
Abstract
Objective:
The study aimed to determine the accuracy of sonography in diagnosing pyomyositis.
Methods:
A retrospective review of pyomyositis cases in a government hospital between January 1, 2016 and June 30, 2019 was done. All cases underwent a sonogram for the indication of pyomyositis. Positive purulence for surgical cases and improved laboratory parameters for conservative cases were confirmatory for pyomyositis. Comparison with sonographic results using a 2 × 2 contingency table was done to determine sensitivity and specificity.
Results:
A total of 122 cases were included. The sonographic results corresponded with 95% of surgical cases and 89% of conservative cases. A lack of false and true negatives for surgical cases resulted in a sensitivity of 100% (95% confidence interval [CI] = 93%–100%) and a specificity of 0% (95% CI = 0%–71%). In conservative cases, sonography had a sensitivity of 92% (95% CI = 82%–97%) and a specificity of 0% (95% CI = 0%–84%) due to a lack of true negatives.
Conclusion:
Sonography is not limited to primarily as a screening tool but a capable diagnostic imaging choice for pyomyositis, particularly in low-resource settings. The results show the strength of sonography, particularly in the suppurative stage of pyomyositis.
Key Takeaways
Localized inflammation, leukocytosis, increased erythrocyte sedimentation rate and c-reactive protein should warrant a consideration of pyomyositis.
Clinical and laboratory findings are complementary to imaging when considering pyomyositis.
Sonography is not limited to as primarily a screening tool.
Sonography appears to have more utility in the suppurative stage of pyomyositis.
Pyomyositis is a bacterial infection that results in an intramuscular abscess and was first described by Scriba in 1885.1–3 It is endemic throughout the tropics and accounts for 2.2%–4% of surgical admissions and 1%–4% of all hospital admissions with a peak incidence at 2–5 years of age.2–4 Recent data still present pyomyositis as primarily a disease of the tropics; however, reports of cases from temperate regions are increasing.1,2,5
The term tropical pyomyositis or primary pyomyositis is restricted to a primary muscle abscess arising within the skeletal muscle. Most patients with tropical pyomyositis are children or young adults who are otherwise healthy without underlying comorbidities, while most patients in temperate regions are adults and elderly who are immunocompromised or have other serious underlying conditions.3,5,6 The definite pathophysiology is still unknown but is widely accepted to be hematogenous in origin. An association between transient bacteremia in the setting of skeletal muscle injury has been reported. Local trauma has been suggested as a risk factor in developing primary pyomyositis with 20%–50% of cases reporting a history of antecedent trauma to the affected muscle group.1–6 Pyomyositis commonly involves the proximal, large muscles of the lower limb, i.e., quadriceps, glutei, iliopsoas, and gastrocnemius.1,2,4,5,7 Previous authors have outlined three stages of pyomyositis: invasive, suppurative, and late. Most patients present and are diagnosed in the suppurative stage which is characterized by abscess formation.1–4,8
Establishing a working diagnosis during the invasive or suppurative stage remains a challenge. Laboratory investigations are not specific and are rarely helpful in the diagnosis of pyomyositis with studies show moderate leukocytosis with a left shift, elevation of erythrocyte sedimentation rate (ESR) and c-reactive protein (CRP) and normal muscle enzyme levels.1,2,4,5,7 Pyomyositis is often misdiagnosed because of unfamiliarity with the disease, atypical manifestations, a wide range of differential diagnoses, and a lack of early specific signs.1,2 A delay in diagnosis can result in increased morbidity and a significant mortality rate.2,5 Aggressive management once diagnosed leads to complete recovery without long-term complications. Serious complications can include local extension into adjacent bone or joint, compartment syndrome, remote infection such as myocarditis, lung and brain abscess, eventual sepsis, and death. Reports of mortality rates differ from 0.5% to 2%, 4 0.9% to 10%, 9 and <1% to 4%. 10
Imaging is valuable due to the lack of specific clinical and laboratory findings in pyomyositis. Of particular importance is the presence of fluid or abscess collection that will stage the disease and determine the treatment plan. Magnetic resonance imaging (MRI) is established as the imaging modality of choice in the workup of musculoskeletal infections.9,11,12 Specifically for pyomyositis, MRI is the imaging gold standard.2,6,7,13,14 Other studies further specify the advantage of MRI in determining pyomyositis in specific regions of the body such as the lumbar region and pelvis,11,15 hip, 16 and spine. 17 Magnetic resonance imaging is considered an advanced imaging tool and is the investigation of choice in developed countries. 1 Despite the established advantages of MRI in diagnosing acute musculoskeletal infections at 97% sensitivity and 92% specificity, 11 the availability and accessibility of this modality in low-resource areas remains a problem. This warrants attention since the burden of disease of pyomyositis still falls primarily on the tropical low-resource areas. Most studies on the utility of sonography in pyomyositis are from an emergency point-of-care system in high-resource settings where a sonogram functions as an initial screening tool.1,5,7,8,12 In this setting, when sonographic features are suggestive of pyomyositis, advanced imaging with computed tomography (CT) or preferably MRI is then generally pursued. However, in low-resource settings, sonography functions as the primary and sole diagnostic imaging tool to establish pyomyositis.1,8 Previous studies have established the sensitivity and specificity of sonography in detecting skin and superficial soft tissue abscess formation.18–21 However, the sensitivity and specificity of sonography for detecting abscesses in deeper soft tissues and muscle, particularly pyomyositis, have not been described.
Despite the advancements of CT and MRI, the value of sonography in diagnosing pyomyositis is maintained since most patients seek consult during the suppurative stage with the onset of fluid collection or abscess formation. Pyomyositis, even with fluid collections, can easily be missed on clinical evaluation and sonography provides a relatively sensitive means for detection. 15 Sonography can also aid in excluding some differentials including superficial infection, i.e., cellulitis or cutaneous abscess. 7
Regardless of the chosen imaging modality, histopathologic evidence remains the gold standard for diagnosing pyomyositis. Aspiration of pus from muscle or muscle biopsy with culture and tissue staining in cases of absent macroabscesses is considered confirmatory. 4 However, conservatively managed patients with imaging findings of pyomyositis are signed off as pyomyositis when clinical signs and laboratory parameters improve with antibiotic treatment.
The accuracy of sonography in diagnosing pyomyositis in low-resource settings warrants further investigation, with most of the cases still in tropical low-resource settings, further establishing the capability of sonography in diagnosing pyomyositis is of primary value. The general objective of the study was to determine the accuracy of sonography in diagnosing pyomyositis. Comparison of sonographic findings with cases treated surgically and cases treated conservatively was done.
