
Abstract
Sirenomelia is a rare, lethal congenital malformation of the fetus, typically characterized by the fusion of lower limbs and additional malformations involving the lumbosacral spine and urogenital and gastrointestinal tracts. We report a case of sirenomelia with anhydramnios detected during anomaly scan where the fetus had normal morphology of long bones of the lower limbs. There were associated abnormalities of the lumbosacral spine (caudal dysgenesis). The abortus had fused lower limbs, absent external genitalia and anal orifice, single umbilical artery, and Potter facies. We also highlight the interesting diagnostic challenges faced by us during this antenatal ultrasound. To our knowledge, this is the first case report of sirenomelia where the synchronous movement of lower limbs was a clue that led to the timely antenatal detection of this rare entity. This ultimately helped in perinatal counseling of parents to decide on termination of pregnancy.
With the diagnosis of sirenomelia, the fetus resembles a mermaid of Roman and Greek mythology. 1 It is a rare, usually fatal, congenital disorder typically characterized by the fusion of lower limbs, single umbilical artery, and anomalies of lower spine and urogenital and lower gastrointestinal tracts. Associated oligohydramnios or anhydramnios may lead to Potter facies and pulmonary hypoplasia. The incidence is about 1 in 60 000 live births 2 to 1.5–4.2 per 100 000 births. 3 About 400 cases of sirenomelia have been reported till 2017. 4 It is considered an axial mesoderm defect and a vascular developmental defect, and these are the two hypotheses on this syndrome. 5 This case study highlights how the evaluation of fetal lower limb movements led to in utero diagnosis of sirenomelia and was associated with a case of anhydramnios during the second trimester of pregnancy.
Case Report
A 24-year-old primigravida reported for an anomaly scan at a period of gestation (POG) of 27 weeks in a zonal-level government hospital. The first-trimester sonogram (at POG of 12 weeks) was for nuchal translucency (NT) and nasal bone (NB), which were unremarkable. The antenatal scan was performed on a GE Logic P5 ultrasound machine, with 3.5-MHz curvilinear and 3.0-MHz curvilinear 4D transducers, as well as on a Vivid T8 ultrasound machine with a 4.0-MHz curvilinear RS transducer. A 2D gray-scale sonogram revealed single live fetus with a composite ultrasound age (CUA) of 21 weeks and 3 days, coinciding with anhydramnios (see Figure 1).
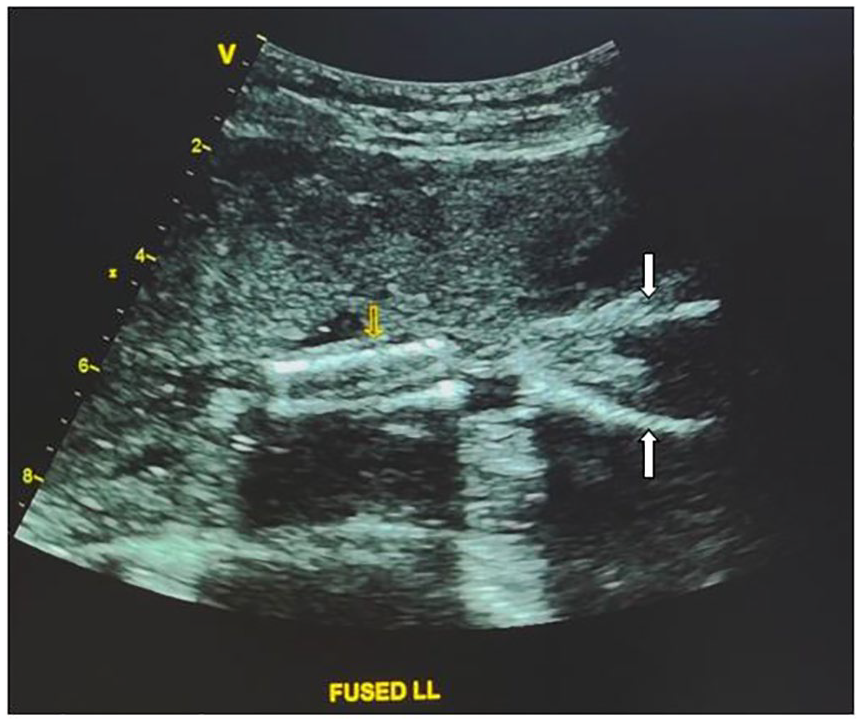
Gray-scale sonogram of the sirenomelic fetus with fused legs (yellow arrow at tibia, white arrows at femurs). The amniotic fluid is noted to be absent.
