
Abstract
Popliteal artery aneurysms are rare, but they have the potential to be limb threatening as a result of thrombosis and distal embolization. Duplex sonography may be used to effectively detect popliteal artery aneurysms and determine patency of the runoff arteries. Findings may include dilatation of the popliteal artery during gray-scale imaging with intraluminal heterogeneous echoes indicating the presence of mural thrombus. Abnormal or absent Doppler signals in the more distal arteries with intraluminal heterogeneous echoes may indicate the presence of thrombus, likely from embolization. This case presents the duplex sonography findings of bilateral popliteal artery aneurysms in conjunction with lower extremity acute arterial thrombosis and an abdominal aortic aneurysm.
Keywords
Although rare, popliteal artery aneurysms (PAAs) are the most common peripheral arterial aneurysm. More than 90% of patients are male, with the aneurysms occurring most frequently in the sixth and seventh decades of life.1,2 PAAs also are known to have a high association with other arterial aneurysms. Of patients diagnosed with a PAA, 50% have a contralateral PAA; 37% have a concomitant abdominal aortic aneurysm (AAA); 34% have a femoral artery aneurysm; and 25% have an iliac artery aneurysm.2,3 While PAAs are not likely to rupture, they can be limb threatening due to thrombosis and distal embolization. Symptomatic PAA may present with claudication, rest pain, or signs of severe acute or chronic lower extremity ischemia. Treatment options for PAA include bypass graft, endovascular repair, thrombolysis, and amputation.1 -5 Duplex ultrasonography (DU) is the recognized modality for noninvasively identifying PAAs,6 -8 as this examination can effectively detect PAAs and evidence of mural thrombus and determine the patency of the runoff arteries.
Case Report
An 89-year-old man presented to the emergency department complaining of left lower extremity rest pain with associated skin discoloration. The patient stated that his left foot began to feel cool to the touch and had become discolored approximately 1 week prior. He had a known history of atrial fibrillation and was not currently on anticoagulation. Upon physical examination, the left lower extremity was cyanotic and cold from the knee to the foot. The pedal pulses were neither palpable nor able to be detected with a handheld continuous wave Doppler flowmeter.
An arterial duplex sonogram was performed with a GE Vivid E9 (GE Healthcare, Milwaukee, WI, USA) with a 2.4- to 10-MHz linear-array transducer and a 1.5- to 4.6-MHz phased-array transducer. DU was performed on the abdominal aorta and bilaterally on the common femoral, superficial femoral, popliteal, posterior tibial, peroneal, anterior tibial, and dorsalis pedis arteries. Images were also obtained of the popliteal veins bilaterally. The examination was done with gray-scale imaging with the use of color Doppler imaging and spectral Doppler waveform analysis.
The right midpopliteal artery was seen to be aneurysmal with mural thrombus, having a maximum diameter of approximately 2.8 cm with a residual lumen of 1.2 cm (Figures 1 and 2). The right proximal popliteal artery had a maximum diameter measurement of 1.2 cm. There were normal triphasic Doppler flow signals noted in the right common femoral, superficial femoral, popliteal, posterior tibial, peroneal, anterior tibial, and dorsalis pedis arteries (Figures 3 and 4). The right popliteal vein was patent as well, with no evidence of any thrombus.