Methodology
This retrospective study was approved by our Institutional Ethics Review Board. Informed consent was waived for this study with patient and data privacy safeguarded as no identifying data were included in this publication. A retrospective medical chart review was done for this study using a International Classification of Diseases, Tenth Revision (ICD-10) diagnosis search. Cases with an admitting diagnosis of pyomyositis managed in the study hospital were sourced from the medical records section. The search included cases admitted from the period of January 1, 2016 to June 30, 2019. A total of 342 cases with an admitting diagnosis of pyomyositis were tagged for chart retrieval. The inclusion/exclusion criteria were as follows: inclusion to the study needed a referral to Musculoskeletal Ultrasonography (MSK-US) Section of the study hospital Rehabilitation Medicine Department with an initial diagnosis of pyomyositis to undergo a diagnostic MSK-US, an official MSK-US diagnosis written in the chart signed by the MSK-US Consultant-in-charge and one of two determined exposures as the reference standard. The exposure for surgically treated cases was the Operative Technique of the surgical procedure done on the same muscle group referred for MSK-US where the surgery must have been done after MSK-US results are released. The exposure for the conservatively treated cases were the laboratory parameters. Cases were excluded when the MSK-US procedure was done outside the study hospital Rehabilitation Medicine Department; there was previous diagnostic imaging done including MRI or MSK-US on the same muscle group leading to present admission or previous diagnostic aspiration/surgical procedure done on the same muscle group leading to present admission. Only 263 physical charts were retrieved from the records section which then underwent eligibility assessment using the inclusion/exclusion criteria. A total of 122 cases underwent a diagnostic musculoskeletal sonogram procedure in the Rehabilitation Medicine Department of the study hospital, and of these, 57 cases underwent surgery. Presence of purulent discharge as described in the intraoperative findings was confirmatory for pyomyositis. The remaining 65 cases represented conservatively treated cases. Presence of improved laboratory parameters with antibiotic treatment alone was determined to be diagnostic for pyomyositis. Both sets of cases were included as primary data. Figure 1 illustrates the process of inclusion and exclusion.
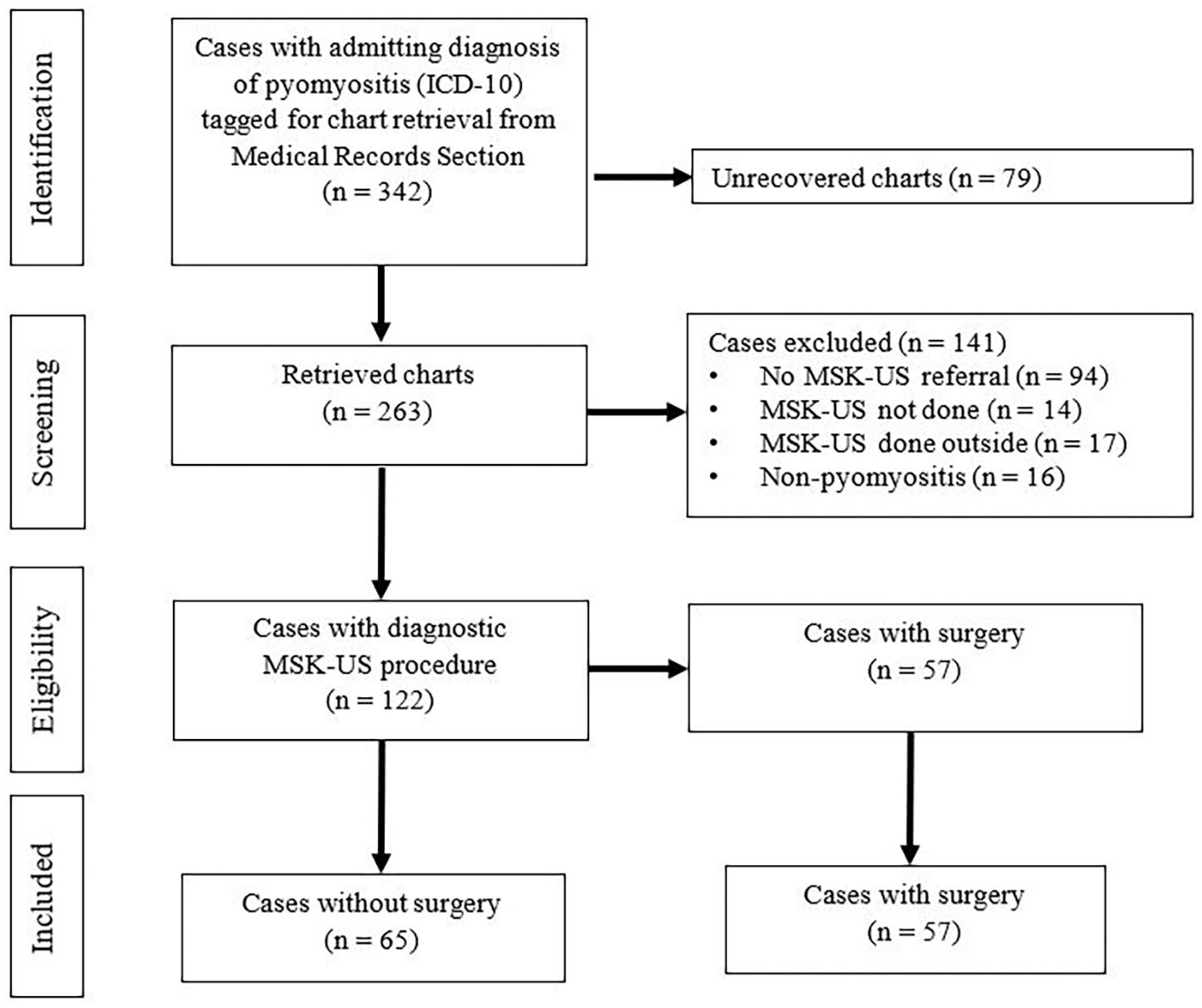
Process of inclusion into the study. MSK-US, Musculoskeletal Ultrasonography; ICD-10, International Classification of Diseases, Tenth Revision.
Demographic data, clinical characteristics, laboratory parameters, the MSK-US result, and intraoperative findings were all obtained. Specifically, the following data points were extracted: age, sex, date of admission and discharge, length of symptoms before consult, history of trauma, history of manipulation, muscle group affected, comorbidities, clinical findings (presence of fever [≥37.8°C], presence of tenderness, swelling, redness, or warmth), admission and discharge laboratory parameters (white blood cell [WBC] count, ESR, and CRP), and the surgical procedure with intraoperative or histopathology findings. Presence of purulent material as described in the intraoperative findings or suppurative inflammation under histopathology findings was noted. Manipulation is defined in the study as manual manipulation/deep massage of the tender area by a local healer or a family member to supposedly alleviate symptoms; this is a popular form of traditional medicine in the study setting. This is done with or without a liniment where the liniment is either a homemade tincture using herbal leaves or an over-the-counter liniment. The number of manipulation sessions differ and may include areas distant to the affected area. Data extracted on the MSK-US finding only indicated whether the case is positive or negative for pyomyositis, relying solely on the written results as seen in the medical chart. Other concomitant pathologies noted during sonographic exams were tallied as well. All MSK-US reports in this study were produced by either one of two consultants with at least 5 years of experience in MSK-US. No review of sonographic images was done in this study. A Microsoft Excel 2013 file was used as the data collection file format. The same program was used for statistical analysis which included frequency, mean, and standard deviation.
For assessing the diagnostic accuracy of MSK-US, a 2 × 2 contingency table was used to determine the sensitivity, specificity, and likelihood ratios. For surgically treated cases, the MSK-US result was compared with intraoperative findings, while for conservatively treated cases, the MSK-US result was compared with laboratory parameters.
