
Abstract
Objective:
To assess the prevalence of carotid artery stenosis and risk factors in stroke patients of northeast India. This is a prospective hospital-based study on 157 first ischemic stroke patients of the region.
Method:
A total of 157 patients presenting with first ever sudden onset focal neurological deficit lasting for more than 24 hours due to acute ischemic brain infarction were selected, after excluding other causes of focal neurological deficit by imaging. All extracranial carotid arteries were evaluated with carotid ultrasonography. Forty-four patients also had computed tomography (CT) angiography of intracranial and extracranial arteries. Risk factors of stroke were recorded for each patient.
Results:
Only 8.92% patients had significant extracranial carotid artery stenosis. There was high prevalence of intracranial artery stenosis compared to extracranial artery stenosis in patients who had CT angiography. There was high prevalence of hypertension, dyslipidemia, and diabetes. Increased age and male sex were important factors associated with first ischemic stroke.
Conclusion:
The prevalence of significant extracranial carotid artery stenosis is low in northeast Indian patients with first ischemic stroke, indicating that it is not a major cause of ischemic stroke in this population. There may be high prevalence of intracranial artery stenosis compared to extracranial artery stenosis.
Stroke is one of the two major causes of death worldwide and the most important neurological disease in adults. 1 Stroke is characterized by a focal deficit of brain function, most commonly a hemiplegia, with or without signs of focal higher cerebral dysfunction (such as aphasia), hemisensory loss, visual field defect, or brain-stem deficit. 2 Stroke causes damage to the brain parenchyma by ischemic (from occlusion of blood vessels) or hemorrhage (from their rupture). Ischemic stroke can be caused by atherosclerosis, thrombosis, embolism, vasoconstriction, or from venous pathology. 3 Atherosclerotic disease in the arteries supplying the brain may often be the cause of a cerebral ischemic stroke. Carotid artery plaques are important causes of ischemic stroke. As the extracranial carotid artery is relatively easily accessible for surgery or stenting, there has been a lot of research into the pathological conditions affecting the carotid arteries.
The cumulative incidence of stroke in India ranges from 105 to 152 per 100,000 people per year. 4 Scarce data exist on the arterial disease distribution of arteries supplying the brain in the Indian population. A study by Padma et al, 5 suggests that the prevalence of significant extracranial arterial disease in India is probably lower than intracranial arterial disease. There is lack of data in northeast India regarding the prevalence of arterial disease in ischemic stroke patients.
It is important to note that there is a socioeconomic burden of ischemic stroke and a lack of data regarding the prevalence of significant extracranial carotid artery stenosis in ischemic stroke patients of northeast India. Therefore, this prospective hospital-based study was conducted in a tertiary care hospital of northeast India to assess the prevalence of extracranial carotid arterial disease in first ischemic stroke patients of this region, to study the relation of risk factors with first ischemic stroke and to compare and discuss the findings of other workers on the same subject.
Materials and Methods
This is a prospective hospital-based study done in a tertiary care hospital of northeast India. The study was conducted over a period of 2 years and 157 patients with first time ischemic strokes were recruited for this study.
For this study, 157 patients presenting with their first ever sudden onset focal neurological deficit lasting for more than 24 hours due to acute ischemic brain infarction, were selected. These patients were selected based on (1) a positive history and (2) computed tomography (CT) evidence of recent brain infarction. By history and clinical examination, all patients without acute onset focal neurological deficit lasting for more than 24 hours were excluded, for example, transient ischemic attacks. By imaging, all the other causes of acute focal neurological deficit, like intracerebral hematoma, subarachnoid hemorrhage, brain tumors, and demyelinating diseases were excluded.
All patients underwent CT of the brain, color Doppler, carotid sonogram, routine blood sugar examination and serum lipid profile examination. Blood pressures of patients were also recorded. Patients who had a brain CT done elsewhere, not in the study institution, were also accepted. In all, 44 patients had CT angiography (CTA) of the neck and brain. CT angiographies were done to correlate the findings of carotid Doppler examination.
The clinical history and findings of clinical examination were recorded in each patient to determine the duration and presence of focal neurological deficit. The patient was then taken to the CT suite and consent was taken. A CT of the brain was done, to look for any pathology, on a multidetector CT scanner (16 slice Brilliance MDCT, Philips Medical Systems, Netherlands) in a caudocranial direction from base of skull to vertex. Contrast was used, where necessary, to rule out other suspected pathologies.
After exclusion by imaging of other causes of acute onset focal neurological deficit, such as intracerebral or subarachnoid hemorrhage, brain tumors, and demyelinating diseases, the patients underwent carotid doppler sonography.
Carotid Doppler was done on a Toshiba Nemio ultrasound unit, model SSA-550A (Shimoshigami, Otowara-Shi, Tochigi-Ken, Japan). The procedure was explained to the patient before starting the procedure. A 6 to 11 MHz linear-array variable frequency transducer was used at 9 MHz for B-mode. Doppler was completed with pulsed, directional Doppler, with an angle of insonation of 60 degrees. Patients were positioned supine with arms lying beside their body, a pillow under their shoulders, with optimal neck extension, and with their face turned opposite to the side being scanned. The position of the sonographer was at the side of the patient. Each sonogram included both longitudinal and transverse images of the vessels.
B-mode sonograms were used to search for plaques, within the arterial wall. Measurements of each plaque at its point of maximum stenosis, and the vessel diameter at that point, were taken in the transverse axis and later used to calculate the percentage stenosis caused by that plaque. Fatty plaques were better appreciated on power Doppler images and power Doppler was extensively used for correlation.
The common carotid arteries (CCA), carotid bulbs, and internal carotid arteries (ICA) were examined using color Doppler, and Doppler waveforms were generated from the longitudinal plane. The Doppler waveforms were obtained with an angle of insonation at 60 degrees.
Presence and type of plaque, diameter stenosis, intima-media thickening, peak systolic velocity (PSV), and end diastolic velocities were specifically recorded. The external carotid and vertebral arteries were also assessed.
Criterion for intima/media thickening was taken as ≥0.9mm. Significant stenosis was defined as ≥50% stenosis; criteria were a diameter stenosis of ≥50%, PSV≥140 cm/sec and an ICA/CCA PSV ratio of ≥2.6–8 Severe stenosis was defined as ≥70% stenosis; criteria were a diameter stenosis of ≥70%, PSV≥230 cm/s, and ICA/CCA PSV ratio of ≥3.6–8 The arteries were sampled through the region of stenosis completely to ensure that the site of highest velocity had been located. The diameter stenosis was measured using the European Carotid Surgery Trial (ECST) criteria as it was easier to measure and more reproducible than the North American Symptomatic Carotid Endarterectomy Trial (NASCET) method. However, the measurements were subsequently converted to NASCET using the formula-

to make it comparable to the velocity measurements and CTA findings for which the NASCET method was used.9–11
Plaques were categorized into the following 5 types: Type I—echolucent; Type II—predominantly echolucent; Type III—predominantly echogenic; Type IV—echogenic; and completely calcific plaques.
In 44 patients, CTA of the neck and brain were also done; in a caudocranial direction (slice thickness 0.8 mm with 0.4 mm overlap, pitch 0.35, collimation 16 mm X 0.75 mm, 120 kV, 30 mAs). Non-ionic contrast of 100 ml was injected through intravenous route at 4.5 mL/s with pressure injector and bolus tracking. Axial source images and reconstructed multiplanar slab MIP and VR images were evaluated in a workstation. The NASCET method was used to calculate the percentage of diameter stenosis.
Risk factors of stroke were also evaluated. These were age, hypertension, hyperlipidemia, smoking, alcohol intake, diabetes, and cardiac disease. 3 A record of blood tests of these patients (for blood sugar and serum lipid profile) were maintained.