Due to anhydramnios, many fetal structures were not clearly visualized, including the lower spine. Also, there was a generalized restriction of fetal movements. The fetal head and thorax were grossly normal. The fetal heart showed normal situs, four chambers, and normal ventricular outflow tracts. The fetal kidneys were not clearly seen during sonography. The umbilical cord was evaluated with color and pulse-wave Doppler, and a single umbilical artery was discovered. The urinary bladder was not visualized (see Figure 2). No other gross spinal deformity was noted during the sonogram. Limb movements were restricted, which was expected to be due to anhydramnios. The upper limbs showed normal morphology of the long bones. The lower limbs were in close proximity in the long-axis plane of imaging (see Figure 1). The femur, tibia, and fibula were considered unremarkable. The lower limb movements were reduced, and whenever there was any movement, both lower limbs were moving simultaneously as a single unit. The targeted and specialized anomaly sonogram was performed twice, over the next 4–5 hours. During each sonographic imaging session, about one to two sporadic, synchronous flickering movements of the lower limbs were noted.
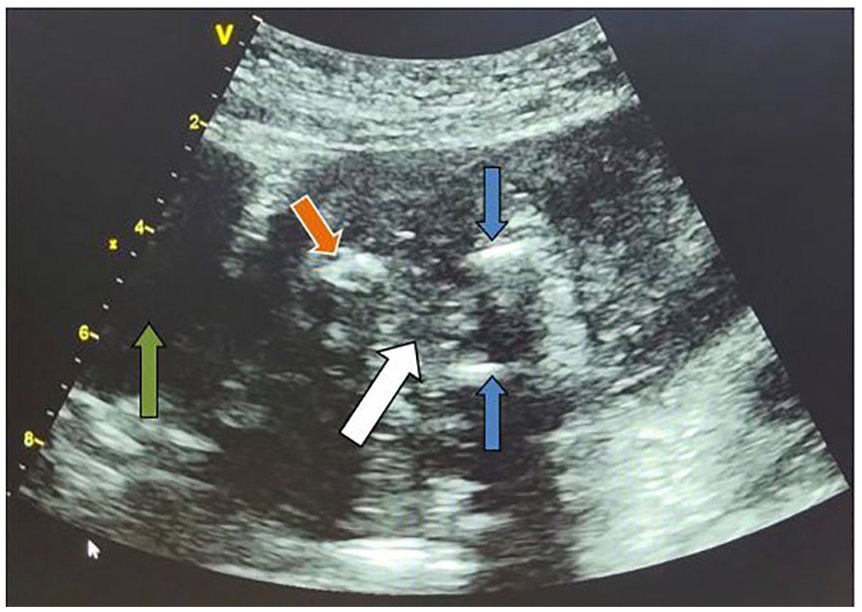
Axial sonographic image of the sirenomelic fetus with fetal sacrum (orange arrow) toward maternal urinary bladder (green arrow), nonvisualization of fetal urinary bladder at expected location (white arrow), and partial visualized femurs (blue arrows).
Finally, the fetus was determined to have a single umbilical artery, absent urinary bladder, and fusion of both lower limbs. The 3D sonogram was not of additional imaging assistance due to anhydramnios. The patient presented for hospital admission after a few days; the antenatal sonogram was repeated, and the same anomalies were confirmed. There was no evidence of diabetes mellitus, tobacco use or maternal fever during the first trimester. Perinatal counseling was provided to the parents, and a written informed consent was obtained for mid-trimester medical delivery.