Results
The results represent the two data sets combined, resulting in a total of 122 cases (57 with surgery, 65 without surgery). The 122 cases represent cases that underwent an MSK-US procedure.
Demographic and Clinical Characteristics
Table 1 shows a high prevalence of trauma as well as manipulation. For cases without trauma, 53% underwent manipulation of the tender area which may be interpreted as a form of trauma. Accordingly, this increases the prevalence of trauma to 89% of the sample size. It is important to note that in all cases, the area of trauma corresponded to the symptomatic area on admission. Inflammatory signs were vastly prevalent at 99% versus documented/undocumented fever. Tenderness, redness, swelling, and warmth may or may not have occurred simultaneously at the time of admission.
Demographic and Clinical Characteristics.
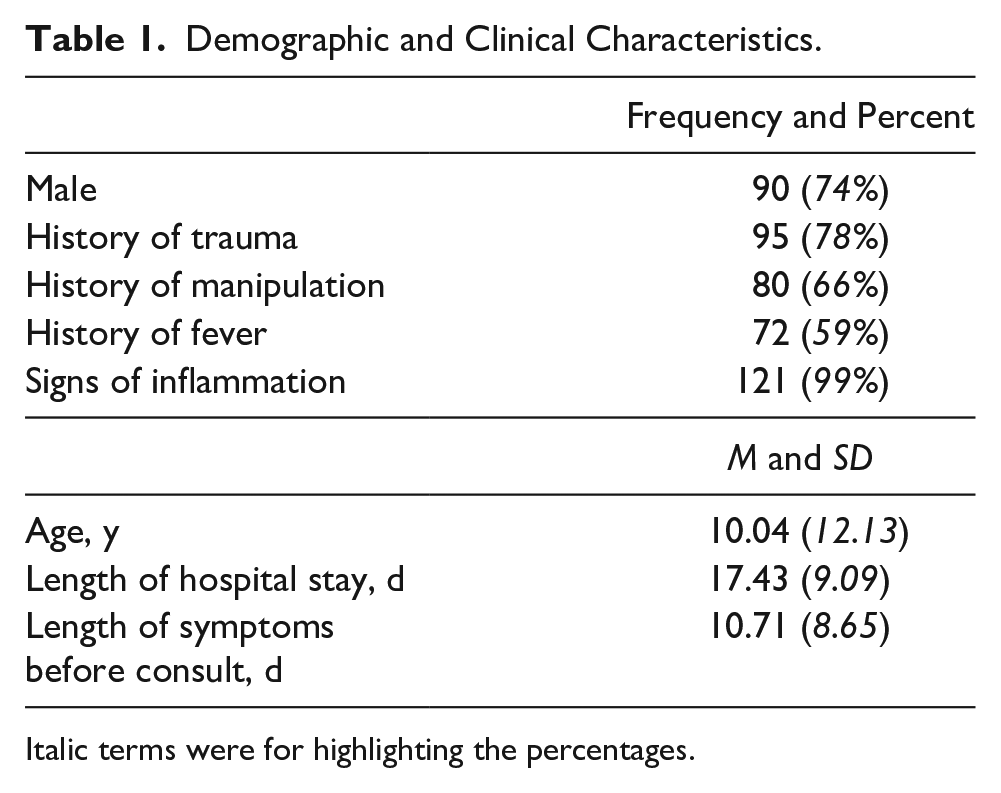
Italic terms were for highlighting the percentages.
Only three cases (two hypertension and one diabetes mellitus) had listed lifestyle co-morbidities which reflect the young age group primarily affected by the disease. In one case, a 26-year-old had a comorbidity of pulmonary tuberculosis diagnosed during hospital stay.
Muscles With Pyomyositis
A total of 117 cases were diagnosed using MSK-US to have pyomyositis. Table 2 tallies individual muscles affected wherein one case may have more than one muscle affected. When tallied as muscle groups, the quadriceps (26%), gluteals (24%), and shoulder girdle (20%) muscle groups were the most commonly affected.
Individual Muscles Affected by Pyomyositis Diagnosed Using MSK-US, n = 117.
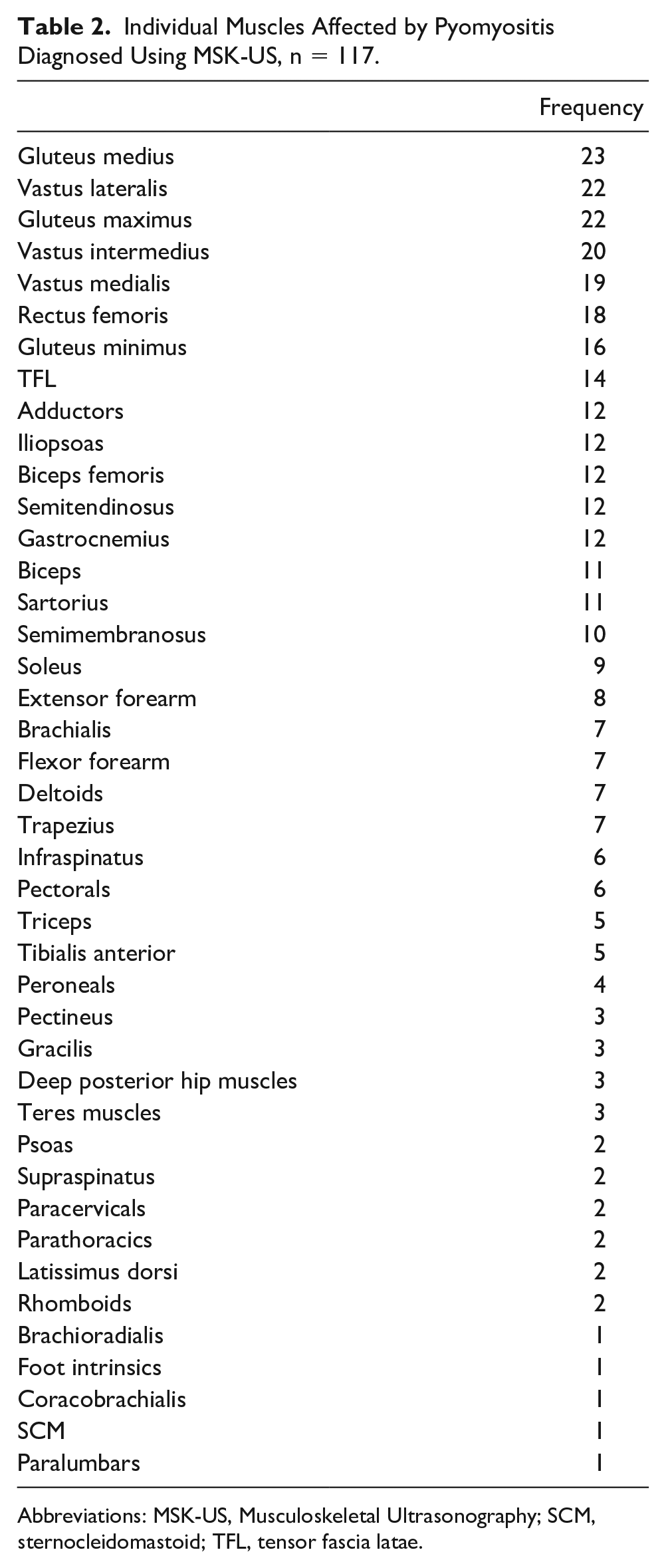
Abbreviations: MSK-US, Musculoskeletal Ultrasonography; SCM, sternocleidomastoid; TFL, tensor fascia latae.
