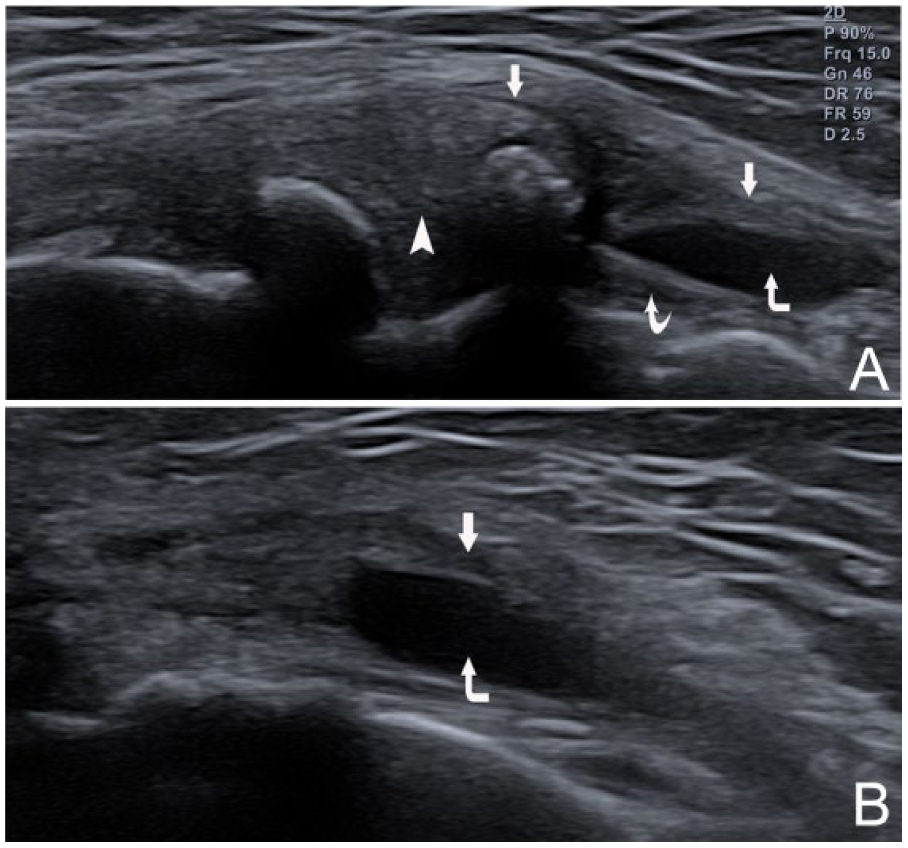
Case 3 medial collateral ligament (MCL) bursa distension. (A) Longitudinal coronal view of the bursa (corner arrow) between the superficial portion (arrows) bowed by the extruded meniscus (arrowhead) and the deep portion (meniscofemoral ligament) (thin arrow) of the MCL. (B) Medial transverse view of the bursa.