Statistical method employed were Chi-square tests to compare data and obtain statistically significant differences. A P-value of less than .05 was considered statistically significant. This study received the clearance of the Ethics Committee. All procedures were properly explained to the patients before execution and written consent were taken for the same.
Results
The carotid arteries of 157 patients were assessed with carotid sonography, out of which 14 had significant (≥50%) luminal stenosis. Of these 14 patients, 3 had complete occlusion, 2 had 70%–99% stenosis, and 9 had 50%–69% stenosis (see Figure 1, Table 1).
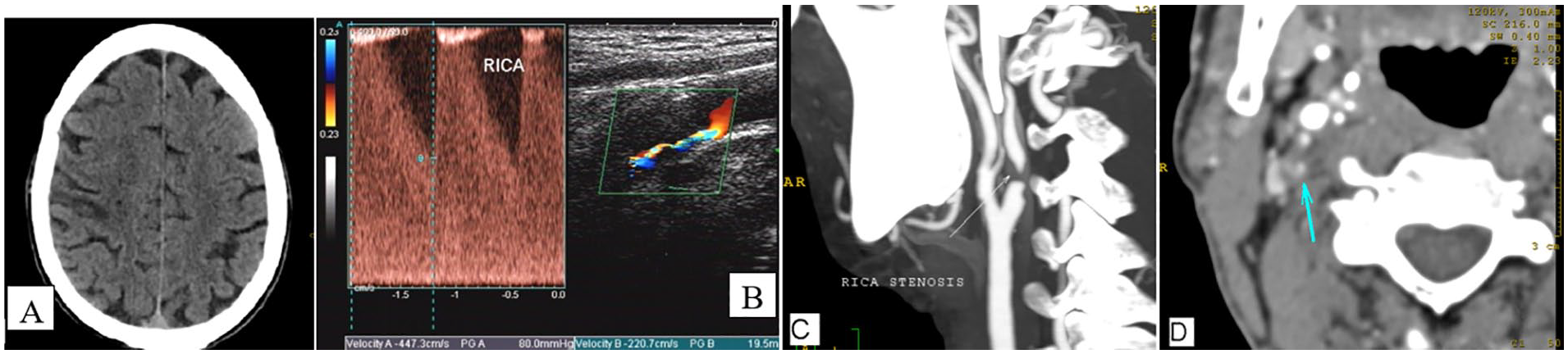
62 year old male, chronic smoker and hypertensive presenting with stroke and left sided hemiparesis one month after the ictus. Blood parameters, echocardiography and ECG were normal. CT scan (A) revealed a territorial infarct in the right fronto-parietal region. Carotid B-mode and colour doppler sonography (B) revealed a plaque causing>80% stenosis of the RICA with a peak systolic velocity in excess of 447cm/s. Smaller plaques were seen in the LCCA, LCB and LICA causing no significant stenosis. CT angiography slab MIP images (C) showed the stenosis on the right to be severe. There is some overestimation of stenosis in the MIP image seen here but the patent lumen (arrow) was seen on the axial source images (D).
Results of Extracranial Carotid Artery Sonography in First Ischemic Stroke Patients of northeast India.
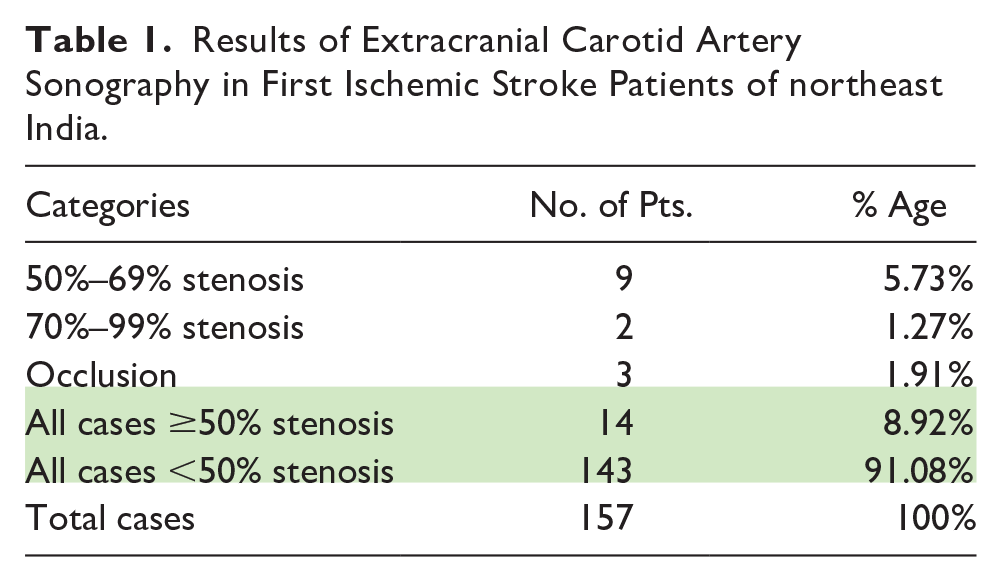
Table 1 demonstrates that only 8.92% of the patients had significant (≥50%) stenosis in either of their extracranial carotid arteries. Prevalence of significant extracranial carotid artery stenosis, therefore, is low in northeast Indian, first ischemic stroke patients.
Plaques that caused significant stenosis (≥50%) were mostly of Type II, that is, they were mixed plaques containing predominantly lipid material (see Figure 2). It was noted that power Doppler was very useful in detecting hypoechoic plaques that were hard to detect on gray scale images. Intima-media thickening was noted in 42.9% of patients with ≥50% stenosis or occlusion (see Figure 2).
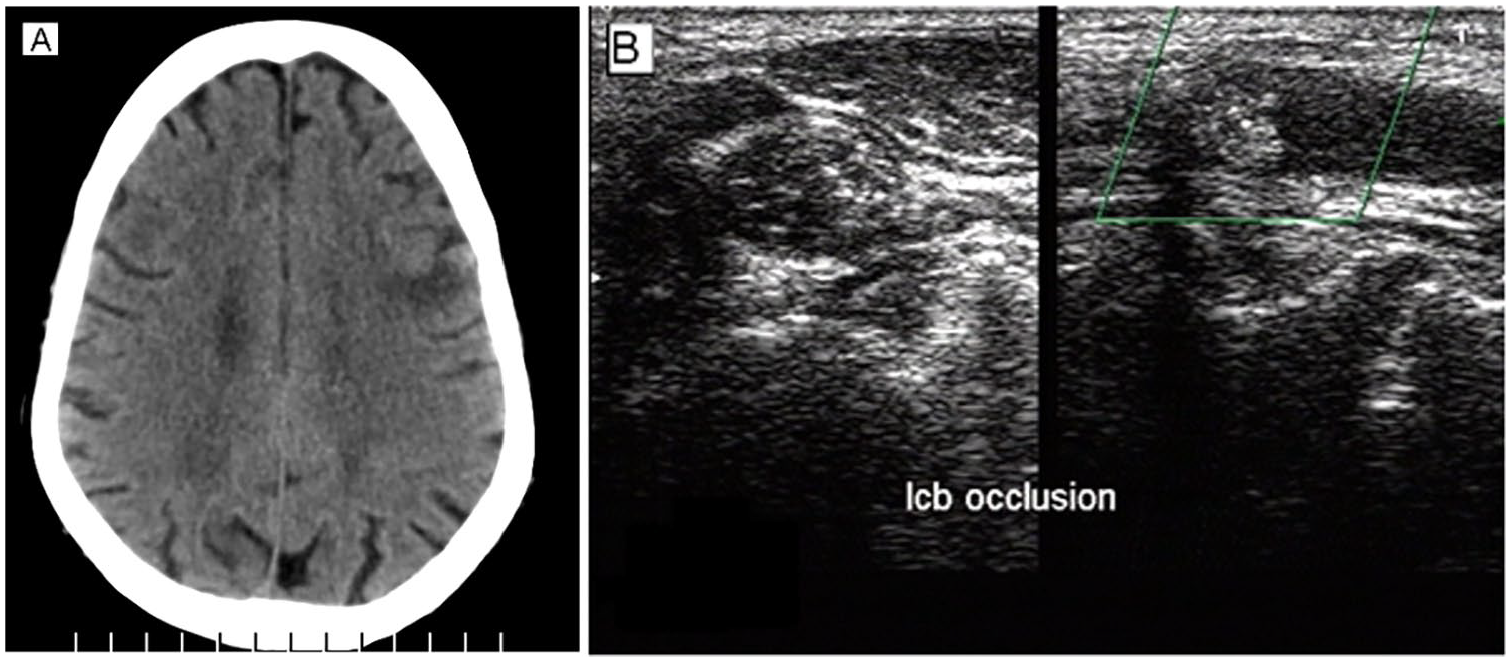
72 year old male presenting with sudden onset right sided hemiparesis and inability to speak. He was hypertensive and his blood parameters suggested hyperlipidemia. CT scan revealed subacute infarcts in the left fronto-parietal and insular regions (A). Carotid B-mode and colour doppler sonography showed no flow in the LCB and LICA indicating occlusion (B) and forward and reverse preocclusive dampened flow.