Of the 117 cases diagnosed with pyomyositis, 22 cases had a single muscle affected and 44 cases had a single muscle group affected. Fifty-one (51) cases had multiple muscle groups affected where the common pattern observed was a simultaneous affectation of adjacent muscle groups. In six of the 51 cases, separate and distant muscle groups were affected simultaneously.
Laboratory Parameters
Admission and discharge WBC, ESR, and CRP values are shown in Table 3.
Admission and Discharge Laboratory Parameters.
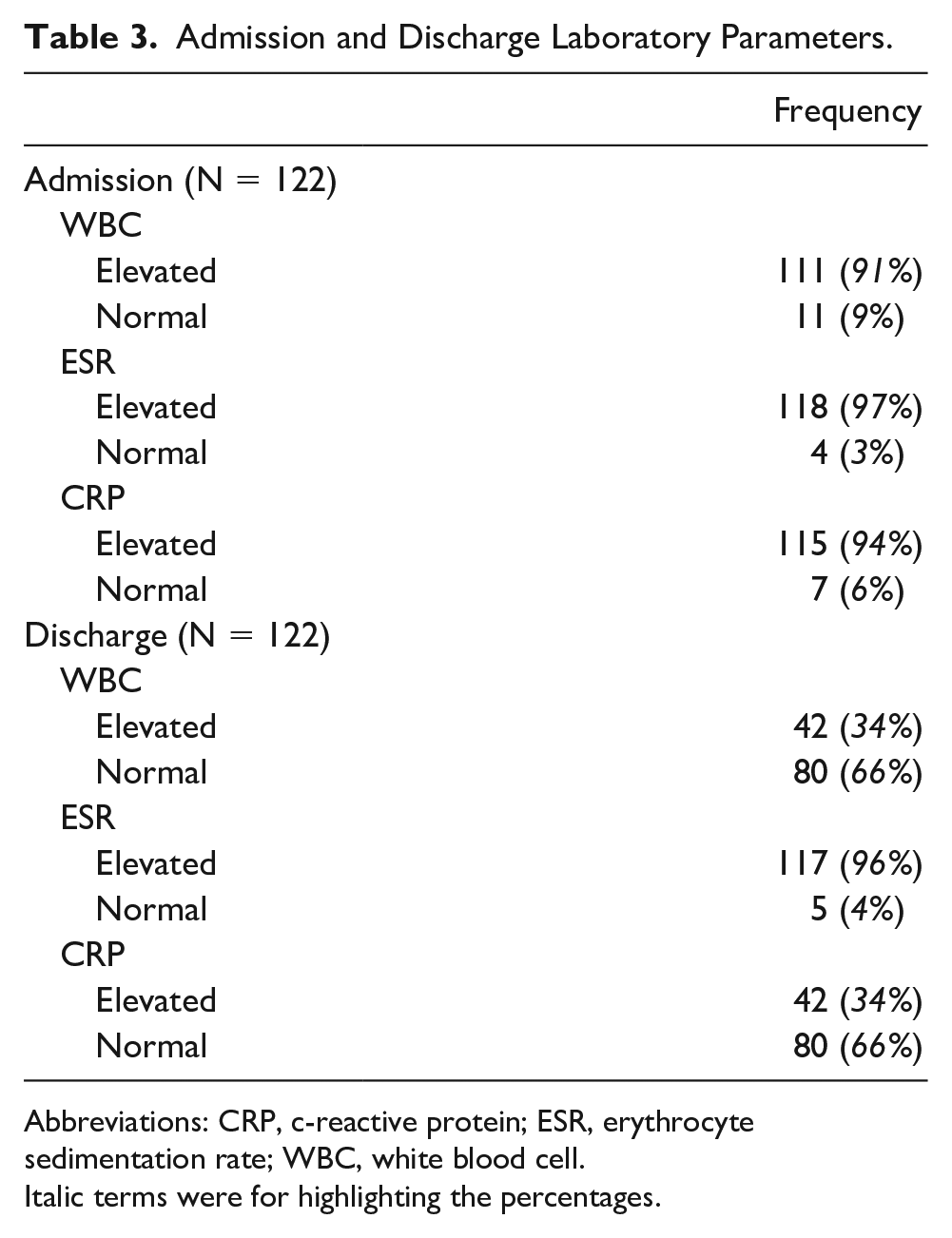
Abbreviations: CRP, c-reactive protein; ESR, erythrocyte sedimentation rate; WBC, white blood cell.
Italic terms were for highlighting the percentages.
Table 4 displays the same laboratory parameters, however, with further consideration to whether the results normalized, displayed a decreasing trend since admission, no change from normal admission status or worsening. No case was observed to have started with elevated values then discharged with an increasing trend. Improved cases are patients with either a normal value or a decreasing trend on discharge. Consequently, all three parameters have comparable improved cases tallies of 111 for WBC, 118 for ESR, and 115 for CRP. Each laboratory parameter had two cases discharged with elevated results. The elevated values in these six cases occurred separately. These six cases were discharged as improved cases of pyomyositis since the other two parameters have either normalized or showed a decreasing trend that indicated an improving case, and in addition, parameters were interpreted as a whole together with improving clinical signs prior to discharge.
Admission and Discharge Laboratory Parameters.