The fetus weighed 630 g and had fused lower limbs (see Figure 3). The feet were inverted with partial fusion at the lateral aspect. The right foot had three toes and the left foot had four toes. External genitalia were absent and there was a small orifice at the expected site of genitalia. An anal orifice was absent. The left hand was flexed and externally rotated. The fetal face had a typical appearance of Potter facies (flattened nose, low set ears, micrognathia) (see Figure 3). The radiograph of the fetus (see Figure 4) revealed normal morphology of the shafts of femur, tibia, and fibula on both sides. There was a noted continuous soft-tissue covering on both legs consistent with the clinical appearance of a fused limb. The lumbosacral spine (see Figure 5) had multilevel segmentation anomalies, at the lower lumbar spine, which included hemivertebra L1 (left). This was accompanied by fusion of L1 with T12, hemivertebrae L3 (right) and L4 (left), and widely separated bifid segments of L5. Sacral (S)1 appeared to be fused with its lateral arches, and a triangular distal sacral segment was seen. The findings of the fetal thorax were that 13 ribs were found on each side. This was seen with bilateral complete cervical ribs (C7 vertebra level). The histopathologic examination of placenta was unremarkable. The karyotyping of the parents was completed subsequently, and it was also unremarkable. Due to cultural constraints, an autopsy of the fetus could not be done.
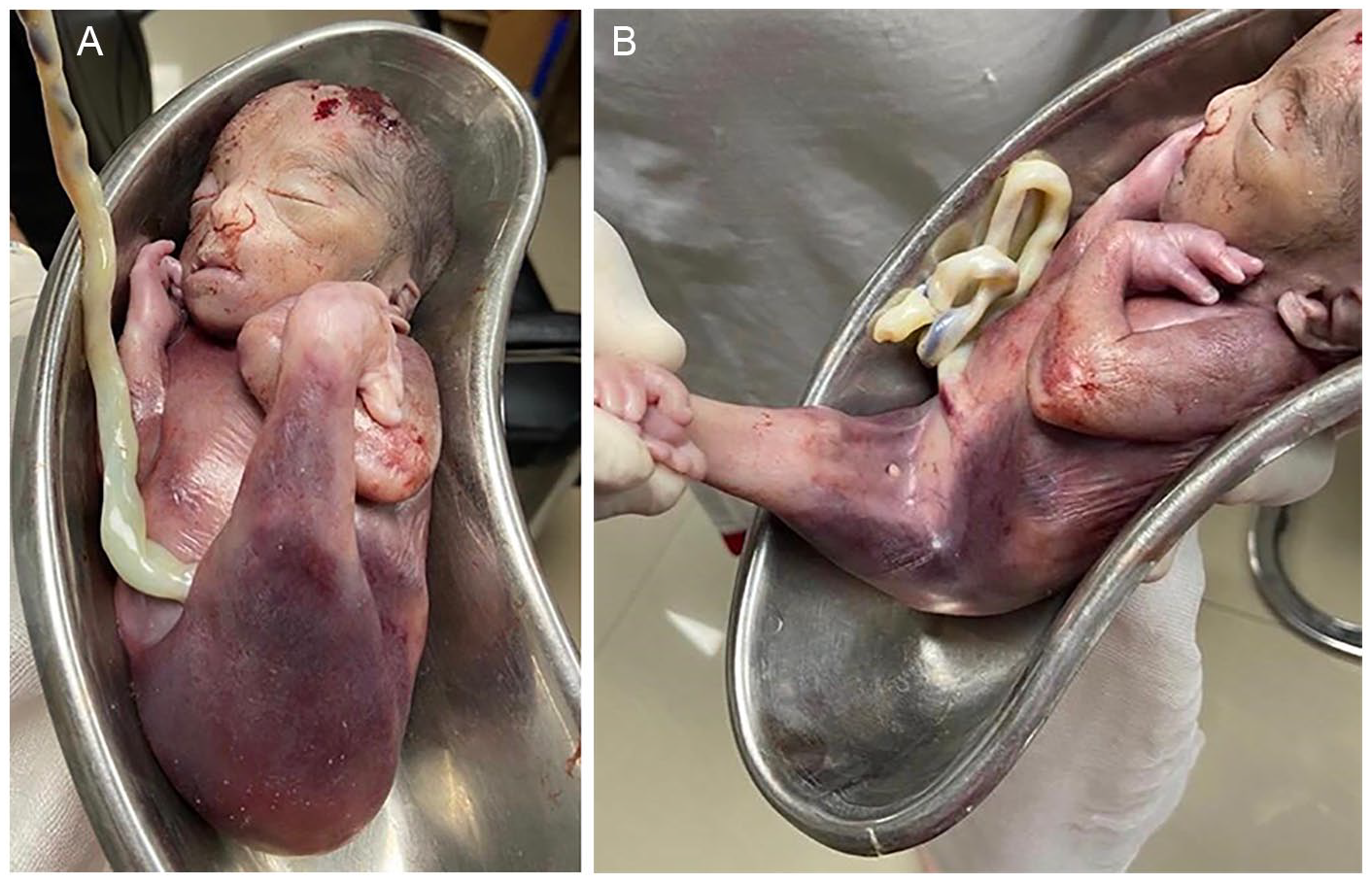
Postdelivery photographs of the fetus demonstrate fused legs, absent genitalia, absent anal orifice and Potter facies.