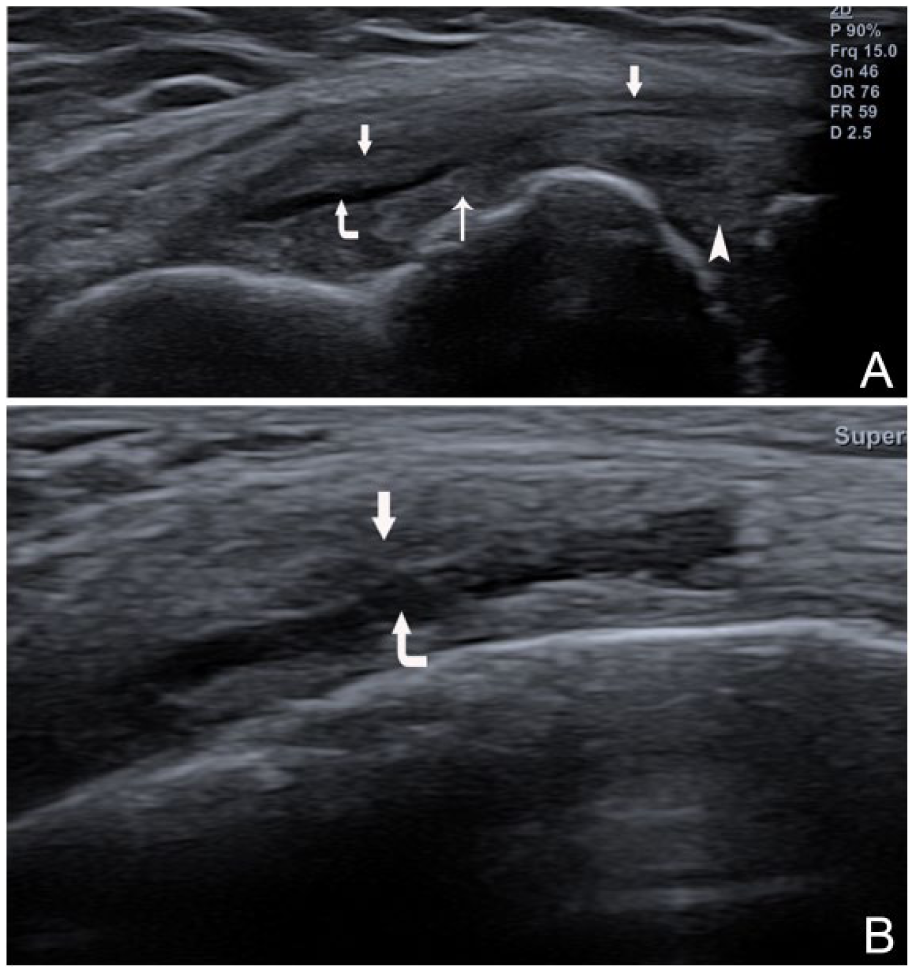
Case 4 medial collateral ligament (MCL) bursa distension. (A) Longitudinal coronal view of the bursa (corner arrow) between the superficial portion (arrow) and the deep portion of the MCL spanning the joint. Meniscotibial ligament (curved arrow), meniscofemoral ligament (thin arrow), meniscus (arrowhead). (B) Medial transverse view of the bursa.
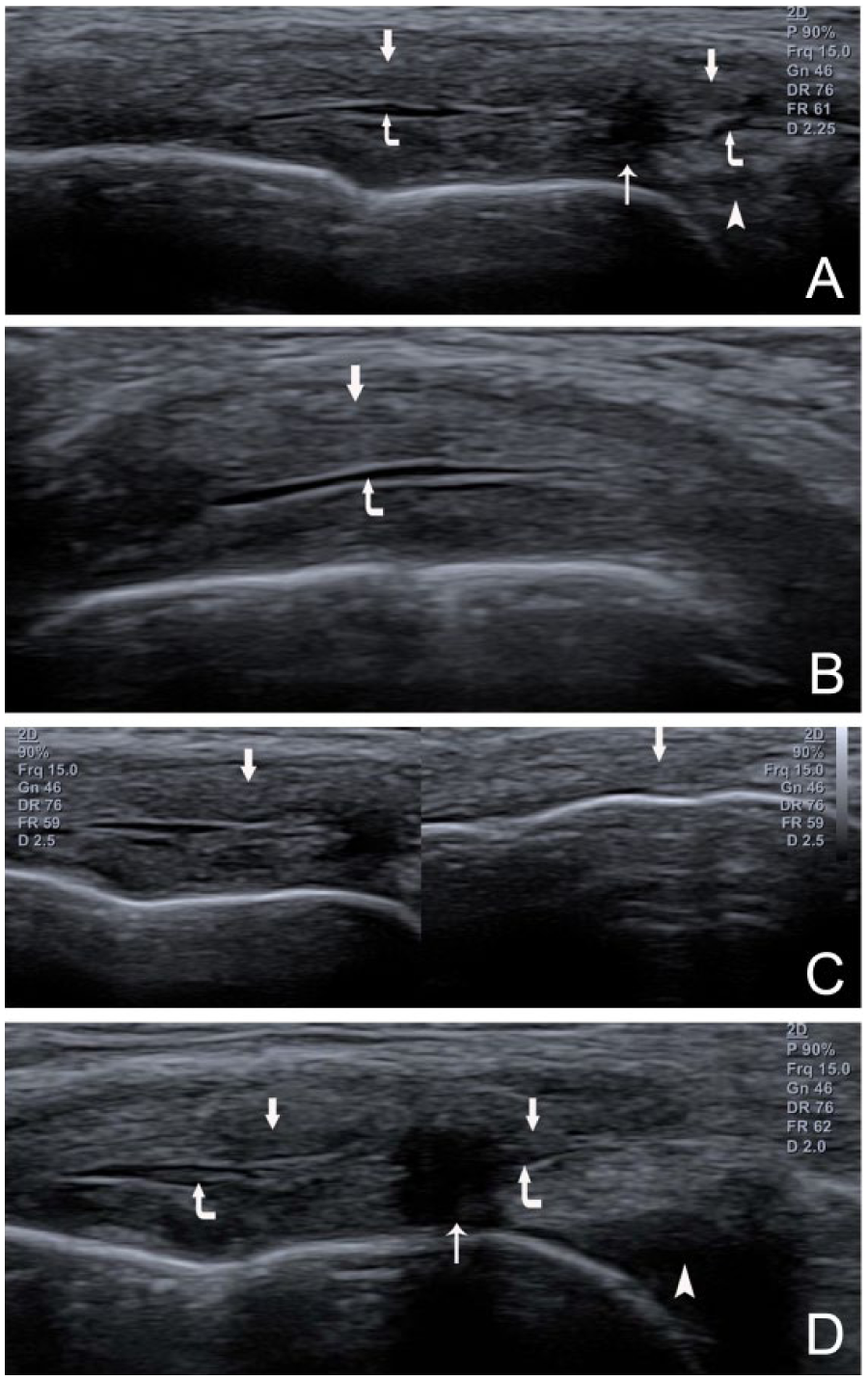