In all, 78.6% (11 patients) had significant (≥50%) stenosis on the left side, whereas 21.4% (3 patients) had significant stenosis on the right side. The mean age of patients with significant extracranial carotid stenosis (≥50%) was significantly higher than patients with <50% stenosis (yellow blocks in Table 2). Among patients with significant carotid stenosis (≥50%), males were found to have a significantly higher age than females (green blocks in Table 2). The number of males (12) with significant stenosis (≥50%) were significantly higher than females (2) (P < .05).
Results of Average Ages in Different Categories.
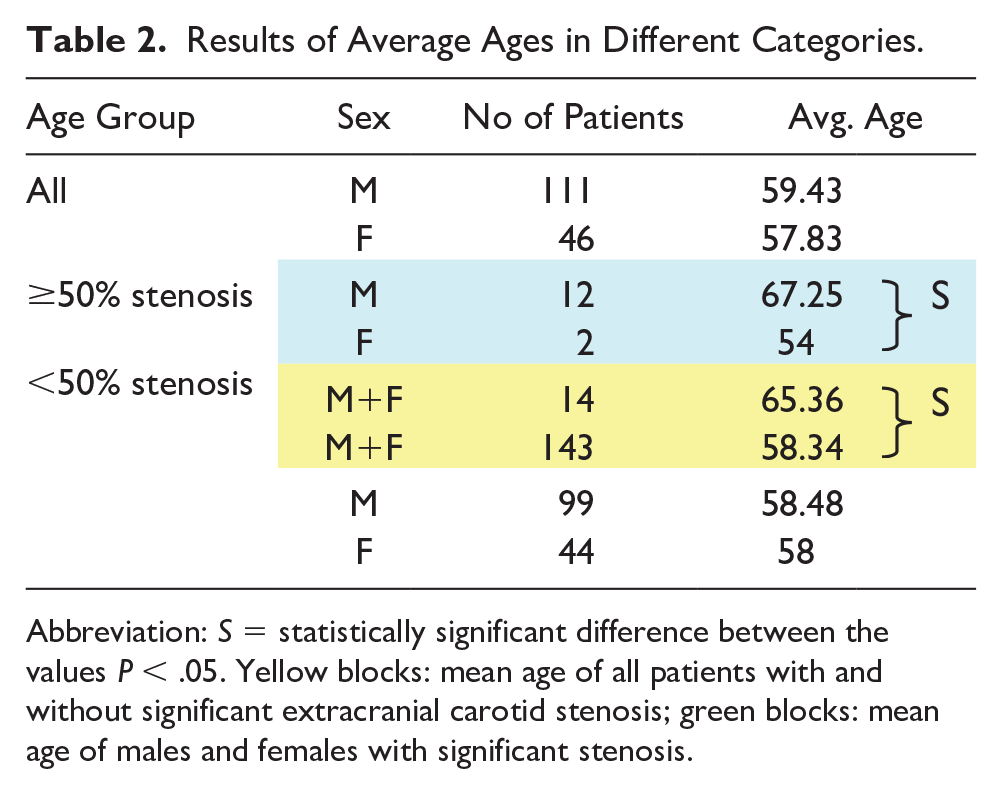
Abbreviation: S = statistically significant difference between the values P < .05. Yellow blocks: mean age of all patients with and without significant extracranial carotid stenosis; green blocks: mean age of males and females with significant stenosis.
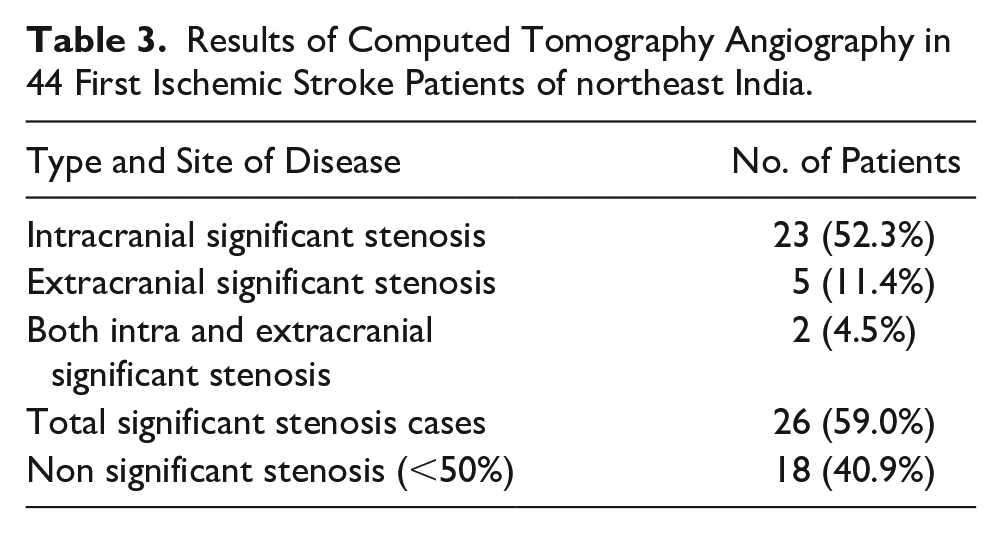
CTA correlation was done in 44 first ischemic stroke patients. From the data in these 44 patients, it was seen that the prevalence of significant intracranial arterial disease was greater than extracranial arterial disease in these northeast Indian patients (Table 3).
Results of Computed Tomography Angiography in 44 First Ischemic Stroke Patients of northeast India.
High prevalence of hypertension, dyslipidemia and diabetes were noted in the northeast Indian first ischemic stroke population. However, none of the risk factors of ischemic stroke that were assessed were significantly higher in the 50%–100% stenotic group than in the <50% stenosis group (Figure 3).