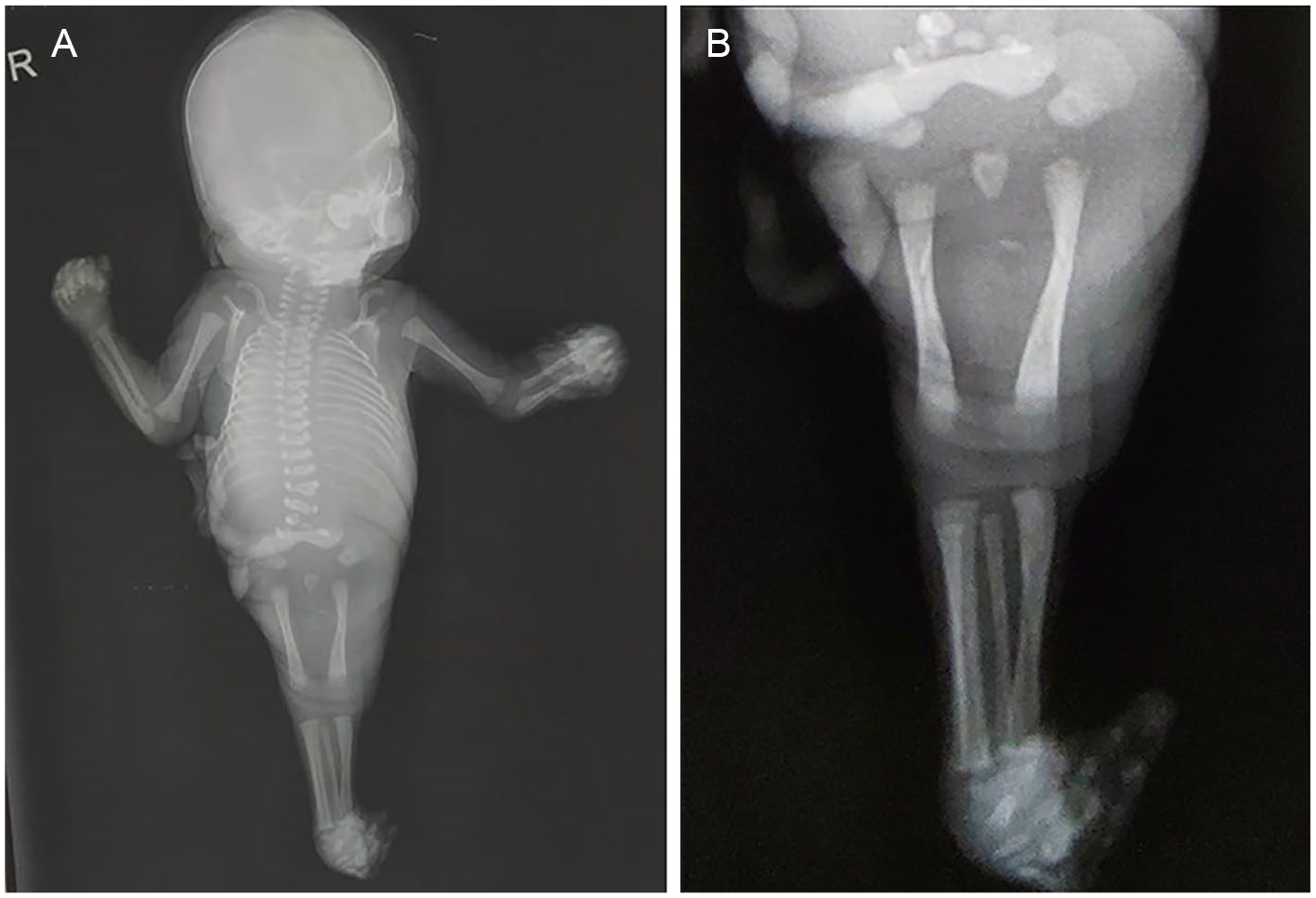
Postdelivery radiographs of the fetus demonstrate the following. (A) The fusion of soft tissues of lower limbs, distinct femurs, tibia and fibula, and bilateral 13 ribs. (B) The right fibula superimposed on right tibia, and poorly demarcated and crowded feet bones.
