
Abstract
A venous aneurysm (VA) in a calf muscle is extremely rare. In this case study, a primary medial gastrocnemius vein aneurysm (MGVA) with thrombosis is reported. A female patient presented with left medial knee pain for 2 weeks. Radiograph demonstrated severe osteoarthritis of the medial compartment of the left knee. Sonography of the knee incidentally detected a focal saccular dilation in one of the gastrocnemius veins, within the medial head of the gastrocnemius (MHG). The diameter of the dilation was almost three times its connected normal vein. Two-thirds of the saccular dilation was occupied by hyperechoic content. Duplex sonography confirmed that the dilation was a saccular MGVA with thrombosis. The patient had no history of knee trauma, surgery, or inflammation. A small Baker’s cyst, medial to the MHG, was also excluded from the cause of the MGVA. These suggest that this MGVA was of a primary cause. The complications of a MGVA are briefly discussed as part of this case study.
A venous aneurysm (VA) is a focal dilation of a vein approximately two to three times its connected normal vein. 1 Based on the cause, VAs are classified into primary and secondary. 2 Secondary VAs are the sequelae of preceding medical conditions, which have been reported as mechanical trauma, venous hypertension, and inflammation. Primary VAs are those without identifiable causes. Even though VAs are uncommon, they have been reported in most major veins.3,4 However, VAs in calf muscles are extremely rare, and only two cases have been reported.5,6 One is in the soleal muscle, and the other is in the medial head of the gastrocnemius (MHG) secondary to compressive trauma in the knee. 6 In this study, a case of primary medial gastrocnemius vein aneurysm (MGVA) with thrombosis is described. Based on a search of the literature, this type of MGVA has not been reported previously.
Case Report
A 72-year-old female was referred for left knee radiograph and sonographic examinations due to left medial knee pain for 2 weeks. The patient had no history of left knee trauma, surgery, or inflammatory. Physical examination revealed left medial knee palpable tenderness without swelling. There was no sign of varicose in the left leg. The left knee radiography was reported as demonstrating severe osteoarthritis of the medial compartment, with varus deformity.
A systematic sonogram of the left knee was performed with a linear high-frequency transducer (6–15 MHz) using the General Electric (GE) LOGIQ S8 ultrasound system (GE Ultrasound, Waukesha, Wisconsin). The scanning protocol complied with the “Musculoskeletal (MSK) ultrasound technical guidelines” issued by European Society of Musculoskeletal Radiology. Mild joint effusion was found in the suprapatellar region of the knee. Medial meniscal extrusion with a vertical tear was also identified. A small Baker’s cyst (2.3 × 1.5 × 0.7) was located between MHG and the semimembranosus tendon in the popliteal fossa. Incidentally, a focal saccular dilation in a blood vessel, within MHG, was noticed (Figure 1A and B). The vessel was identified as one of the gastrocnemius veins. The saccular dilation was 0.98 in diameter and 0.99 in length, while the diameter of its connected vessel was 0.33. Two-thirds of the dilation was occupied by mildly hyperechoic content. Power Doppler showed dynamic non-pulse flow in both the vein and the saccular dilation. No blood flow was displayed in the mildly hyperechoic area (Figure 2A and B), which indicated a thrombus, in the dilation. The focal dilation was located at the same level with the Baker’s cyst (Figure 3). The dilation connected vessel went cephalad with four parallel gastrocnemius veins (Figure 4) and converged into one main trunk, before entering the popliteal vein. This patient was referred to a vascular specialist for further evaluation and management.