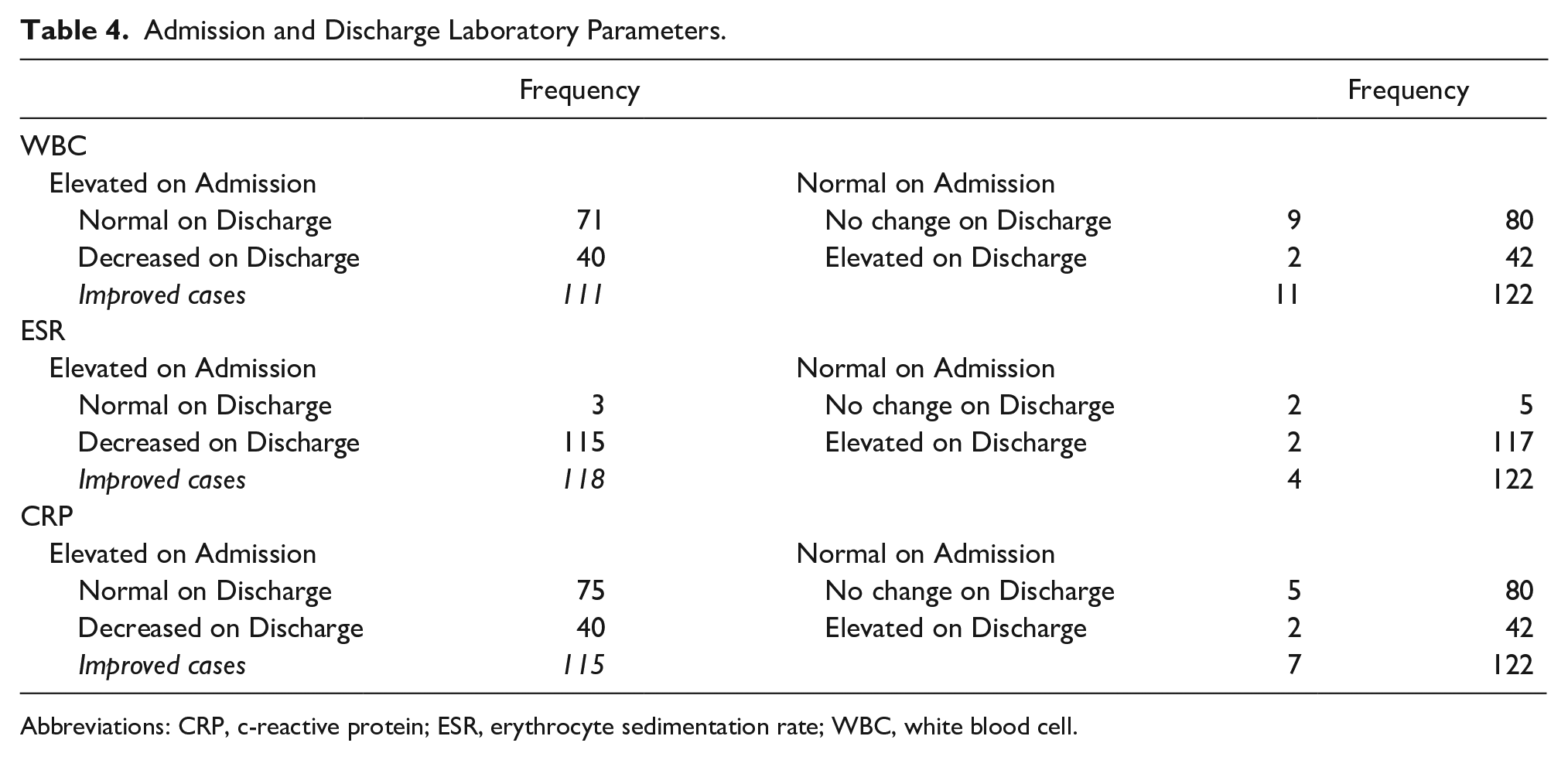
Abbreviations: CRP, c-reactive protein; ESR, erythrocyte sedimentation rate; WBC, white blood cell.
Surgical Procedures
Fifty-seven (57) cases, representing 47% of all cases, underwent a surgical procedure with all undergoing incision and drainage except for one case where percutaneous aspiration was done. Fifty-four (54) cases displayed intraoperative findings ranging from purulent to seropurulent discharge with 46% having necrotic tissue described. These intraoperative findings, as a reference standard, were confirmatory for pyomyositis. Three (3) cases were negative for discharge or gross muscle pathology intraoperatively, hence were considered negative for pyomyositis. Only nine out of 54 cases with gross pyomyositis were sent for histopathology evaluation, all of which had confirmation of pyomyositis where findings ranged from acute to chronic suppurative inflammation or acute to chronic inflammation and with or without presence of granulation tissue.
Other Pathologies
Cellulitis was noted in 28 cases and was the most common pathology diagnosed together with pyomyositis on MSK-US scanning. Other pathologies in decreasing frequency were hip effusion (8), chronic osteomyelitis (5), elbow effusion (4), knee effusion (4), knee bursitis (2), and subcutaneous abscess (1). All pathologies seen were adjacent to the muscle group with pyomyositis.
Diagnostic Results
Shown below are two separate 2 × 2 contingency tables to assess the diagnostic accuracy of MSK-US. Important to note that an MRI result was to be included as the imaging reference standard for this study; however, as data were collated, only one case underwent an MRI, hence its exclusion in the data analysis.
Based on Table 5, the sensitivity of MSK-US for surgically treated cases was 100% (95% confidence interval [CI] = 93%–100%). Specificity was 0% (95% CI = 0%–71%). The positive likelihood ratio was 1. The negative likelihood ratio was undetermined, whereas predictive values were not included as the sample size did not reflect disease prevalence and furthermore, no data on local disease prevalence were available. For conservatively treated cases, the sensitivity of MSK-US for pyomyositis was 92% (95% CI = 82%–97%). Specificity was 0% (95% CI = 0%–84%). The positive likelihood ratio was 0.92. The negative likelihood ratio was undetermined, whereas predictive values were also not applicable. All five cases with negative MSK-US findings improved without undergoing surgery. The laboratory parameter tallies shown in Table 5 are for WBC and CRP values as both had identical tallies. The tally for ESR values had 59 true positives and one false positive; nevertheless, the resulting calculations revealed the same percentages and ratio.
Combined Contingency Tables Showing MSK-US Result Comparison With Two Reference Standards, Intraoperative Findings (Surgically Treated) and Laboratory Parameter Improvement (Conservatively Treated).
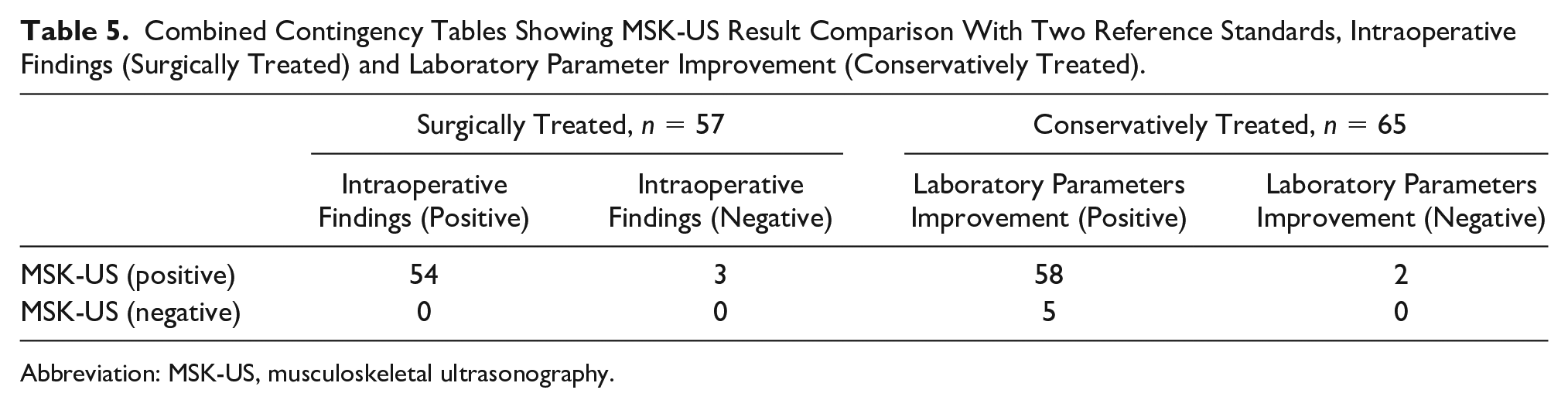
Abbreviation: MSK-US, musculoskeletal ultrasonography.