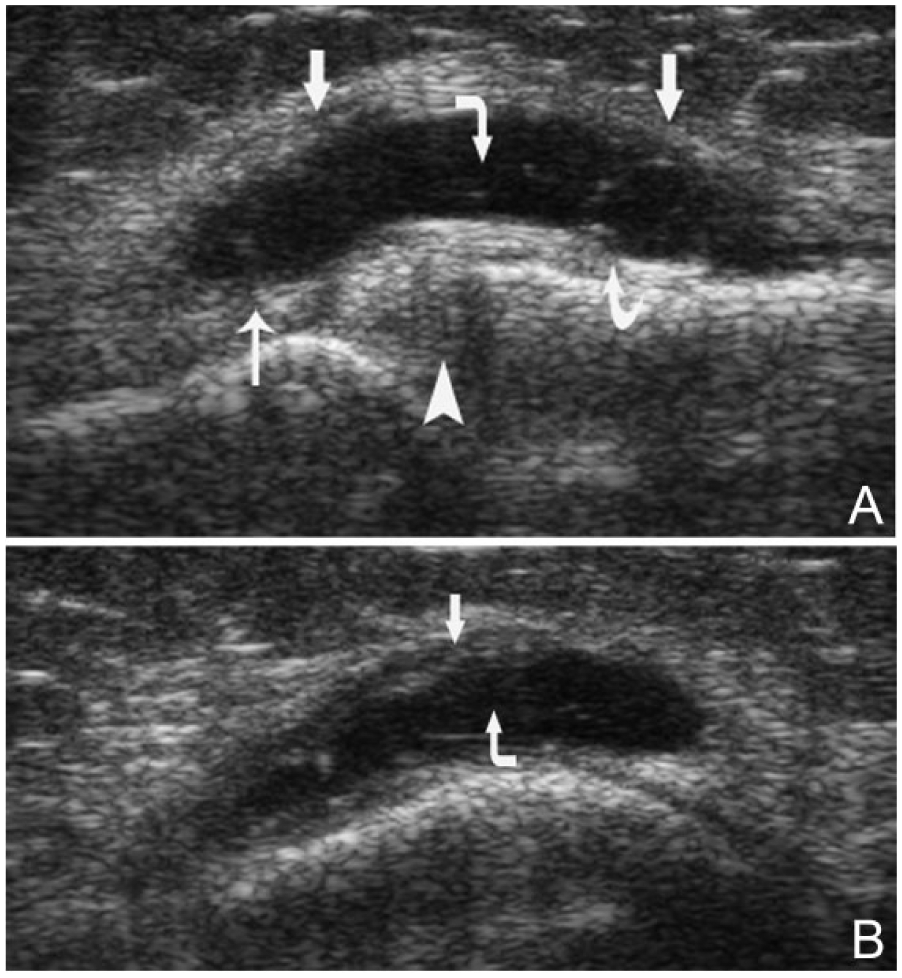
Case 5 medial collateral ligament (MCL) bursa distension. (A) Longitudinal coronal view of the bursa (corner arrow) between the superficial portion (arrow) and the torn deep portion (meniscofemoral ligament) (thin arrow) of the MCL. Meniscus (arrowhead). (B) Medial transverse view of the bursa. (C) Compared with the unaffected left knee, the right affected MCL (superficial and deep portions) (left panel) is