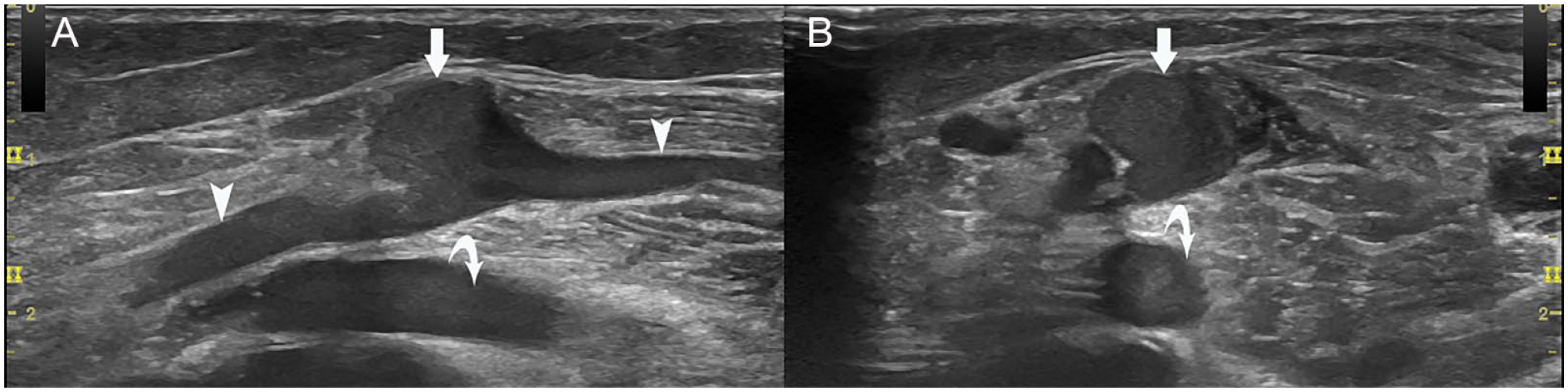
Focal saccular venous dilation in MHG: (A) Longitudinal view of the focal dilation (arrow) of the gastrocnemius vein (arrow heads). (B) Transverse view of the dilation. MHG, medial head of the gastrocnemius. Popliteal vein (curved arrow) is lateral and deep to the gastrocnemius vein.
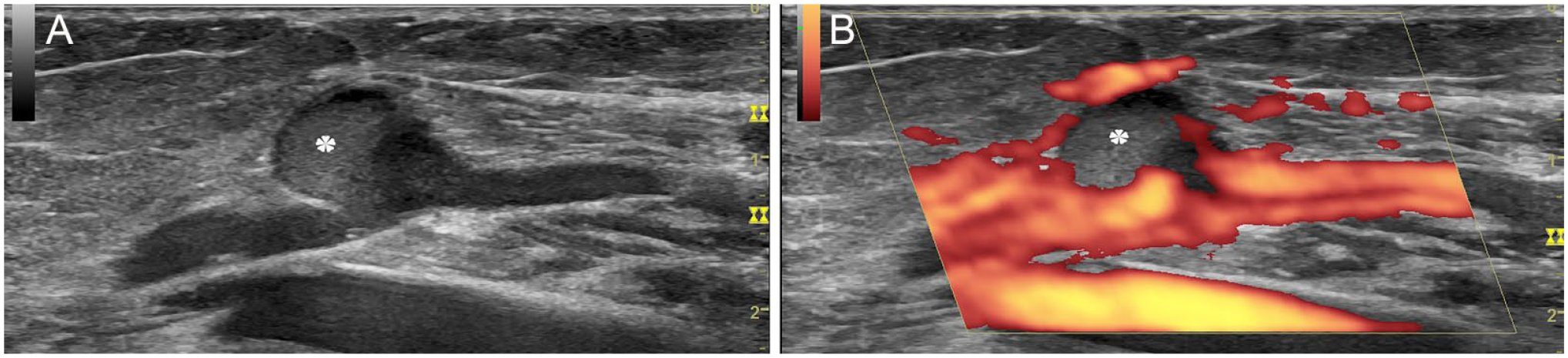
Thrombosis in the saccular dilation of the gastrocnemius vein: On longitudinal view, (A) two-thirds of the dilation was occupied by mild hyperechoic content (asterisk). (B) Power Doppler showed no blood flow in the mild hyperechoic area.