Despite deficiencies in the contingency tables that led to extreme values, it is worth noting that MSK-US was able to correctly identify abscess formation within muscle in 95% of cases that had surgery (54 out of 57 cases). For cases that underwent conservative treatment, MSK-US was able to correctly diagnose pyomyositis in 89% of cases (58 out of 65 cases).
Discussion
The demographic characteristics observed in the study including a high male prevalence and a predilection for pediatric patients reflect that of previous investigations on pyomyositis.2,3,4,14 However, male to female ratio differs between studies. The male to female ratio in this study was approximately 3:1 compared with other studies at 2:1 2 and 1.5:1. 4 Most of the pyomyositis case reports encountered on literature review also reveal the same trend of young male patients.6,9,11,13,16,17
Trauma with transient bacteremia has been reported to be one of the risk factors for infection to develop in generally resistant skeletal muscle. History of antecedent trauma to the affected muscle group ranges from 20% to 50% of cases in previous studies.1–6 In the study, antecedent trauma was present in 78% of cases; this increases to 89% if manipulation is included as a form of trauma. The pathogenesis of pyomyositis remains unclear, however is widely accepted to be hematogenous in origin. A review article by Chauhan et al 4 proposed that in a healthy state, the sequestration of iron by myoglobin imparts the resistance of skeletal muscle to infection. However, when trauma occurs, iron is dislodged and now becomes available for bacteria to proliferate that consequently leads to pyomyositis. 4 The high prevalence of trauma observed in the study is seen as contributory to this proposed pathogenesis.
Fever is considered a feature of pyomyositis; however, its presence or absence and pattern is determined by the disease stage at presentation. The invasive stage usually presents with a variable fever, whereas the suppurative stage is characterized by high fever.2,4 Study results showed that fever was present in 59% of cases compared with signs of inflammation which were present in 99% of cases. Important to note that a few cases presented with only one or two of the four inflammation signs. As such, a combination of fever and local signs of inflammation should warrant consideration of pyomyositis as a differential.
The mean length of symptoms before consult of 10.71 days corresponds to when previous authors describe the transition from the invasive stage to the suppurative stage. Most patients consult and are diagnosed with pyomyositis in the suppurative stage which ranges from 10 to 24 days from the invasive stage.1,2,4 Previous studies described differing mean duration of symptoms before hospitalization of 24, 12, and 6.2 days. 2 Despite the variability of results across studies, the majority fall within the described suppurative stage range. These results suggest that knowledge of disease presentation and staging is important when considering a diagnosis of pyomyositis. The mean length of hospital stay of 17.43 days also corresponds to the length of intravenous antibiotics with oral antibiotics prescribed on discharge as take-home medication for another 1 or 2 weeks depending on the initial clinical severity and patient status on discharge. The study mean of 17.43 days of intravenous antibiotic treatment fall within what two case series describe where the antibiotic treatment duration ranged from 2 to 6 weeks, beginning initially with intravenous antibiotics then transitioning to oral antibiotics upon discharge.2,12 Despite the average range of treatment duration reported, there is still no specific treatment duration established for pyomyositis.1,2,7
The muscles involved in this study, either taken individually or as a group, are similar to previous reports where the large muscles of the lower limb are commonly affected, with the quadriceps and gluteus muscles the two most commonly affected muscle groups.1,2,5–7 The upper limb muscle is also often affected, with the pectorals being commonly encountered; however, in this study, the biceps muscle was the most commonly affected upper limb muscle. Most of the pyomyositis cases affect a single muscle group, with percentages ranging from 60%1,4 to 75%. 3 The study results, though comparable, showed a slightly lower percentage, with 56% of cases showing the same affectation pattern. When comparing occurrences of multiple muscle group involvement, the study result was slightly higher at 44% compared with previous studies that report it only as high as 40%.1,4
All MSK-US diagnoses of pyomyositis in this study were guided by sonographic features that have been previously described. The appearance of muscle tissue with suspected pyomyositis corresponds to either the invasive or suppurative stage. In the invasive stage, diffuse muscle swelling with edema is seen, where edema can present as diffuse muscle hyperechogenicity with or without localized ill-defined hypoechogenicity and diffuse hyperemia.15,22 Figure 2 shows a case of pyomyositis in the invasive stage.
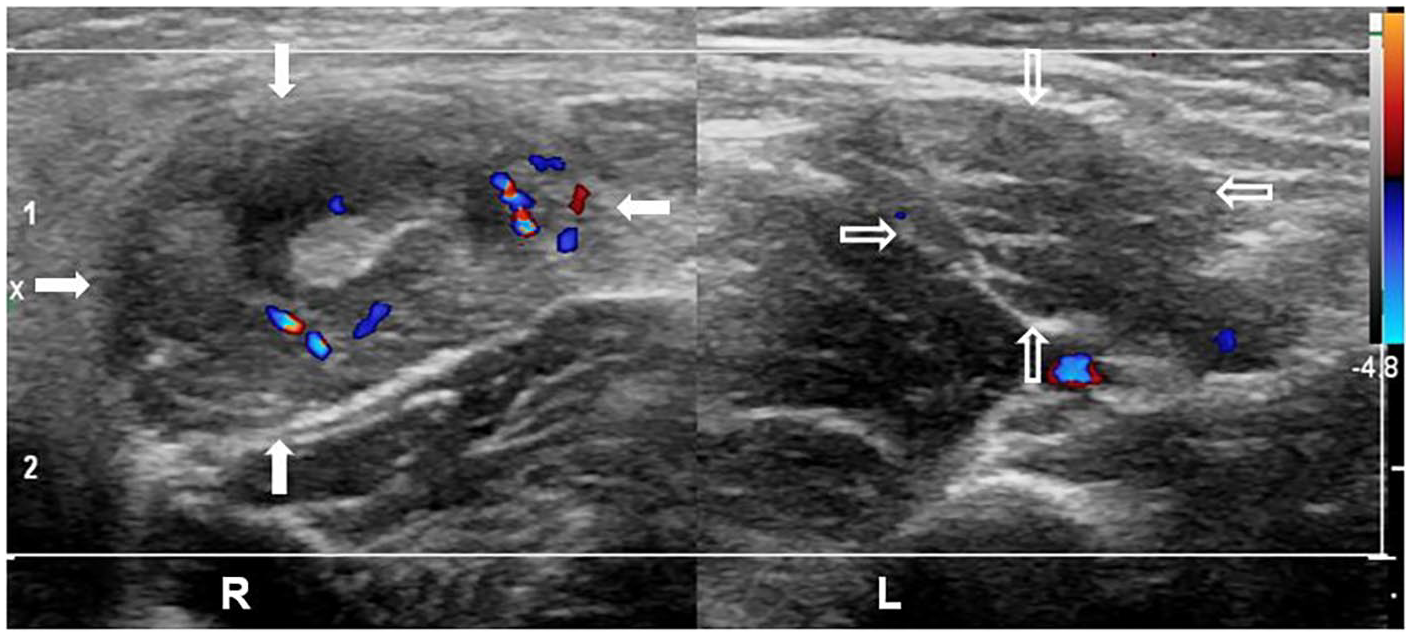
Pyomyositis, invasive stage, short-axis view of right adductor longus. A 3-year-old boy presenting with localized swelling, tenderness, and erythema at the right proximal antero-medial thigh with history of blunt trauma and manipulation. Sonography shows an enlarged and edematous right adductor longus (arrows) with diffuse hyperechogenicity and sparse hypoechoic areas. Color Doppler shows diffuse hyperemia. Sonopalpation showed no movement of fluid or debris. The left side shows the unaffected adductor longus (open arrows) size and echotexture.