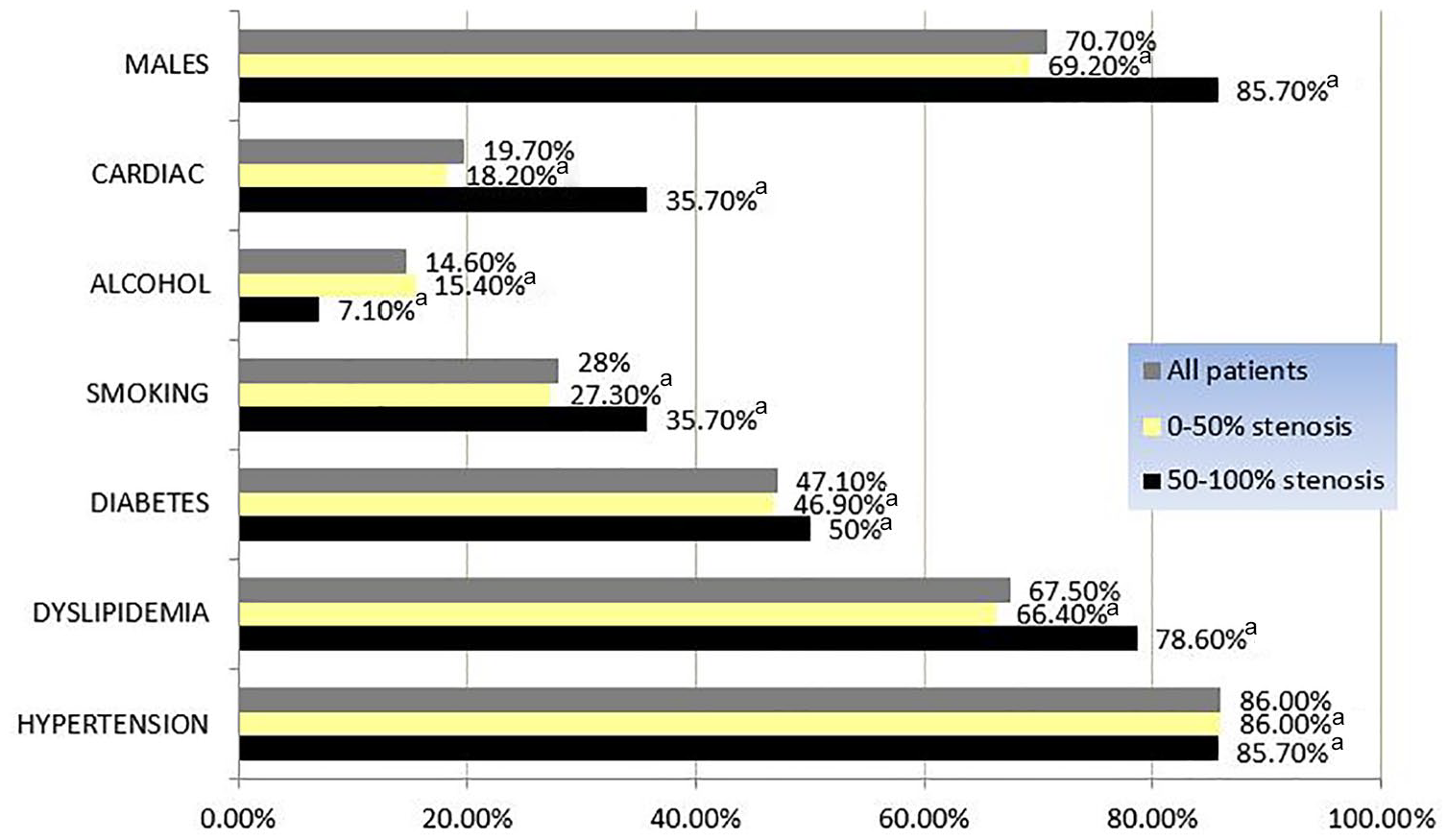
Results of risk factors in first ischemic stroke patients of northeast India.
Discussion
A large number of autopsy studies, angiography studies, doppler studies, and clinical trials now exist that have shown racial differences in distribution of occlusive disease in the arteries supplying the brain.12–19 These racial differences (in disease distribution of the intracranial and extracranial arteries) have been reported among ischemic stroke patients in studies from across the world.15,20–26 Most of these studies have shown a higher prevalence of extracranial arterial stenosis and a lower prevalence of intracranial arterial stenosis in Caucasians, but this was not the case in Africans and Asians, with numerous studies showing a reverse distribution pattern. Carotid endarterectomy and stenting are now accepted modalities for reducing the threat of recurrence of ischemic strokes in patients with severe carotid artery stenosis.
There is scarce data on Indian patients. A MR angiography (MRA) based study by Padma et al, 5 had been done in patients with recent onset of ischemic stroke. In this study of 100 patients, there was a smaller number of patients (26%) with ≥70% stenosis of extracranial carotid arteries while more (45%) had ≥70% stenosis of intracranial arteries. The study had its limitations in that the number of patients enrolled was less and MRA is known to overestimate stenosis, which may have shown a higher number of lesions with severe stenosis. However, the pattern of more intracranial to extracranial arterial stenosis as reported in other studies on Asians was reflected in this study. 5 The present study has demonstrated that the prevalence of extracranial carotid stenosis in northeast Indian first ischemic stroke patients is low. Further CTA correlation has shown that not only is the prevalence of extracranial stenosis low, but also the intracranial arterial stenosis in the same group of patients is high (Table 3). When only extracranial carotid arteries were scanned (with sonography), few (8.92%) cases with ≥50% stenosis were found, whereas assessment of both neck and brain arteries (with CTA) revealed a sizable number (59.0%) of cases with ≥50% stenosis (of which 52.3% had intracranial arterial stenosis).
The results of the present study are similar to a study on Taiwanese population by Tan et. al, conducted on 276 patients with first ischemic stroke by carotid doppler ultrasonography (Figures 4 & 5). They found the prevalence of significant (≥50%) extracranial carotid stenosis to be 8% with color Doppler carotid sonography. In all, 64 of their 276 patients also had CTA evaluation of the neck and intracranial vessels. They found a prevalence of 69% significant (≥50%) intracranial artery stenosis in the subset of patients assessed by CTA. Our findings are similar to the findings of this Taiwanese study, that is, we found a prevalence of 8.92% significant (≥50%) extracranial artery stenosis with ultrasonography and 52.3% significant (≥50%) intracranial arterial stenosis in 44 patients assessed with CTA (Figures 4 & 5). 6
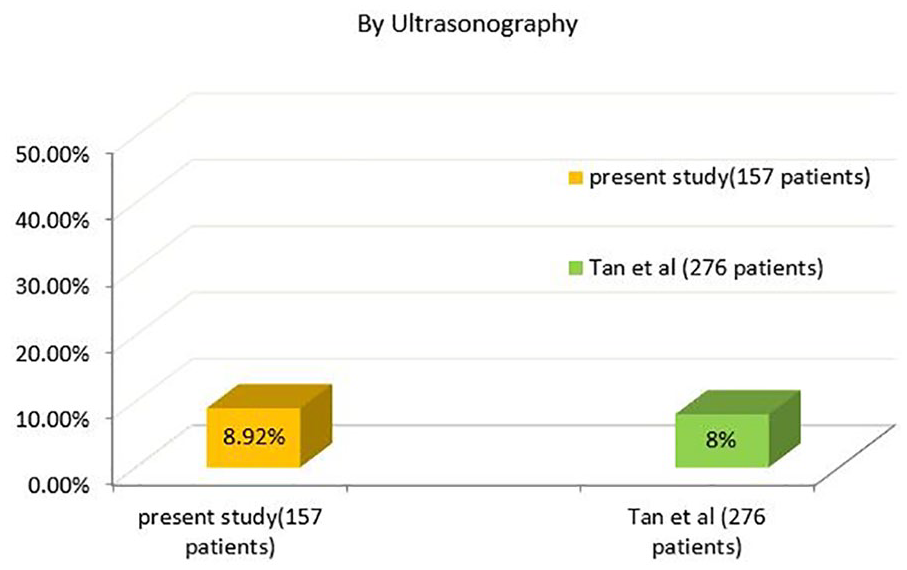
Comparison of significant (≥50%) extracranial carotid artery stenosis by sonography in first ischemic stroke patients (157 patients in present study, 276 patients in study by Tan et al 6 ).