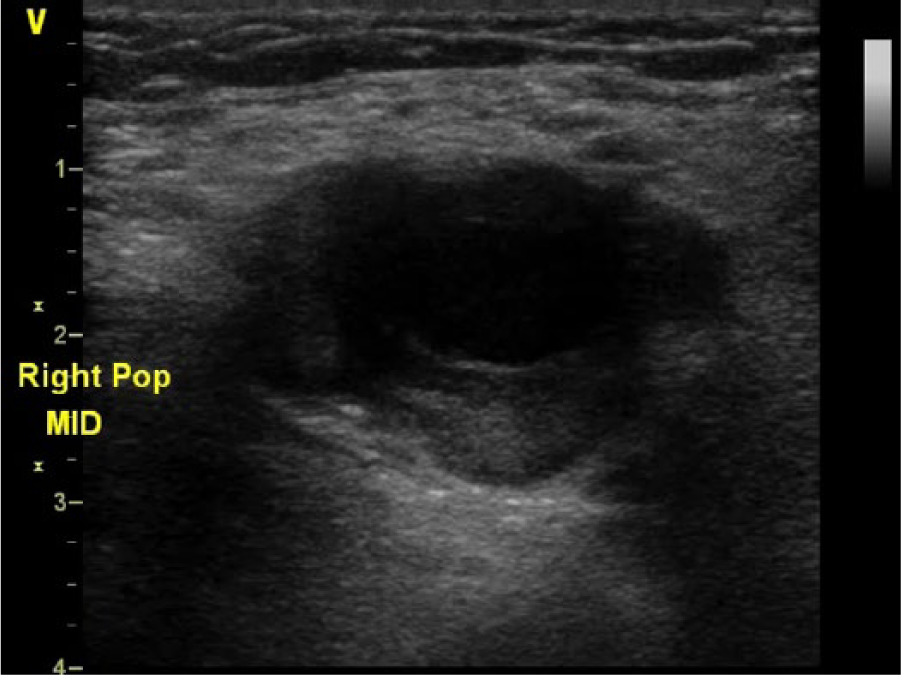
Cross-sectional gray-scale image of the right mid- popliteal artery showing aneurysmal dilation with echogenic filling within the lumen characteristic of mural thrombus.
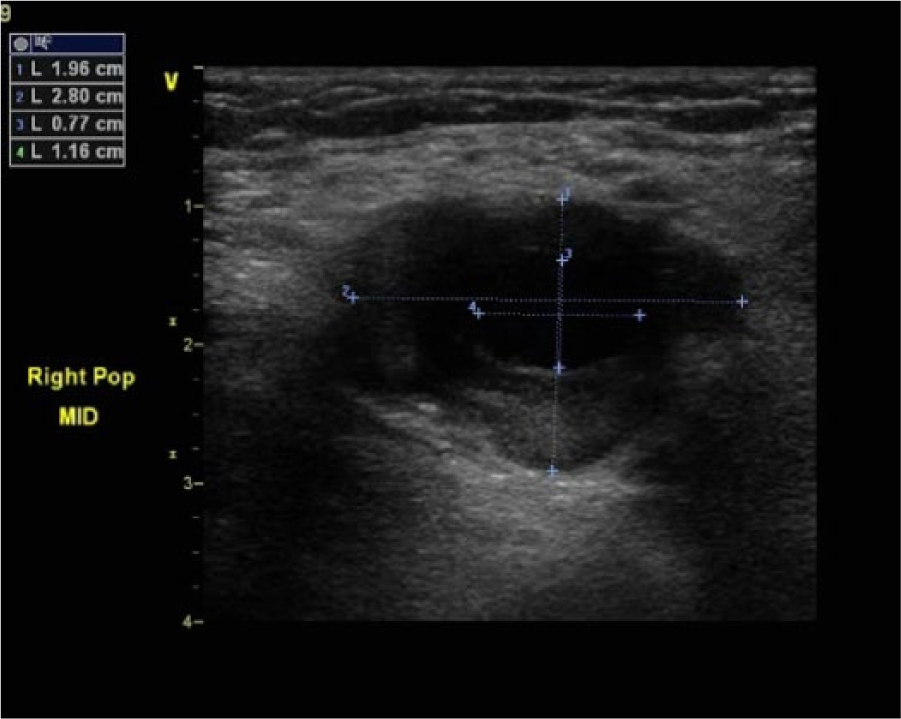
Cross-sectional gray-scale image of the right mid-popliteal artery with electronic caliper measurements showing an aneurysmal dilation (2.0 × 2.8 cm) and a residual lumen (0.8 × 1.2 cm).