much thicker and more hypoechoic (arrow) than the unaffected MCL (right panel). (D) The tear (thin arrow) of the proximal deep portion of the MCL (meniscofemoral ligament) reached the deep edge of the superficial portion. It divided the bursa into proximal and distal parts (corner arrows).
Sonographic Findings of the Patients. a
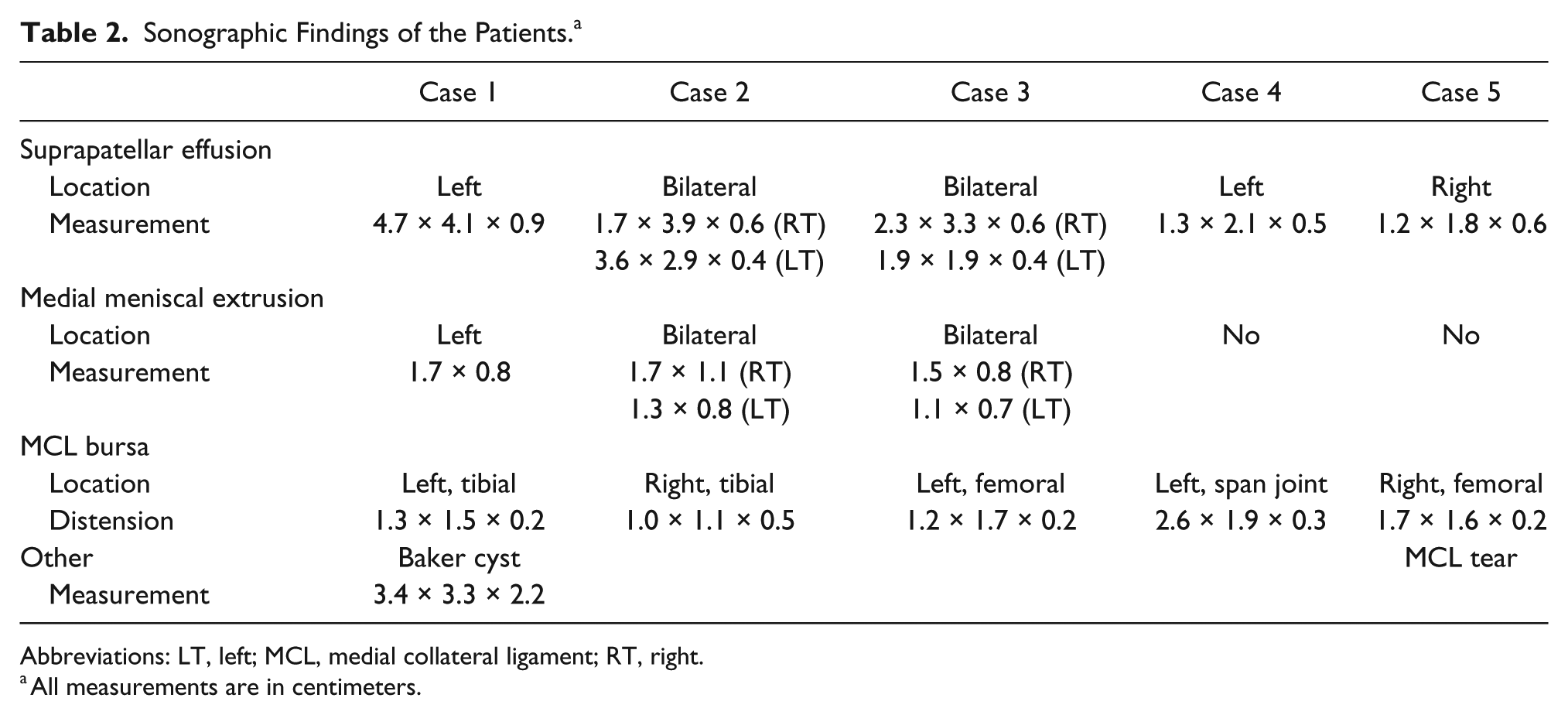
Abbreviations: LT, left; MCL, medial collateral ligament; RT, right.