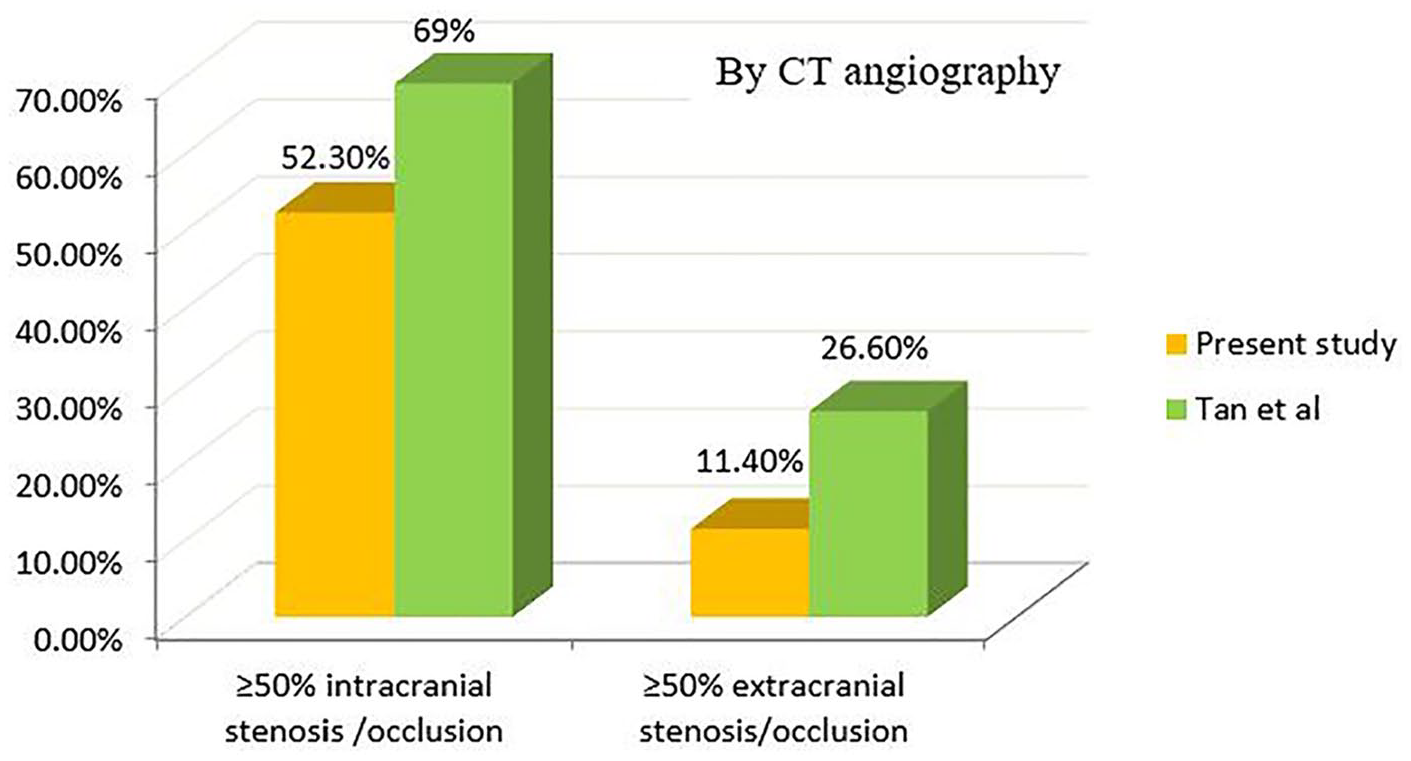
Comparison of significant (≥50%) stenosis by CT angiography in first ischemic stroke patients (44 patients in present study, 64 patients in study by Tan et al 6 ). CT, computed tomography.
Comparison of ischemic stroke patients with significant (≥50%) extracranial carotid artery stenosis of different ethnic origins is demonstrated in Table 4.6,27–31 The northeast Indians have a similar low prevalence of significant extracranial carotid stenosis as other Asians, but compared to other Asians, the prevalence in northeast Indians is even lower. Statistical analysis of the data showed that Caucasians have a significantly higher prevalence of ≥50% extracranial carotid stenosis than northeast Indians. It also revealed a significantly higher prevalence of extracranial carotid stenosis compared to the northeast Indians in the Japanese population from one study (Kieffer et al 29 ). Contrarily, another study (Brust 31 ) in the Japanese population showed no significant difference from the northeast Indians. It was observed, however, that the prevalence of extracranial significant stenosis was greatest among the Asians in the Japanese ischemic stroke population. 31
Comparison of Significant (≥50%) Extracranial Carotid Artery Stenosis in Ischemic Stroke Patients of Different Ethnic Origins.
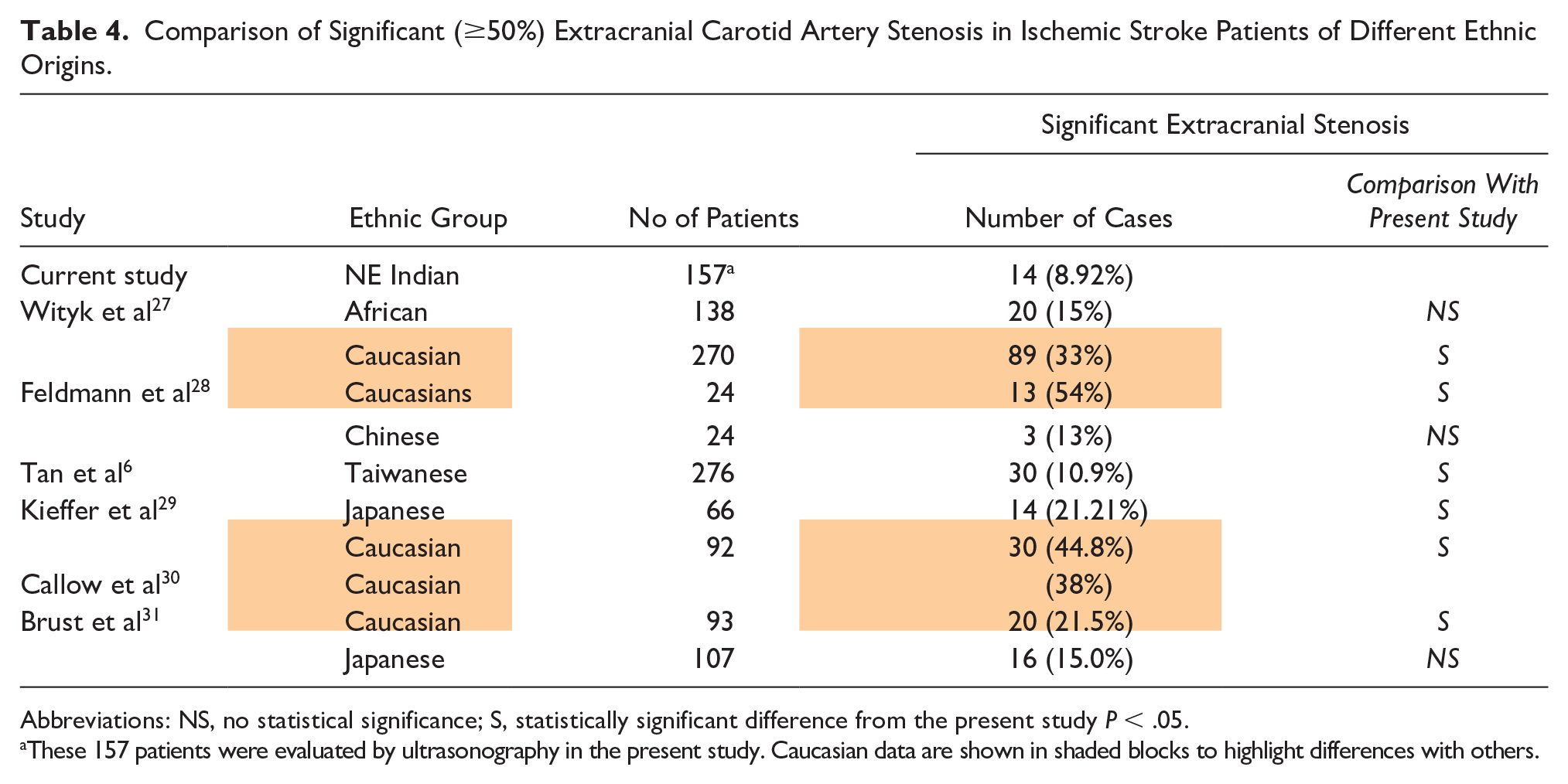
Abbreviations: NS, no statistical significance; S, statistically significant difference from the present study P < .05.