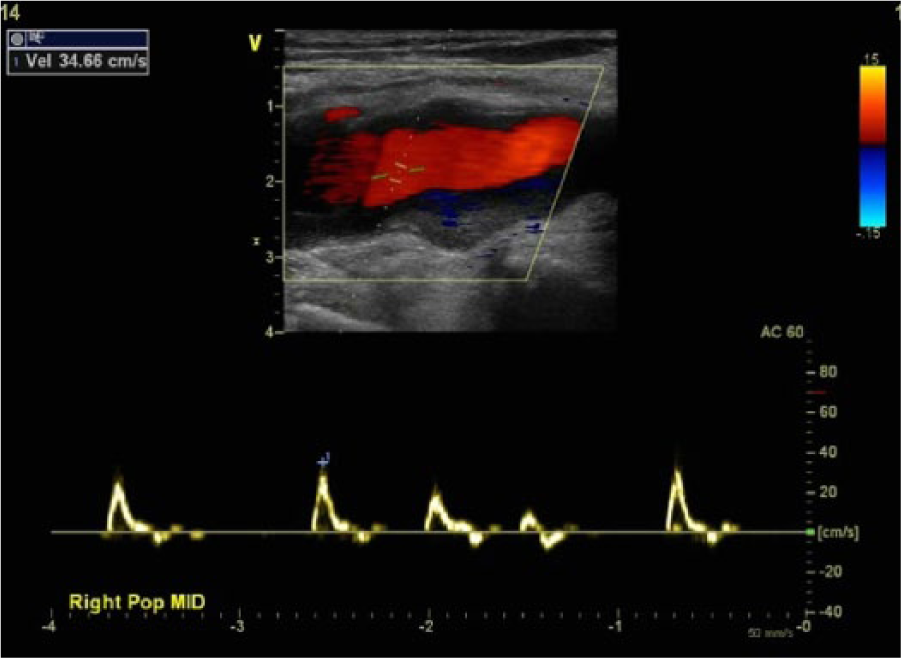
Color and spectral Doppler image taken at the site of maximal right popliteal artery aneurysmal dilation showing mural thrombus but no evidence of significant obstructive disease and an essentially normal triphasic spectral Doppler signal. Incidental note is made of a cardiac arrhythmia.
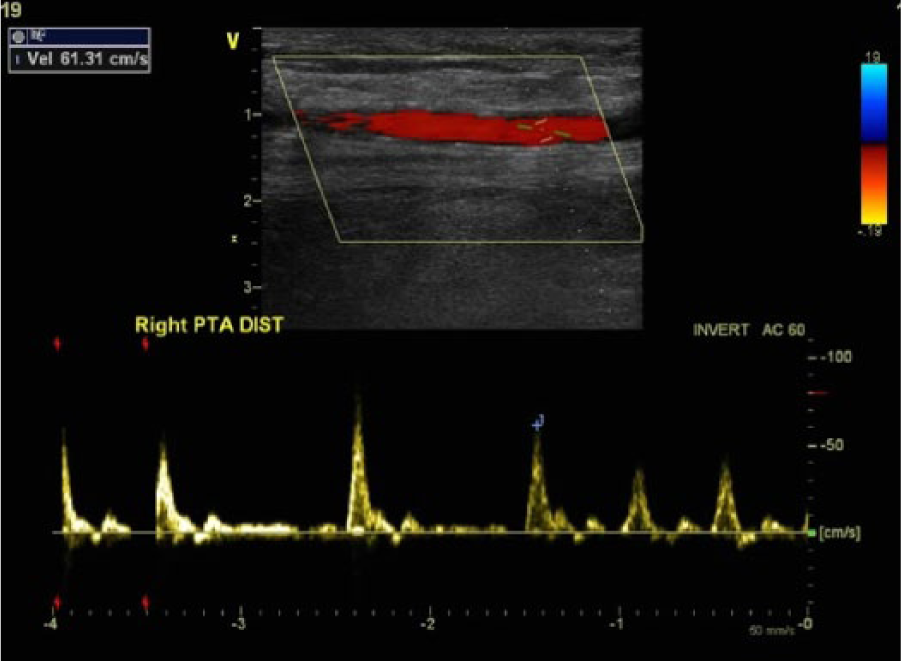
Color and spectral Doppler image taken at the distal right posterior tibial artery showing no evidence of significant obstructive disease and an essentially normal triphasic spectral Doppler signal.