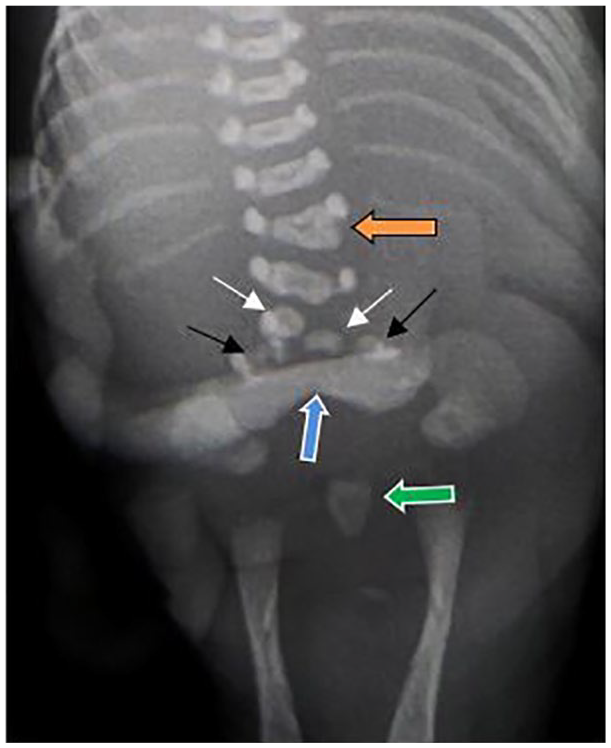
A radiograph that demonstrates hemivertebra fusion with T12 (orange arrow), hemivertebrae (white arrows), spina bifida L5 (black arrows), suspected sacral ala (blue arrow), and distal sacrum (green arrow).
Discussion
Sirenomelia was first described by Rocheus and Palfyn between 1542 and 1553. 1 The etymology of the word “siren” is not clear. It might have originated from Greek words like seira (rope) or seirazein (to bind—as sirens “bind/enchant” sailors). 6
Two main hypotheses have been suggested for sirenomelia pathogenesis. 5 First is the axial mesoderm hypothesis that suggests that sirenomelia arises from blastogenesis defect. Second is a vascular hypothesis that suggests that a single umbilical artery is remnant of vitelline artery. This would result in a diversion of blood flow away from the caudal part of the fetus and cause vascular steal syndrome. There has been a noted increased risk for sirenomelia in younger and old maternal ages (under 20 and over 40 years). 7 In the present case, the mother was 24 years old. This syndrome has a strong association with maternal diabetes mellitus. 8 Haloperidol, vitamin A, and heavy metals, such as lead and cadmium, have also been mentioned as causative agents. 9 There was no association of any those factors that could be established in the present case. It was also important to note that the karyotyping of parents was unremarkable.