These 157 patients were evaluated by ultrasonography in the present study. Caucasian data are shown in shaded blocks to highlight differences with others.
In Table 5, CTA data of ≥50% intracranial and extracranial carotid artery stenosis was compared with ischemic stroke patients of different ethnic origins, and it was found that a statistically significant difference exists in the prevalence of intracranial arterial stenosis of Caucasians from the northeast Indians.6,27–31 As is evident from the table, northeast Indians have a high intracranial arterial stenosis and a low extracranial arterial stenosis, while Caucasians have low intracranial arterial stenosis and high extracranial arterial stenosis. A statistically significant difference in intracranial arterial stenosis of the northeast Indians from the Africans and Japanese was also found, but there was no difference in the results of the present study from the studies on Chinese and Taiwanese populations (Table 5).
Comparison of ≥50% Intracranial and Extracranial Arterial Stenosis in Ischemic Stroke Patients of Different Ethnic Origins With CT Angiography Results of the Present Study.
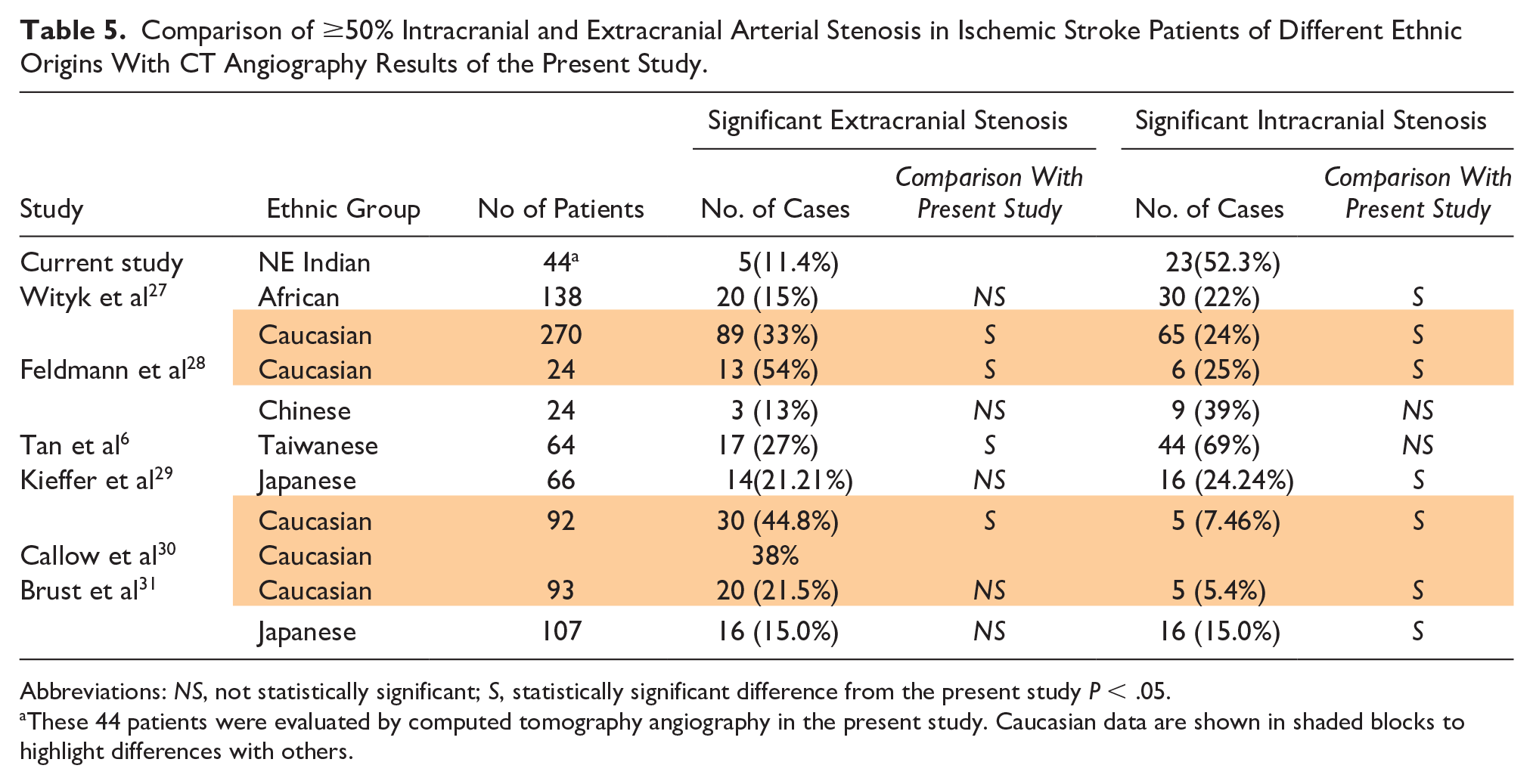
Abbreviations: NS, not statistically significant; S, statistically significant difference from the present study P < .05.
These 44 patients were evaluated by computed tomography angiography in the present study. Caucasian data are shown in shaded blocks to highlight differences with others.
The same pattern is noted on comparing ≥70% stenosis in different ischemic stroke populations in Table 6.12,32,33 It is determined from Table 6 that northeast Indians, Koreans and Chinese ischemic stroke patients have very low prevalence of severe(≥70%) extracranial carotid artery stenosis compared to the Caucasians. The Africans have a higher prevalence of severe extracranial stenosis than the Asians, but it is much lower than the Caucasians. Statistical analysis reveals that the prevalence of severe extracranial carotid stenosis in northeast Indians is significantly lower than most other ischemic stroke populations (except the Chinese) (Table 6).
Comparison of Severe (≥70%) Extracranial Carotid Artery Stenosis in Ischemic Stroke Patients of Different Ethnic Origins.