All measurements are in centimeters.
Discussion
Bursitis is the inflammation of a bursa, which is lined with a synovial membrane that secretes synovial fluid. Medial collateral ligament bursitis is an uncommon disorder in knee pathology. 1 Kerlan and Glousman 4 first reported clinical diagnosis of MCL bursitis based on the findings of tenderness over the MCL at the joint line without a history of mechanical symptoms, such as locking or catching. The MRI diagnosis of MCL bursitis was established in 1991 and was based on documenting fluid distention in the bursa, an intact MCL, and lack of a medial meniscal tear. 2 Normally, the MCL bursa cannot be visualized on MRI or sonography. However, when it is distended with fluid, it can be seen as a well-defined fluid collection between the superficial portion and deep portion of the MCL.1,2,5 Distension of the bursa may suggest bursitis, but meniscocapsular separation or medial capsuloligamentous injury is also possible.2,3 In situations of meniscocapsular separation or medial capsuloligamentous injury, distension of the bursa may be related to local hemorrhage or synovial fluid leaking from the joint, secondary to a layer 3 rupture.2,3
Meniscocapsular separation is the detachment of the meniscus from its outer capsular attachment (middle part of the deep portion of the MCL). It is a tear of the capsule from its junction with the meniscus. 12 This injury is rare and usually found in young athletes due to a twisting injury of the knee. Isolated meniscocapsular separation is uncommon and the associated injury may involve the deep portion of the MCL (meniscofemoral and meniscotibial ligaments) or peripheral portion of the medial meniscus. 12 This type of injury is more common in the medial knee than in the lateral knee. The symptoms and signs are medial knee pain, swelling, and tenderness. The most important MRI factors for diagnosis of meniscocapsular separation are the presence of perimeniscal fluid and an irregular meniscal outline. Meniscal inward displacement can also be seen. 12 If there is a peripheral tear in the middle third of the medial meniscus, it is highly possible that the lesion can be detected with a high-frequency linear transducer. In addition, injuries of meniscofemoral and meniscotibial ligaments can also be detected.
Medial capsuloligamentous injury usually occurs in young adults participating in sports activities. The MCL is the most common structure involved in this injury. The majority of MCL injuries are isolated and affect the proximal MCL. 8 Partial thickness tears most commonly occur in the meniscofemoral ligament (part of layer 3). In severe situations, the coexistence of a meniscal or anterior cruciate ligament tear is possible. Radiating pain along the medial knee and local swelling are the clinical presentations, which, like other medial knee pathologies, are nonspecific. Sonography usually depicts a thickened and heterogeneous ligament. 8 In the case of a meniscofemoral ligament tear, fluid collection can be seen deep to the superficial portion of the proximal MCL. Most of the time, detachment of the meniscofemoral ligament can be visualized with sonography. The young study patient with a history of an acute knee injury had the above-mentioned meniscofemoral ligament tear and fluid collection. However, the fluid collection was interrupted by and directly connected to the tear of the meniscofemoral ligament. Its border was smooth and distinct, except for the interrupted segment. It may be the torn MCL bursa filled with either blood or fluid that leaked from the joint through the ruptured meniscofemoral ligament. In the situation of the tear of the superficial portion of the proximal MCL, fluid collections (hematoma) deep to the superficial portion of the MCL can also be seen, but the meniscofemoral ligament should be seen intact. 8 An important tip is that in the tear of the deep or superficial portion of the MCL, without involving the bursa, the fluid collection will have no distinct boundary.