The left midpopliteal artery was also noted to be aneurysmal with mural thrombus and had a maximum diameter of approximately 4.5 cm with a residual lumen of 1.3 cm (Figures 5 and 6). The left proximal popliteal artery had a maximum diameter measurement of 1 cm. There was a low-velocity, high-resistive Doppler flow signal noted in the left popliteal artery, suggestive of a distal obstruction (Figure 7). There was no Doppler flow signal detected in the left posterior tibial, peroneal, anterior tibial, and dorsalis pedis arteries (Figure 8). During gray-scale imaging of these arteries, heterogeneous echogenic material was noted intraluminally, consistent with arterial thrombosis (Figure 9). The left common femoral and superficial femoral arteries appeared normal with triphasic flow. The left popliteal vein was also noted to be patent.
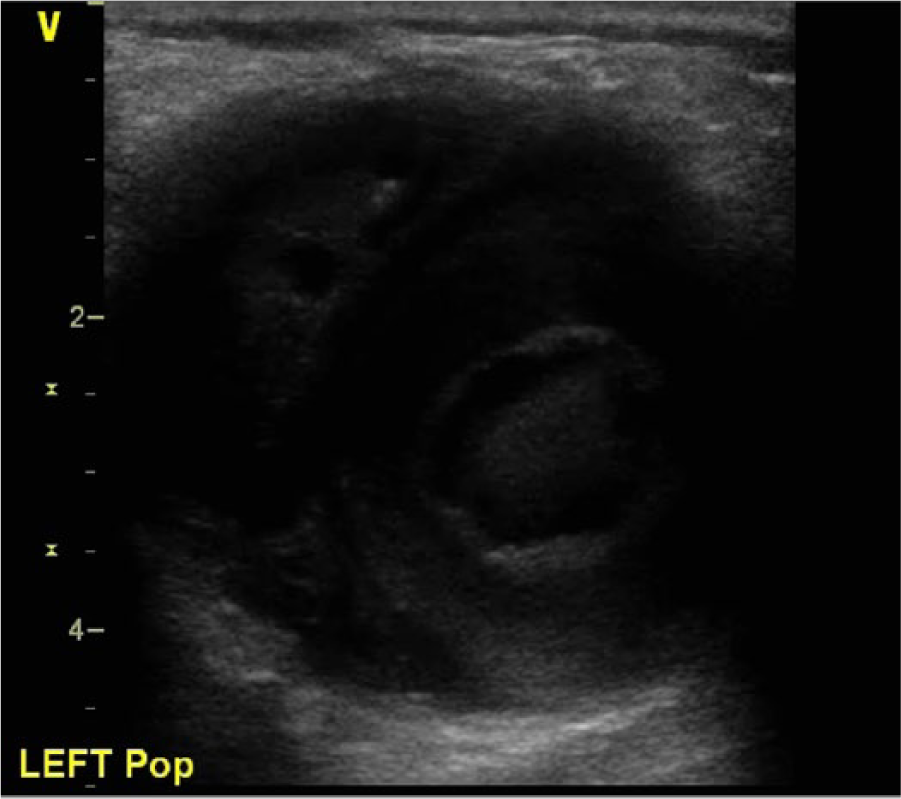
Cross-sectional gray-scale image of the left mid- popliteal artery showing aneurysmal dilation with echogenic filling within the lumen characteristic of mural thrombus.