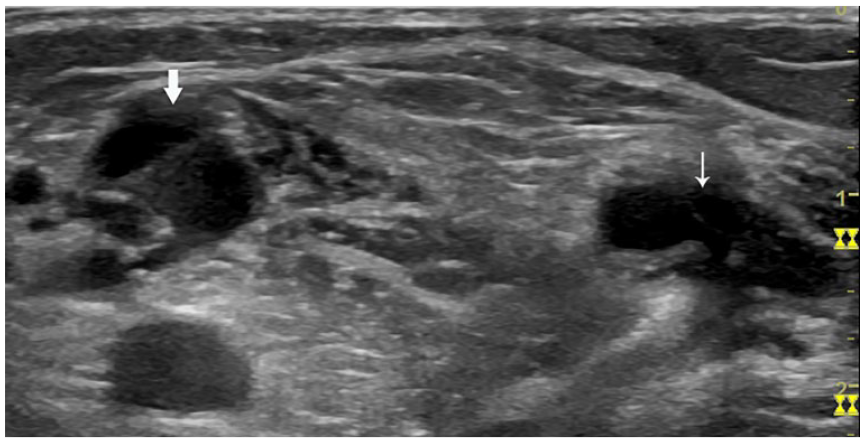
The saccular dilation of the gastrocnemius vein was at the same location level with the Baker’s cyst. On transverse view, the dilated vein (arrow) in MHG, and the Baker’s cyst (thin arrow) medial to MHG. MHG, medial head of the gastrocnemius.
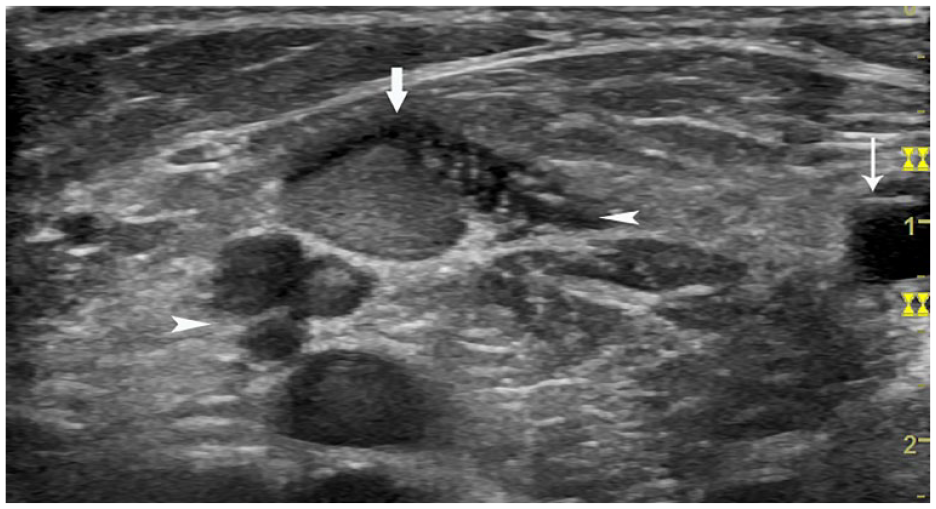
The saccular dilated vein is one of the five gastrocnemius veins in MHG: On transverse view, the dilated vein (arrow) and its four parallel gastrocnemius veins (arrow heads), and the medial Baker’s cyst (thin arrow). MHG, medial head of the gastrocnemius.
Discussion
The veins of lower limbs are classified into superficial and deep groups. The deep veins in the leg include deep calf and sural veins. The former include paired anterior tibial, posterior tibial, and fibular (or peroneal) veins. The latter include soleal veins, as well medial and lateral gastrocnemius veins. 7 The soleal veins originate from the soleus muscle and drain into the posterior tibial or peroneal veins. The medial and lateral gastrocnemius veins are from the medial and lateral heads of the gastrocnemius, respectively. There are approximately 2 to 12 veins with a mean 4.6 in each muscle head. They converge to a main trunk from each head before draining into the popliteal vein. 8 The drainage sites of the medial and lateral main trunks are at the same level as the small saphenous vein entering the popliteal vein. 9 A universal dilation or thickening of one of the gastrocnemius veins in MHG is occasionally seen. However, a focal dilation is rare. The current case not only presents a focal saccular dilation, but also has dilation that is three times in comparison with the connected normal vein. It is consistent with the consensus definition of VA. The uniqueness of the current case is that the location of the aneurysm is in one of the five gastrocnemius veins in MHG, while the reported MGVA caused by compression trauma is in the main trunk, near its confluence in the popliteal vein. 6
The pathogenesis of primary VA is still unknown, even though several hypotheses have been proposed. One consensus theory is that the focal vein wall weakness caused by congenital underdevelopment of normal connective tissue progresses to focal dilation.1,4,10 By analyzing the patient’s medical history and the unique location of the aneurysm, we tend to conclude that the current case is a primary MGVA. The following evidence supports our assumption. The current case has no history of local injuries, or inflammation; in addition, the coexisting Baker’s cyst can be excluded as an inciting factor. It has been reported that large Baker’s cyst could compress popliteal vein and cause thrombosis. 11 Although the current case has a Baker’s cyst, it is small and has no sign of compression on its medial MHG. Moreover, from the anatomical and hemodynamic aspects, if the cyst were a compression factor, it should be located at the level cephalad to the MGVA. Nevertheless, the fact is that the cyst and the MGVA are at the same level in the popliteal fossa. Furthermore, this MGVA is in only one of the five medial gastrocnemius veins in MHG. All the above suggest that the Baker’s cyst has no impact on the development of MGVA of the current case. Therefore, it is deduced that this MGVA is a primary cause.