In this study, all of the patients older than 50 years had no injury history. Therefore, the chance that the distension of bursa was caused by meniscocapsular separation or medial capsuloligamentous injury may be limited. The sonography of the fluid collection demonstrating a distinct and smooth border and the sonography of the middle third of the medial meniscus and the MCL revealing no tear provided further evidence to exclude the two entities.
Other pathologies that need to be considered are parameniscal recess effusion and meniscal cysts. The parameniscal recesses are the recesses on either side of the knee located superiorly and inferiorly to the meniscus, respectively. The recess is in contact with the femoral condyle superiorly and tibial condyle inferiorly on either side. It is more obvious on the lateral side of the knee. 13 Since the peripheral surfaces of the menisci themselves are not covered by the synovial membrane, no fluid in the recesses should be seen superficial to the menisci. With significant knee effusion, these recesses could be seen to extend superiorly and inferiorly, which may mimic a distended femoral compartment and tibial compartment of the bursa. However, the effusion in these recesses can be identified deep to the deep portion of the MCL (layer 3) and can be tracked to the joint deep to the medial meniscus. The fluid collections, in all five patients, were superficial to the deep portion of the MCL and the meniscus, therefore excluding the possibility of parameniscal recess effusion.
Meniscal cysts are common disorders of the knee. They often occur in the posterior horn of the medial meniscus. Thus, the cysts are located posteriorly with respect to the bursa.1,5,14 On the other hand, the cysts are between layer 1 and the conjoined layers 2 and 3, which is different from the location of the bursa. If a meniscal cyst occurs in the middle third of the medial meniscus, it is an important pathology to consider for differentiation. The shape of this medial meniscal cyst may be unilobular or multilobular. Its location may be adjacent to the meniscus or develop at some distance through a pedicle from the meniscus because of the restriction of the medial collateral ligament. 8 In either location, the cyst is deep to the superficial portion of the MCL. Furthermore, the border of a meniscal cyst may not be smooth and sharp. Such a meniscal cyst is usually directly connected to the meniscal tear, which can be sonographically seen as a hypoechoic cleft in the meniscus.5,14 In all five cases, no meniscal tear or direct connection of the fluid collection with the middle third of the medial meniscus was identified, and the borders of the fluid collections were distinct and smooth. Hence, they are not meniscal cysts.
This case series excluded the possibility of meniscocapsular separation and medial capsuloligamentous injury in four patients without injury history, as well as differentiated them from parameniscal recess effusion and meniscal cyst. Therefore, the fluid collections between the superficial and deep portions of the MCL in four of the patients should be distended MCL bursas, which implies MCL bursitis. Since the younger patient had a tear of the meniscofemoral ligament of the deep portion of the MCL after acute injury, the distended MCL bursa may contain blood or joint fluid. It is likely that this was not inflammation of the bursa but part of the injury. The sonographic characteristics that supported the diagnosis of MCL bursitis in this cohort were no acute injury history of the knee, especially the medial knee; a fluid collection with distinct and smooth borders between the superficial portion and deep portion of the MCL; no meniscal tear at the middle third of the medial meniscus; and no tear of the MCL (deep or superficial portion). In this cohort, a fluid distended bursa was at either of the following locations: adjacent to the femur (femoral compartment), adjacent to the tibia (tibial compartment), or spanning from femur to tibia over the medial joint. The symptoms and signs of bursitis, included pain and swelling in the medial aspect of the knee and tenderness around the medial joint line.1,4,15 It is important to note that these findings at the medial joint are commonly seen in meniscal disorders and MCL injury 8 ; therefore, they are nonspecific to MCL bursitis. Conversely, some patients with MCL bursitis may have a lack of medial joint symptoms and signs. 1 In this study, four cases of MCL bursitis, without injury history, had inconsistent pain location. One patient had no swelling in the medial knee, whereas another had no focal tenderness. Thus, diagnosis based only on the clinical findings without imaging evidence may be unreliable. Joint effusion and a Baker cyst found in these patients have no direct relationship with MCL bursitis; therefore, they may have little diagnostic value.