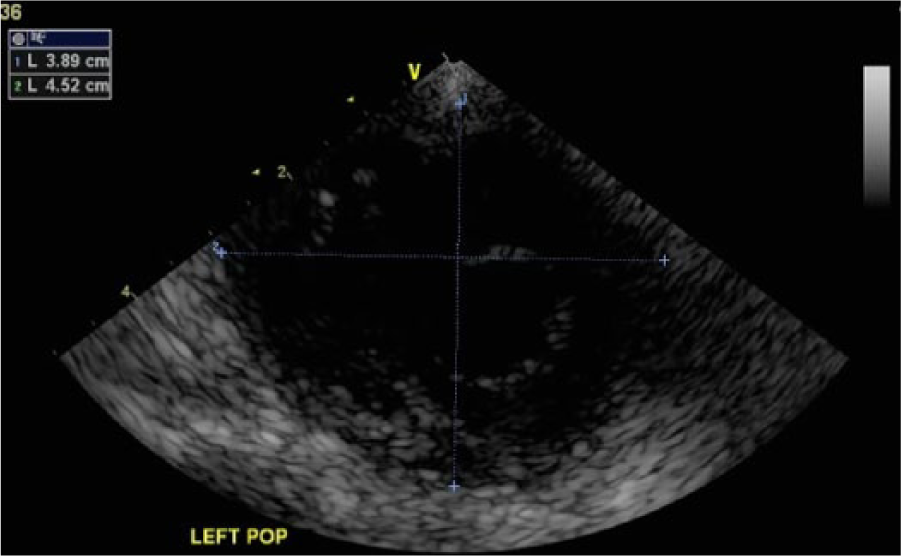
Cross-sectional gray-scale image of the left mid-popliteal artery with electronic caliper measurements showing an aneurysmal dilation (3.9 × 4.5 cm).
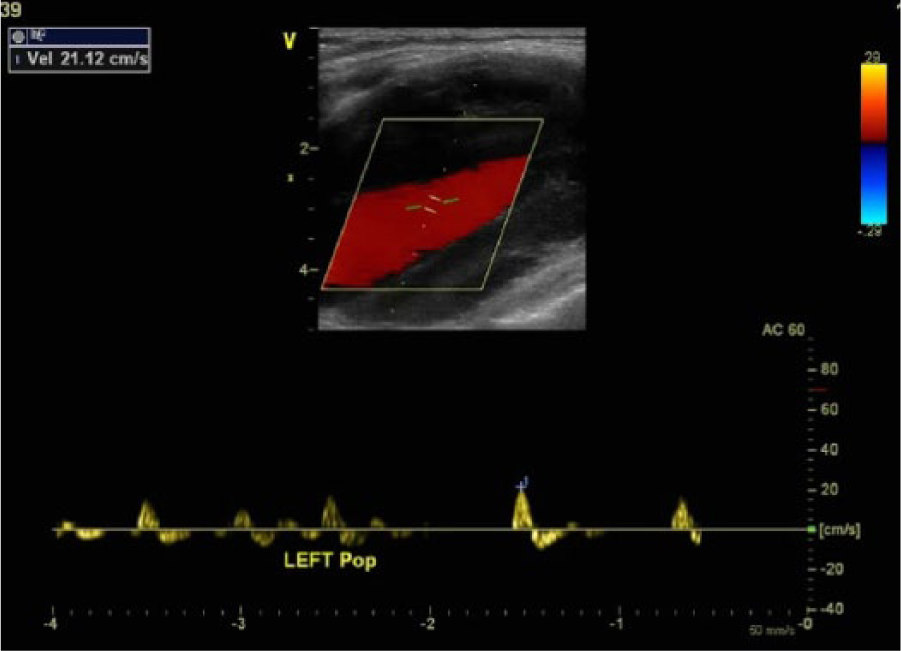
Color and spectral Doppler image taken at the site of maximal left popliteal artery aneurysmal dilation showing mural thrombus but no evidence of significant obstructive disease with a diminished spectral Doppler signal (compared to the right side) and an absence of a diastolic flow component characteristic of a high-resistive waveform secondary to more distal obstruction.