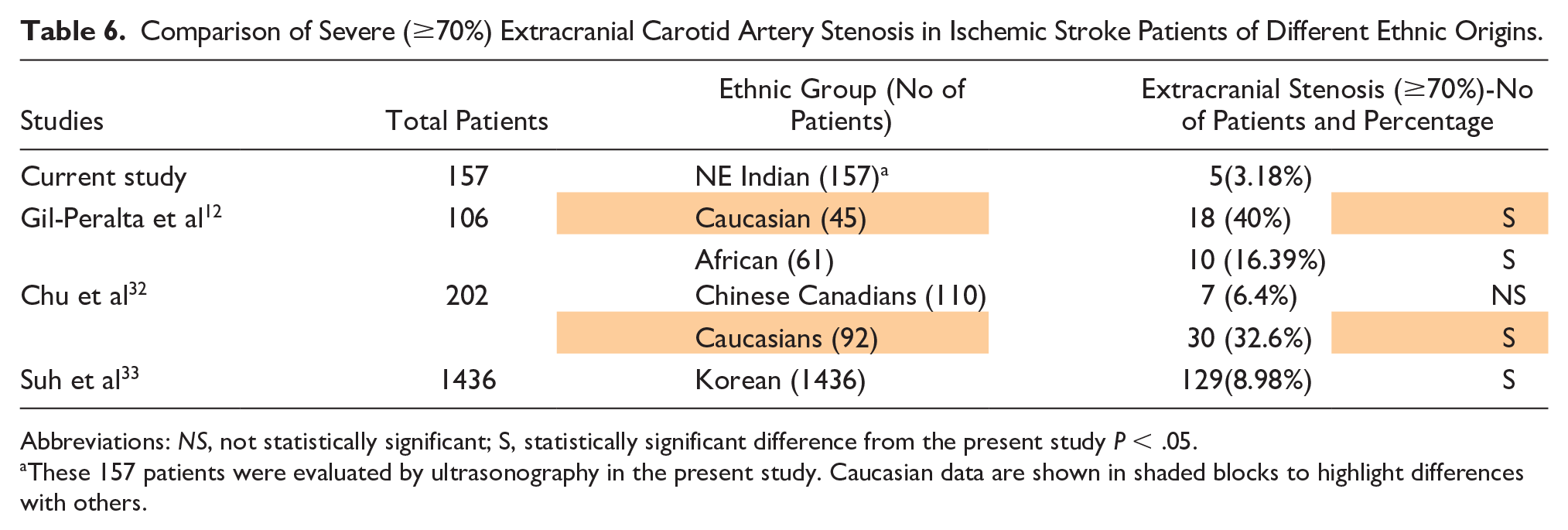
Abbreviations: NS, not statistically significant; S, statistically significant difference from the present study P < .05.
These 157 patients were evaluated by ultrasonography in the present study. Caucasian data are shown in shaded blocks to highlight differences with others.
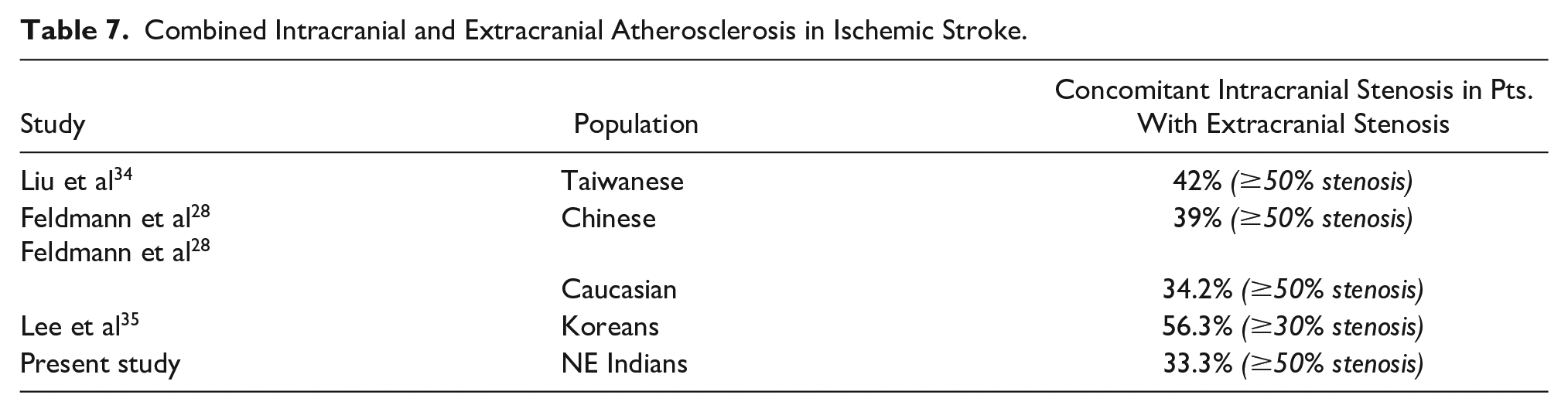
Concomitant intracranial arterial stenosis in patients with extracranial stenosis is seen in 34.2% of Caucasians and 39%–56.3% of Asians (Chinese, Taiwanese and Koreans). Comparatively the prevalence in northeast Indians is less as seen in Table 7.28,34,35
Combined Intracranial and Extracranial Atherosclerosis in Ischemic Stroke.
From Table 8, it is noted that the proportion of males experiencing ischemic stroke for the first time is significantly higher in the northeast Indians than in Caucasian, African, Hispanic and Taiwanese populations.6,27,36,37 A significantly higher number of ischemic stroke patients of northeast India have hypertension, hyperlipidemia and diabetes mellitus as compared to Caucasian, African, Hispanic and Taiwanese populations. Africans and Hispanic ischemic stroke patients have a higher prevalence of hypertension than Caucasians, whereas the prevalence of hypertension in the Taiwanese population is as low as the Caucasians.6,27,36,37
Comparison of Prevalence of Risk Factors in Ischemic Stroke Patients of Different Ethnic Groups.
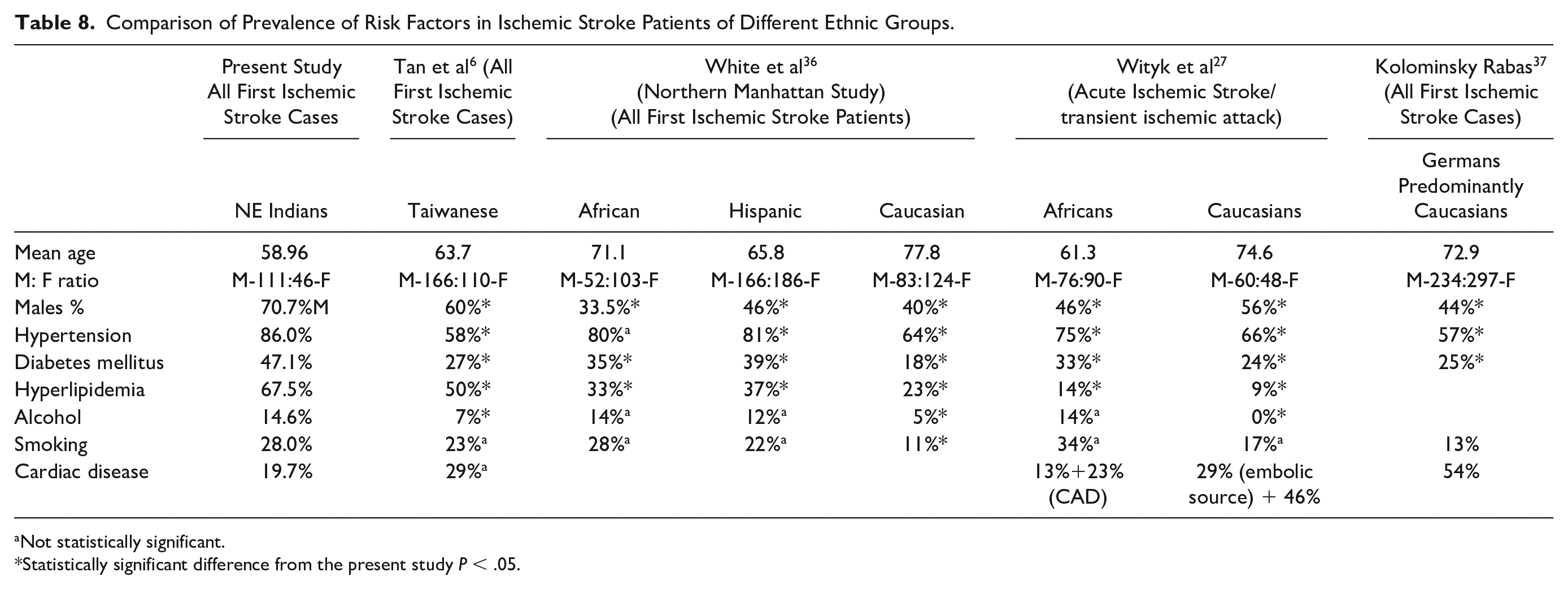
Not statistically significant.