As the disease progresses into the suppurative stage, a muscle abscess forms. Abscess echogenicity varies from hypoechoic to isoechoic or hyperechoic depending on location, maturity, and contents, with an associated posterior acoustic enhancement that is indicative of a fluid component. Abscess margins may be well circumscribed or blend with the surrounding tissues with color Doppler imaging revealing hyperemia of these margins or the adjacent surrounding tissue.15,22 Dynamic evaluation of the soft tissues via sonopalpation, which is unique to sonography, is useful to reveal motion of the liquefied purulent material.7,15 Figures 3 and 4 show pyomyositis in the suppurative stage.
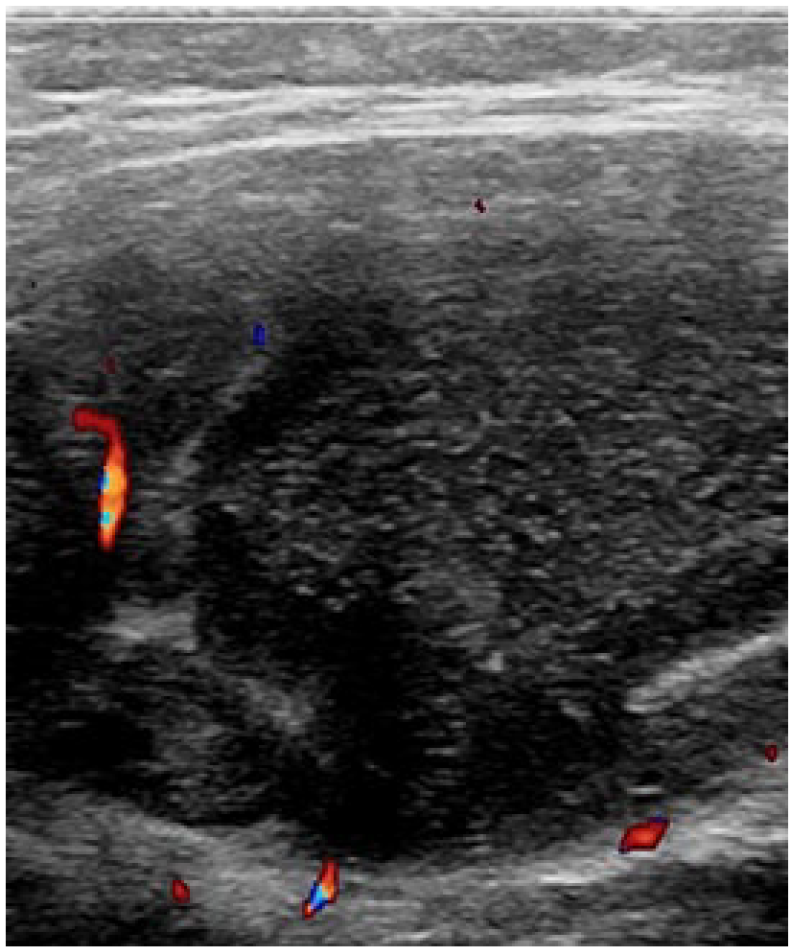
Pyomyositis, suppurative stage, short-axis view of right gluteal muscles. A 4-year-old boy presenting with diffuse swelling, tenderness, and erythema at the right gluteal and paralumbar area with history of fall and manipulation. Ultrasound shows a large intramuscular predominantly hypoechoic complex fluid collection with punctate hyperechoic echoes affecting the gluteus maximus and medius. Adjacent muscle fibers appear echogenic and edematous with hyperemia. Color flow is not present within the fluid collection. Sonopalpation showed movement of fluid and debris.
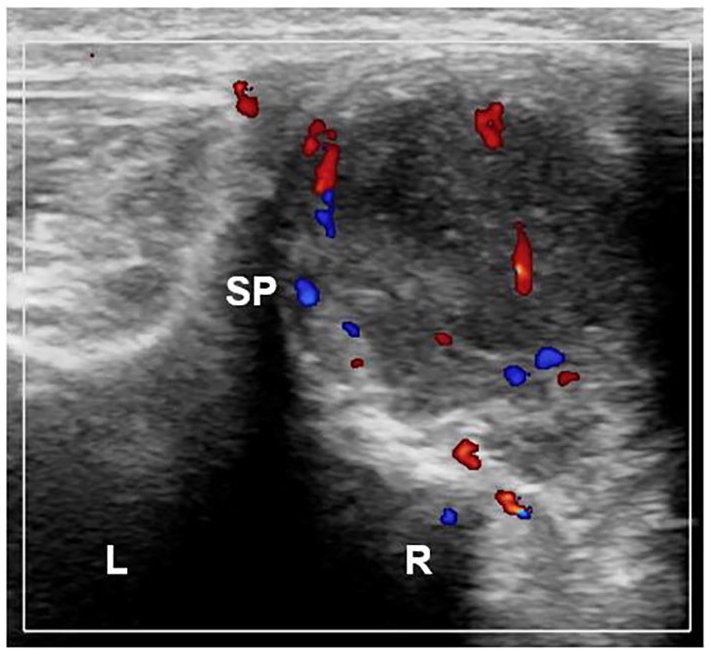
Pyomyositis, suppurative stage, short-axis view of right paralumbars. The same patient described in Figure 3 is shown here. Ultrasound shows an intramuscular complex fluid collection affecting the right paralumbars. This collection was seen communicating with the previously described gluteal complex fluid. Adjacent muscle fibers appear echogenic and edematous with hyperemia. Sonopalpation showed movement of fluid and debris. The left side shows the unaffected paralumbar muscle size and echotexture. SP, spinous process.
The laboratory parameters in this study showed a commonality among WBC, ESR, and CRP on admission where most of the cases had elevated values; on discharge, only WBC and CRP were comparable in the tallies of normalized values. The high prevalence of elevated ESR values on discharge reflects the normal physiology of elevated ESR where it remains elevated for weeks after resolution of inflammation, whereas CRP normalizes within 3 to 7 days. 23 The timing of normalization for both reactants varies per type of infection, but regardless of the infection severity and type, CRP normalizes earlier than ESR.
The results shown in Tables 3 and 4 reflect treatment practices in a low-resource setting wherein the decision to discharge a patient does not solely rely on attaining normal laboratory parameters. Maintaining a clinical eye in conjunction with equitable use of resources remains an essential skill in this setting. In summary, both tables showed that most of the cases had elevated WBC (91%), ESR (97%), and CRP (94%) values on admission. On discharge, the same percentages were observed per parameter as improved cases. The high prevalence of leukocytosis, elevated ESR and CRP on admission were all reported by previous studies; however, these studies also maintain the nonspecificity of laboratory findings.1,2,4,5,7 Despite its nonspecificity in diagnosing pyomyositis, these parameters are considered valuable as an adjunct to clinical judgment and in monitoring response to treatment.