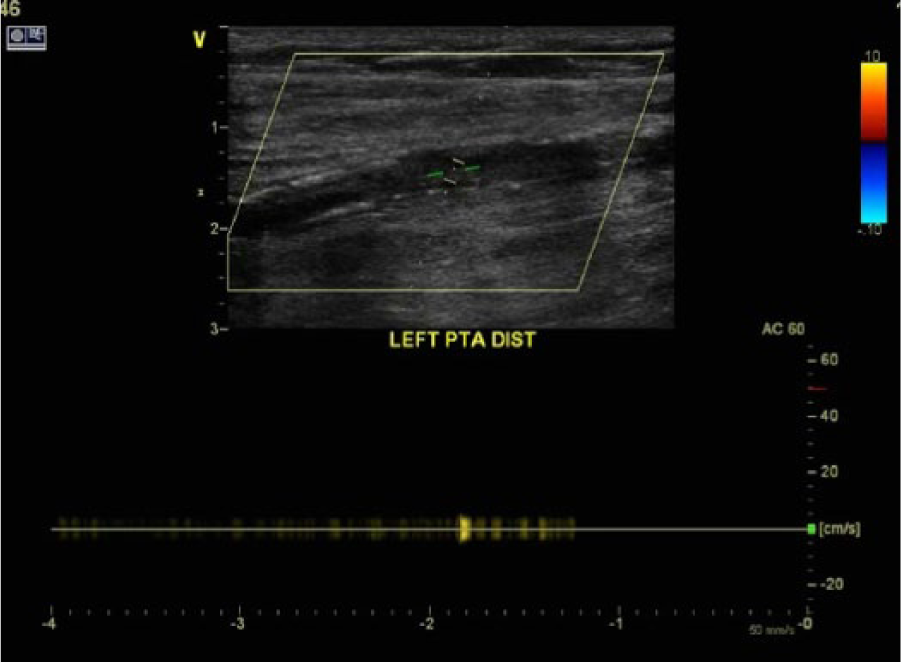
Color and spectral Doppler image taken at the distal left posterior tibial artery showing occlusion of the vessel, with no evidence of any color filling of the arterial lumen and an absent spectral Doppler flow signal.
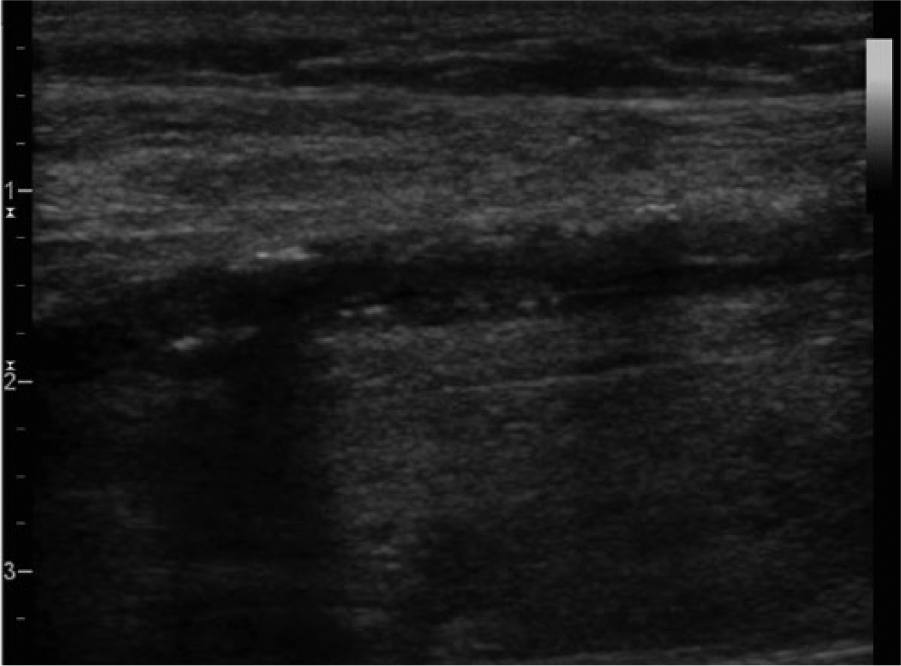
Sagittal gray-scale image of the distal left posterior tibial artery showing diffuse intraluminal heterogeneous echoes.
Evaluation of the abdominal aorta was attempted as well, though bowel gas partially obscured the abdomen. The midinfrarenal abdominal aorta was visualized and seen to be patent but aneurysmal, with a maximum diameter of approximately 4.1 cm (Figure 10). Because of the patient’s elevated creatinine level, an aortogram and pelvic arteriogram were not performed. A unilateral left leg arteriogram confirmed the occlusion of the trifurcation vessel system with no distal flow detected in the runoff arteries. The left common femoral, superficial femoral, and popliteal arteries were patent.