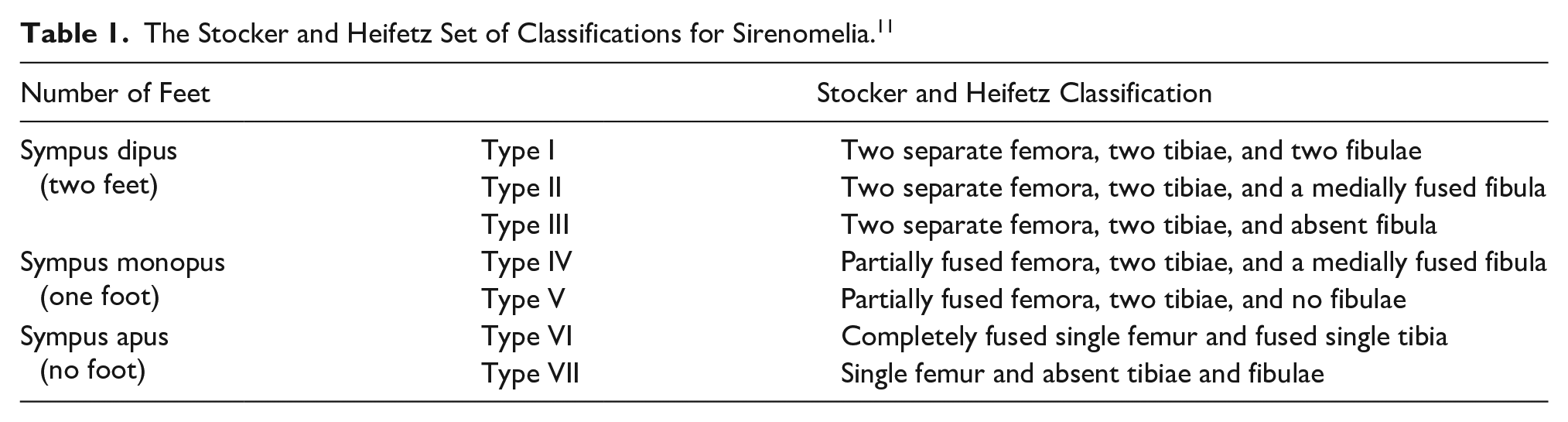
Depending on the number of feet, sirenomelia was classified into three types: sympus apus (without feet), sympus monopus (one foot) and sympus dipus (two feet). 10 This case represents sympus dipus, as the feet were partially fused. Stocker and Heifetz classified sirenomelia into seven varied types (see Table 1). 11 In type 1, there are two separate femurs, two tibiae, and two fibulae. A type II case has two separate femurs, two tibiae, and a medially fused fibula. In type III, there are two separate femurs and two tibiae, but the fibula is absent. A type IV sirenomelic fetus has partially fused femurs, two tibiae, and a medially fused fibula. In type V, there are partially fused femurs and two tibiae, but no fibulae. Type VI includes a completely fused single femur and fused single tibia. Type VII is considered the most severe form of sirenomelia, where only single femur is present and tibiae and fibulae are absent. The present case would be properly classified as type 1. Additional findings from this fetus were three toes in right foot and four toes in left foot.
The Stocker and Heifetz Set of Classifications for Sirenomelia. 11
On sonography, at POG of 21 weeks, the sacral vertebrae should be visualized till the S4 level. 12 In this case, at POG of 27 weeks (and CUA of 21 weeks), some part of sacrum was seen, but due to anhydramnios, anatomic details could not be ascertained. The concept of sirenomelia with caudal dysgenesis was proposed to be the most severe form of caudal regression syndrome by Thottungal et al. 13 The present case is also an example of sirenomelia, with caudal dysgenesis including multiple bony anomalies of the caudal spine and sacrum.
The associated anomalies that are usually found in sirenomelia are absent genitalia, absent anal orifice, dysgenetic/absent kidneys, absent urinary bladder (if kidneys are absent) and Potter facies. 10 This case study also had all the findings listed above. Taori et al 14 described a sirenomelic fetus delivered to a 22-year-old primigravida, and the fetus had 13 ribs. The presence of crowded ribs, cervical ribs, and fused ribs has also been mentioned in the literature.15,16 In this case also, there were 13 ribs on each side with bilateral cervical ribs. Further evaluation of a well-formed sacral ala S1, in such an early antenatal period, could not be done without an autopsy. Another possibility for this radiographic appearance could be due to soft-tissue density artifact of the proximal umbilical cord.