The decision to proceed with surgical drainage of an abscess in pyomyositis depends on the disease stage at presentation.2,6 Forty-seven percent (47%) of cases underwent drainage which suggests a case admitted in the suppurative stage of the disease pending confirmatory intraoperative findings. All surgical procedures done in this study were done after the release of MSK-US results, where presence or absence of an abscess was described. Absence of an abscess in scanning suggests a case presenting in the invasive stage. These cases represent those that underwent conservative treatment with intravenous antibiotics. It is important to note, however, that not all cases with MSK-US determined abscesses underwent drainage in this study as the decision to proceed with surgical drainage was based as well on present clinical and laboratory status and ultimately on the discretion of the attending physician. Comegna et al 2 mentioned that in many series, despite abscess formation in some patients, neither surgical nor percutaneous drainage is needed. Regardless of current practices, the role of imaging, particularly MSK-US, in guiding management remains unchanged and vital. Imaging functions in establishing a working diagnosis, disease staging, and treatment planning. Early recognition and initiation of proper management leads to faster recovery and better outcomes. In addition, prompt diagnosis followed by early initiation of intravenous antibiotics can prevent abscess formation and avoid surgical drainage.2,5
Histopathologic evidence remains the gold standard for diagnosing pyomyositis. Both gross evidence of pus or muscle biopsy showing edematous fibers and suppurative inflammation are confirmatory. 4 In the study, only nine out of 54 cases with gross pyomyositis had samples sent for histopathologic study. These nine cases represent physician discretion where either doubtful intra-operative findings or absent macroabscess was encountered. This also reflects the study hospital practice and low-resource setting wherein histopathologic study is not routinely done especially for cases that already revealed gross pus formation.
The other pathologies noted during MSK-US scanning reflect the common differential diagnoses grouped together with pyomyositis. The presence of these pathologies can indicate progression of pyomyositis, a coexisting pathology or a preexisting pathology. Progression can be via direct extension in the form of cellulitis, subcutaneous abscess, and osteomyelitis. Progression can also take the form of reactive inflammation of adjacent joints manifesting as effusion, bursitis, or septic arthritis. An impression of chronic osteomyelitis was made when abscess formation was seen adjacent to bony cortices with periosteal reaction or cortical irregularities. These represent cases with either delayed consults or a misdiagnosis from other clinics. All five cases with a consideration of chronic osteomyelitis had a mean length of symptoms before consult of 32.50 days, compared with the study mean of 10.71 days. Development of osteomyelitis is one of the complications of a delayed diagnosis. The presence of other pathologies identified by MSK-US reinforces its utility not only in ruling out differentials but also in indicating the need for further imaging especially in osteomyelitis or an adjunct diagnostic investigation such as joint fluid analysis in cases with effusion.
Testing the diagnostic accuracy of MSK-US was the general objective of the study. However, when compared with intraoperative findings, a lack of false negatives and true negatives was encountered that led to extremes of sensitivity (100%) and specificity (0%). The unlikely results were attributed to inherent limitations of a retrospective study and the small sample size. For cases that underwent conservative treatment, a tally for false negatives was observed; however, there was still a lack of true negatives. The sensitivity in this case was 92% with the specificity remaining at 0%. The sensitivity and specificity of MSK-US for detecting abscesses in deeper soft tissue and muscles, in particular pyomyositis, have not been described. Previous studies have established the diagnostic strength of MSK-US for superficial soft tissue abscess formation. These studies showed different values, sensitivity 98% and specificity 88%, 18 96.7% and 85.7%, 19 97% and 83%, 20 and, 65.9% and 94%, 21 respectively. Comparing those with the study results, the calculated sensitivity of 92% (vs improved laboratory parameters) and 100% (vs intraoperative findings) was comparable with the sensitivity established by three of the four studies. Although the high sensitivity values were for superficial soft tissues, the study points to the potential strength of MSK-US for identifying pyomyositis. The higher measures obtained by comparison with intraoperative findings (surgical cases) versus laboratory parameters (conservative cases) points to the relative strength of sonography in detecting abscess formation or fluid collection in the suppurative stage of pyomyositis. 15 Cases that present in the invasive stage are also the cases that are treated conservatively. At this stage, sonography appears to have less ability to establish pyomyositis when compared with its ability to detect an abscess in the suppurative stage as results have shown in this study. Nevertheless, both sets of results still represent high values and are considered preliminary at this point.
Determining the true diagnostic strength of MSK-US was undermined by inherent data deficiencies; however, the utility and diagnostic value of sonography was clearly observed in the study. Only one case had an MRI done which reflects a common problem in low-resource settings, despite MRI remaining as the imaging gold standard for pyomyositis.2,6,7,13,14 The study results have shown that sonography has functioned not only as an initial screening tool but also as the sole imaging choice when managing pyomyositis. Easy access, a shorter procedure time and lower cost are inherent advantages of this modality. The utility of sonography is seen in its ability to exclude differentials, establish a diagnosis, and guide early initiation of treatment.
Limitations
A small sample size, presence of bias, data availability problems, and a retrospective design were the identified limitations. The small sample size was attributable to a combination of factors. These included record keeping and retrieval problems, pyomyositis management in the study hospital where MSK-US referrals are only beginning to become routine, and inherent referral system gaps. These resulted in a total of 204 cases that would have contributed to the quality of the results. The authors of the study are certain that case numbers will improve as attending physicians recognize MSK-US as a valuable tool. This outlook is encouraged by an increasing trend of MSK-US referrals since the availability of an ultrasound machine in the study hospital in 2015. Missing data and reliance on written data records were encountered in this study, both of which are inherent problems for retrospective chart reviews. The lack of interobserver data wherein only one performer of the MSK-US was involved affects the strength of the data obtained. In addition, being a retrospective study, the lack of exposure blinding and uncertainty as to how the scans were performed may have led to significant diagnostic bias. Deficiencies with sonographic image storage and retrieval were contributory to the exclusion of an interobserver interpretation comparison in the methodology.
Recommendations
A larger sample size is recommended to improve the validity of the results. Overall improvement of data retrieval and storage and establishment of a pyomyositis referral system is likewise needed. Incorporation of exposure blinding and implementation of interobserver comparison using sonographic images are warranted to eliminate bias and improve data quality. A prospective study design will best accommodate all recommendations for future studies.
Conclusion
Musculoskeletal ultrasonography is a valuable imaging modality for diagnosing pyomyositis. Its value is not limited to as primarily a screening tool but as a capable diagnostic imaging choice, particularly in low-resource settings. The results provide preliminary data on the strength of sonography, particularly in the suppurative stage of pyomyositis. However, further research is needed to determine the true diagnostic accuracy of sonography in pyomyositis.
Footnotes
Acknowledgements
The authors would like to acknowledge the Musculoskeletal Ultrasound Section of the Department of Physical and Rehabilitation Medicine and Medical Records Section of the Philippine Orthopedic Center for ensuring data access and availability throughout the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.