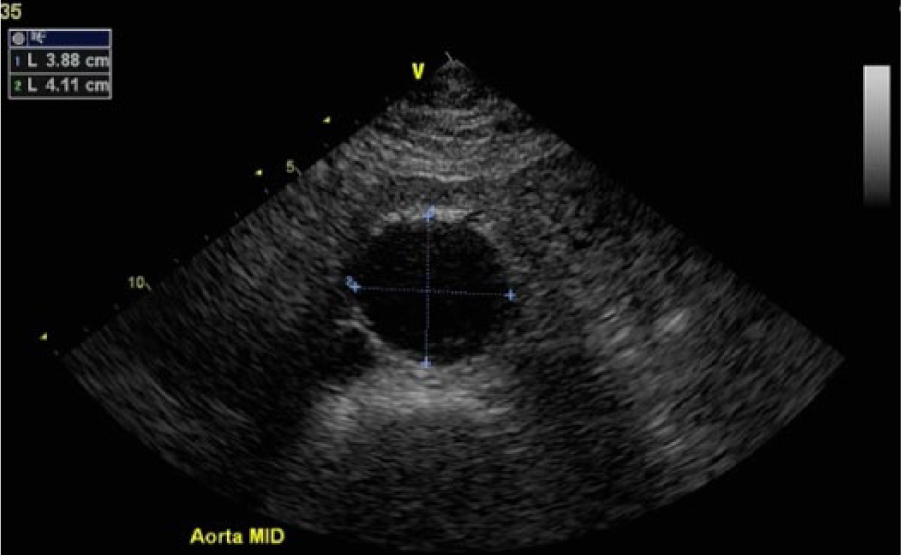
Cross-sectional gray-scale image of the midinfrarenal abdominal aorta showing aneurysmal dilation measuring 3.9 × 4.1 cm. No evidence of mural thrombus was seen.
The patient was taken to the operating room, where a reversed great saphenous vein above-knee popliteal artery to tibioperoneal trunk bypass was placed. The left popliteal artery was noted to be aneurysmal, measuring approximately 5 cm. Thromboembolectomy of the posterior tibial and peroneal arteries also was done.
A computed tomography scan of the abdomen and pelvic region was performed approximately 1 week later, which showed an infrarenal AAA measuring maximally between 4.5 and 5 cm.
Subsequently, the patient developed forefoot gangrene, and a left above-knee amputation was deemed necessary 9 days after the initial presentation to the emergency department.
Discussion
The normal diameter of the popliteal artery has been reported extensively in the literature, ranging from 0.5 to 0.9 cm.1,9 The popliteal artery is considered aneurysmal with a localized dilatation to 1.5 cm in diameter or a 1.5-times increase in size compared to a normal proximal segment.1,5,10 Atherosclerosis is the most common etiologic factor associated with PAAs, while they are less commonly associated with mycosis, connective tissue disorders (e.g., Marfan syndrome), trauma, or popliteal artery entrapment.8,10 Comorbidities often found in patients with PAAs include hypertension, cardiovascular disease, stroke, and diabetes.
Approximately two-thirds of PAAs are symptomatic and, when left untreated, have a 35% incidence of thromboembolic complications. 2 Symptomatic patients with PAAs most often present with signs of lower extremity ischemia, such as claudication and rest pain.1 -3,10 Localized pain at the popliteal fossa and/or swelling can also occur in patients with PAAs as a result of compression of the nerves and veins. In cases of acute thrombosis or embolization from the PAA, the patient may present with signs of acute ischemia, such as foot coolness, discoloration, or numbness.