The etiology of bursitis is multifactorial. It has been attributed to repetitive knee movement, excessive pressure on the medial knee, and resultant friction between the superficial portion and the deep portion of the MCL, leading to bursal inflammation. Osteoarthritis, autoimmune diseases such as rheumatoid disorders, and trauma are all linked to this disease pathway.1,2,4,15 In osteoarthritis with marginal osteophytes, the spurs may impinge on the MCL and lead to inflammation of the bursa.1,2 Three of the patients in this cohort are older than 70 years, and they had radiographic evidence of osteoarthritis of the knees. On the sonographic images, in addition to the marginal osteophytes identified in their examined knees, meniscal extrusions were also discovered. Meniscal extrusion is the external displacement of the meniscus with regard to the external aspect of the tibiofemoral compartment. It is also called meniscal subluxation. Most of the meniscal extrusion occurs in the medial meniscus because it bears more weight force than the lateral meniscus. 16 The development of the meniscal extrusion is related to the progress of osteoarthritis. 11 Sonography usually demonstrates the meniscus’ radial displacement with bowing of the overlying superficial layer of the MCL, narrowing of the medial joint space, and osteophytes at the margin of the medial tibiofemoral compartment. 8 Meniscal extrusion is also one of the important imaging signs of MRI for diagnosis of osteoarthritis in the knee. 1 Three of the four patients with MCL bursitis in this cohort had medial meniscal extrusion and osteoarthritis. This finding could suggest that osteoarthritis may be a factor in the development of MCL bursitis. Other unknown factors may also exist, such as the patient who had no recognizable history or specific clinical presentations associated with MCL bursitis.
The medical treatment of bursitis usually includes medication, focal injection, and surgery. Nonsteroidal anti-inflammatory medications such as aspirin and ibuprofen can be used first, combined with rest and the use of ice. Therapeutic injection of a steroid into a bursa can be an effective method. If long-term relief of the symptoms after the injection can be achieved, it confirms the diagnosis of bursitis. 2 However, blind injections have poor accuracy. Sonographically guided therapeutic injection of a mixture of anesthetic and long-active corticosteroid for MCL bursitis was introduced to increase accuracy and patient outcomes.17,18 Arthroscopic surgery may be avoided if the sonographically guided therapeutic injection achieves long-term effectiveness. 18 It is unfortunate that follow-up information on this cohort of patients was not available; therefore, their course of treatment could not be followed. This represents a limitation to this case series as the diagnosis of MCL bursitis could not be fully confirmed.
Conclusion
Since MCL bursitis is not a common disorder of the knee, there is a lack of imaging evidence that could lead to a definitive diagnosis. An MRI diagnosis of MCL bursitis has been made based on clinical history and exclusion of other related pathologies with similar imaging features of MCL bursitis. Long-term effectiveness of therapeutic injection has been additional evidence that leads to this diagnosis. Sonographic detection of the MCL and its related lesion is becoming a well-established imaging alternative. Lower cost and documentation of dynamic movement are advantages over MRI. This case series suggests that a sonographically detected fluid collection with a distinct and smooth border, between the superficial and deep portions of the MCL without MCL injury, may support the diagnosis of MCL bursitis. Sonography may also assist in differentiating bursitis from other medial knee conditions. Correlation study of sonograms and sonographically guided therapeutic injections will raise the diagnostic effectiveness of MCL bursitis.
Footnotes
Acknowledgements
The author thanks his colleague Ms. Shaline Chandrarajan for helping prepare this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.