Statistically significant difference from the present study P < .05.
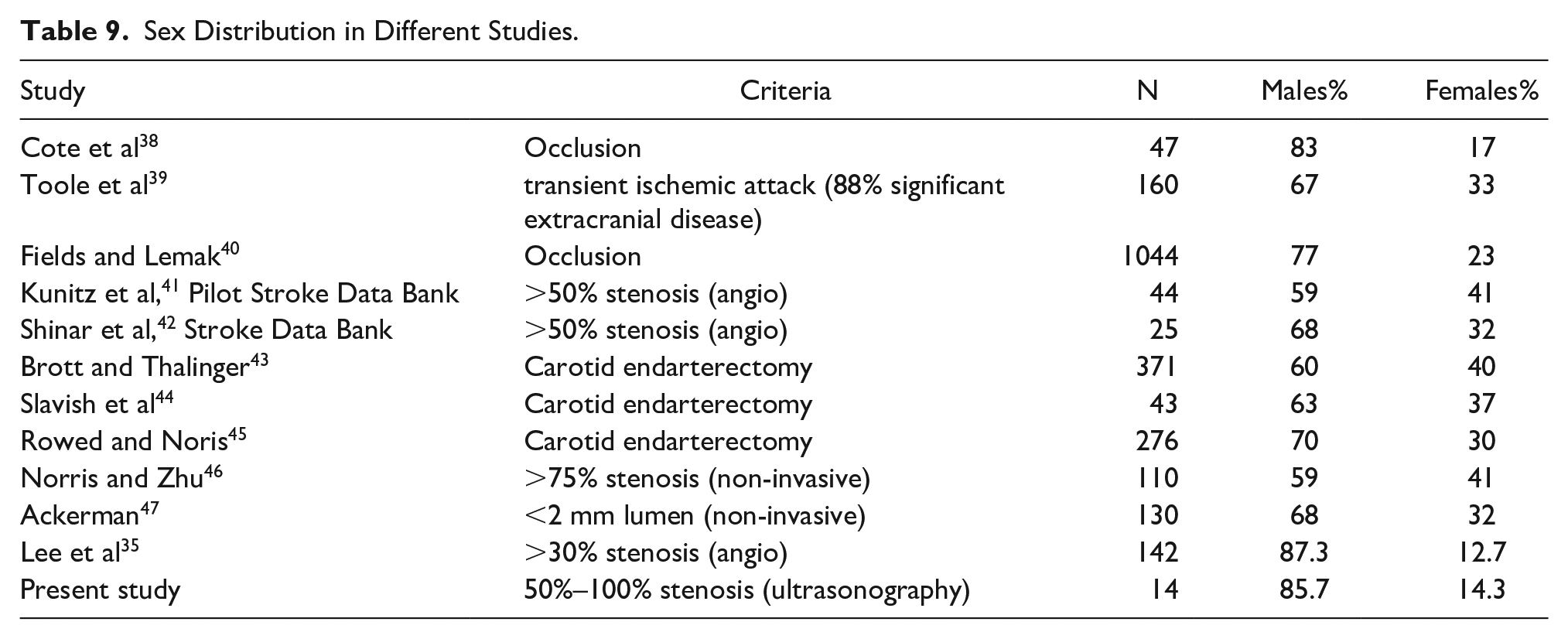
Several studies have reported a male preponderance in extracranial carotid artery disease (See Table 9). The proportion of male patients with significant stenosis in the present study is very high, but the number of patients having significant stenosis in the present study is less. A larger study needs to be done before any definite conclusion can be made (See Table 9).
Sex Distribution in Different Studies.
Conclusion
The prevalence of significant extracranial carotid artery stenosis in northeast Indian patients with first ischemic stroke is low, and it is significantly lower compared to Caucasians. The low prevalence of significant (≥50%) extracranial carotid artery stenosis in northeast Indians is similar to that in other Asians. However, compared to rest of the Asians, the prevalence in northeast Indians is even lower.
Northeast Indians, like other Asian ischemic stroke patients, have low prevalence of severe (≥70%) extracranial carotid artery stenosis, compared to the Caucasians. Africans have a higher prevalence of severe extracranial stenosis than the Asians, but it is lower than the Caucasians.
Significant (≥50%) intracranial arterial stenosis may be more common in our patients with first ischemic stroke as evident from the limited CTA data. A larger study is required to confirm these findings. The prevalence in patients with first ischemic stroke of significant (≥50%) stenosis in the intracranial arteries is significantly higher in northeast Indians as compared to Caucasians. The pattern of low extracranial significant (≥50%) arterial stenosis and high intracranial significant (≥50%) arterial stenosis seen in northeast Indians is similar to that reported in the Africans and other Asians. On the contrary, Caucasians have high significant (≥50%) extracranial artery stenosis and low significant (≥50%) intracranial arterial stenosis. Since ischemic stroke is a disease with a variety of pathophysiologic mechanisms, assessing only the extracranial carotid arteries cannot provide sufficient information regarding the cause of ischemic stroke in northeast Indian patients.
With a higher prevalence of intracranial stenosis in our population, there is a need to focus on this aspect in these ischemic stroke patients. Intracranial angiography (with conventional, MR or CT angiography) will allow a more comprehensive assessment of ischemic stroke patients. Advances in the diagnosis and management of intracranial arterial stenosis are the need of the hour and may be hugely beneficial to such patients in northeast India and rest of the world. Larger studies, especially on intracranial arteries, are required on ischemic stroke patients of rest of the Indian subcontinent and on other large ethnic groups hitherto unexplored.
Increased age and male sex are important factors associated with first ischemic stroke in northeast Indian patients. Northeast Indian males present with first ischemic stroke at an older age than females. The proportion of males experiencing ischemic stroke for the first time is significantly higher in the northeast Indians than in Caucasian, African, Hispanic and Taiwanese populations. Northeast Indian patients experience first ischemic stroke at a lower age than their Taiwanese, African, Hispanic and Caucasian counterparts.
High prevalence of hypertension, dyslipidemia and diabetes were noted in the northeast Indian first ischemic stroke population. The presence of these risk factors in northeast Indians is significantly higher than Caucasian, African, Hispanic and Taiwanese populations. Management of these modifiable risk factors in northeast Indian population may effectively reduce the risk of ischemic stroke.
The combination of gray scale sonography, color, and power Doppler, as well as spectral tracings could be used to accurately assess the severity of significant extracranial carotid artery stenosis. Not only can the stenosis be assessed, but also the arterial wall can directly be visualized, and plaques can be characterized. It is difficult to accurately assess plaques and evaluate the severity of stenosis caused by them with single criteria (PSV, EDV, IC/CC ratio, or diameter stenosis) by ultrasonography and more than one criterion are necessary.
There are certain limitations of sonography that need to be underscored when performing the procedure. CTA is possibly better for assessing some calcific plaques than sonography, as it was found out in 2 cases in this study where sonography failed to assess calcific plaques causing ≥50% stenosis.
Limitations
Carotid sonography has certain limitations. In case of a calcified plaque in the anterior arterial wall, the lumen beyond may not be accessible by sonography. Additionally, velocities may not always be elevated immediately proximal or distal to the stenotic area, as in two cases of significant stenosis that were correlated with CTA. Also, though with increasing stenosis PSV rises, at very severe stenosis the velocities may fall. This may lead to misinterpretation of the results. Access to the carotid bifurcation and ICA is not always possible. There can be a high bifurcation, stiff neck, uncooperative and restless patient or other factors that may make visualization difficult or impossible in certain carotids.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.