Treatment of PAAs is recommended in the presence of symptoms and for asymptomatic aneurysms that reach 2 cm in diameter or contain significant amounts of thrombus. Other studies have recommended repair of all PAAs regardless of size or symptoms.2,3,11 -15 Still, some researchers have suggested incorporating aneurysm distortion as a means of determining elective surgical treatment in mid- to smaller-sized aneurysms measuring <3 cm in maximum lumen diameter.5,10,16
Conventional repair of PAAs involves the use of a vein bypass graft with anastomoses proximal and distal to the aneurysm. In the presence of acute limb ischemia due to thrombosis, thrombolysis in conjunction with bypass grafting may be necessary to clear the runoff arteries.1,4 Endovascular repair of PAAs is another option that has been reported to decrease recovery time and length of hospital stay. 17 The stent graft, which excludes the aneurysm, also crosses the knee joint. This location can result in repetitive stress on the stent graft.17,18 Studies reporting on endovascular repair of PAAs have shown 2-year primary patency rates of 77% to 87% and secondary patency rates of 87% to 100%.17,18 The early results of endovascular repair of PAAs were not as promising as later results, and until recently, open repair was still the favored approach. 19 As technology improved and interventionalists became more familiar with the necessary techniques, the choice of open versus endovascular repair is now made more on the basis of clinical evaluation of the patient and the operator’s level of experience with either technique.20,21 However, for endovascular repair, the long-term patency rates, particularly rates in cases of PAAs with acute limb ischemia, have limited reporting in the literature.15,20
DU is the imaging modality most commonly utilized in the initial identification of PAAs. MacGowan et al. reported on the accuracy of DU in the identification of PAAs compared with angiography. In their study, DU identified 11 PAAs later confirmed at operation, while angiography only identified 7 of the 11 PAAs. 6 Angiography may not be able to diagnose PAA if there is significant thrombus or occlusion of the aneurysm. In a study evaluating femoral and PAAs in patients with AAA, Diwan et al. noted that sonography may be more appropriate than physical examination in the detection of peripheral aneurysms in men with AAA. 7 Duplex sonography can also detect mural thrombus associated with a PAA, extrinsic compression of the veins due to aneurysm size, and the patency of the runoff arteries.
Although PAAs have a low prevalence, it is important to be able to accurately identify a PAA along with the associated abnormalities during a DU examination. Dilatation of the popliteal artery is noted during gray-scale imaging and may be associated with evidence of mural thrombus appearing as intraluminal heterogeneous echoes that partially fill the aneurysm sac. 22 The important clinical measurements include location and diameter of the PAA; diameter of the popliteal artery proximal and distal to the PAA; and color and spectral Doppler signals proximal, within, and distal to the PAA. 22 Evidence of mural thrombus and residual lumen diameter measurements are also noted. Diameter measurements are obtained in a transverse view, while the Doppler signals are obtained from a longitudinal view. 22 Patency of the popliteal vein is determined as well, noting any signs of extrinsic compression from the arterial aneurysm. The posterior tibial, peroneal, anterior tibial, and dorsalis pedis arteries are evaluated for evidence of thromboembolism from the PAA. Abnormal or absent Doppler signals along with evidence of intraluminal heterogeneous echoes may indicate thromboembolism. Due to the high association of PAAs with other arterial aneurysms, the contralateral limb and the abdominal aorta should be assessed in the same manner.2,3,23
Differential diagnoses include popliteal cyst, popliteal artery pseudoaneurysm, popliteal vein aneurysm, and popliteal vein thrombosis.24,25 The supplemental use of color and spectral Doppler can distinguish a PAA from a popliteal cyst as well as a popliteal vein aneurysm and popliteal vein thrombosis. Careful interrogation of the popliteal artery with color Doppler and spectral waveform analysis can help determine if the PAA is a true aneurysm or a pseudoaneurysm.
Conclusion
In cases of suspected PAA, DU is the accepted modality for noninvasive evaluation. Through use of DU, a PAA can be visualized in the popliteal fossa with dilatation of the popliteal artery noted during gray-scale imaging. DU also can identify evidence of mural thrombus within a PAA and thrombosis of the more distal arteries. A meticulous DU examination can distinguish a PAA from other conditions and provide detailed data on the aneurysm along with any associated abnormalities (e.g., distal embolization, contralateral PAA, AAA). In the presented case, utilizing a comprehensive DU examination protocol made it possible to accurately detect the PAA, the status of the runoff arteries, and evidence of a contralateral PAA as well as an AAA.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.