Amniotic fluid is secreted by the amnion until POG of 14–15 weeks. However, after POG of 16 weeks, the amniotic fluid is primarily renal in origin. In sirenomelia, oligohydramnios or anhydramnios is seen due to renal dysgenesis or agenesis. Hence, there are more chances of detection of sirenomelia in the first trimester due to the presence of adequate amniotic fluid. This becomes more difficult in the second or third trimester when the amniotic fluid becomes less or minimal. 17 Due to this, it becomes important to conduct a detailed sonographic fetal anatomic survey in the first trimester, as much as possible. At this gestational age, the presence of adequate amount of amniotic fluid should be able to provide good visibility of lower limb movements. Many cases of sirenomelia, with oligohydramnios, have been reported where the diagnosis was established after delivery. This case was diagnosed in the late second trimester of pregnancy. Yoshida et al reported a case of sirenomelia with 3D sonography but could not provide detailed sonographic images due to severe oligohydramnios. These authors also stated that detection of sirenomelia with oligohydramnios is very difficult if long bones of lower limbs are normal in morphology. 18
In this case study, three major issues were encountered. First, there was anhydramnios which led to poor visibility of many fetal parts, and 3D color sonography was not helpful in the diagnosis. Second, the long bones of both lower limbs (femur, tibia, and fibula) were normal in number and morphology. This resulted in no suspicion of any lower limb anomaly in the first instance. Third, the limb movements were already restricted due to anhydramnios; hence, it was difficult to separately evaluate the lower limbs. Unlike the upper limbs, the lower limb evaluation was not always easy, due to the natural position of close proximity of thighs. In this case, even though the lower limb movement was minimal, they were synchronous flickering movements, and hence there was a need to further evaluate this finding. The repeat sonogram resolved this diagnostic dilemma.
After comparing the guidelines, published by various international societies, a significant variation was noted in the recommendations adopted as minimally required for evaluating fetal limbs. 19 The International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) guidelines, as well as the National Health Service in the United Kingdom (NHS), the American College of Obstetricians and Gynecologists (ACOG), American Institute of Ultrasound in Medicine (AIUM), American College of Radiology (ACR), and Society of Radiologists in Ultrasound (SRU), promote assessing “fetal movement.” However, only ISUOG has this parameter included in the routine sonographic survey of fetal limbs. The remaining societies listed have not enlisted this parameter for routine screening of fetus.
Although sirenomelia is a rare entity, it should be included in differential diagnosis when severe oligohydramnios or anhydramnios is associated with renal anomalies and there is an inability to distinguish lower extremities, especially in the second trimester. 20 In this case, the kidneys were indistinct but the lower limb bones were normal in morphology. The authors were unable to find any case of sirenomelia, with normal lower limb long bones, along with anhydramnios, in the late second trimester. This diagnosis was made possible due to the absence of independent movements of lower limbs, from each other.
In a suspected case of sirenomelia, caudal regression syndrome is part of the differential diagnosis. Both conditions have few overlapping features on sonography, such as lumbosacral spine anomalies and genitourinary anomalies. However, there are few differentiating sonographic features. In caudal regression syndrome, amniotic fluid is usually normal or increased, 1 lower limbs are typically in a “cross-legged” position due to lack of movements, and the umbilical cord typically has two arteries. 21 Hence, during antenatal sonography, these features should be key in making the differentiation between these two conditions.
The histopathologic examination of placenta was found to be unremarkable, which negated the placenta as the cause. Despite extensive research, the authors could not find the histopathologic evaluation of placenta in cases of sirenomelia.
After delivery, in sirenomelia, the survival depends on the functionality of the urinary system. Antenatal sonography can reveal the presence of adequate amniotic fluid in the late second trimester and is suggestive of the functional urinary system. 17 Surgical management is not advisable in sirenomelia, as the survival rate is only 1% in the first week of life. 10 Timely antenatal detection of lethal anomalies, like sirenomelia, helps the parents to decide on the desired outcome of the pregnancy.
Conclusion
Sirenomelia is a rare and lethal multisystem congenital disorder. It can happen in a pregnancy without known risk factors, and its antenatal detection allows parents to decide on the desired outcome. If anhydramnios is detected during an anomaly scan, the lower limbs should not be reported as unremarkable based on only the number and normal morphology of long bones. In such cases, there should also be an evaluation of independent lower limb movements. If required, sonography should be repeated to resolve this diagnostic dilemma. In addition, during the first trimester sonogram, it is important to evaluate fetal anatomy as much as possible. This should include an evaluation of fetal limbs, as adequate amniotic fluid promotes this assessment during this gestational age.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.