Isolated deep vein thrombosis (IDVT), in the calf, includes the isolated calf muscle vein thrombosis (ICMVT; thrombosis confined to the sural veins) and deep calf vein thrombosis (DCVT; thrombosis confined to the paired calf veins). Its prevalence among patients with lower extremity DVT varies from 11.1% to 34%,9,12,13 while the prevalence of ICMVT varies from 10.4% to 25%. 14 Among IDVT in the calf, 37% is ICMVT. 12 Soleal vein thrombosis is more common than gastrocnemius vein thrombosis, and is frequently seen coexisting with DCVT.12,15 The coexisting chance of soleus and gastrocnemius veins thrombosis is low. 15 The complications of IDVT include propagation to proximal deep veins and pulmonary embolism (PE). In all, 15% to 25% of untreated IDVT in the calf may propagate proximally, and one-third of IDVT in the calf may have PE. 13 Among patients with ICMVT, 9% progress to proximal (proximal to the knee) DVT, and 4% to PE. 14 The development of ICMVT has not been elucidated. 9 However, some factors such as smaller diameter of the muscle veins, and long-haul flights, seem to contribute more to ICMVT.9,16 Aneurysm is a high-risk factor for DVT. 17 A reported recurrent ICMVT is due to a VA of the soleal muscle veins. 5 The current case of MGVA has a thrombus, which distinguishes it from the reported case of MGVA secondary to compressive trauma in the knee, as latter has no thrombosis. 6 Among the three sural aneurysms (including the current case), two are complicated with thrombosis, but without PE. This finding may imply the possibility of high prevalence of thrombosis, but low occurrence of PE in sural vein aneurysms. Because of this assumption being limited by the rarity of sural vein aneurysm, more patient cases are required for further investigation.
An asymptomatic deep VA is usually an incidental finding during a MSK sonogram. If a deep VA is suspected, duplex sonography is the first choice for a vascular diagnosis, as it is noninvasive, inexpensive, easily repeatable, dynamic, and without ionizing radiation. 4 It is also reliable in determining the characteristics of a VA, such as the site, size, thrombus presence, and the relationship with adjacent vessels and tissues. The current case was found incidentally during a routine knee sonography, for medial knee pain. The reported pain may have been caused by severe osteoarthritis of the medial compartment of the knee. The above-mentioned characteristics of a VA were also established in the current case by the dynamic duplex sonography. Regarding the management of the sural vein aneurysm, there is no specific guidelines provided. However, a recent clinical research on the treatment of the popliteal vein aneurysm may provide a reference value. Surgical resection may be the choice of treatment for large, symptomatic sural vein aneurysm, or the one complicated with thrombosis. Surveillance alone may be sufficient for small asymptomatic ones without thrombosis. 17
Conclusion
This case is the first reported primary VA in sural veins. Its location and the presentation of thrombosis in the MGVA also distinguishes this case from the other cases that have been reported. The occurrences of the MGVA complications, especially PE, are still unknown. More patient cases are required for further investigation of this diagnosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.