
Abstract
Objective:
The MAGEC (Magnetic Expansion Control) rods were introduced to a medical institution in 2015. The rod expansion procedures were initially evaluated with radiographs. The staff undertook a quality initiative to reduce radiation exposure by utilizing sonography.
Material and Methods:
The radiation dose for a typical visit was measured by examining DICOM imaging data, stored in PACS. Imaging visit time was determined from the difference between times of first radiograph/sonogram before distraction to last radiograph/sonogram after distraction.
Results:
The 21 patients (8 male, 13 female) were an average age of 11.4 ± 2.82 years (age at implant = 7.5 ± 1.94) when evaluated. The average length of time for a radiographic visit was 40.7 ± 20.7 minutes, whereas a sonography visit was 10.7 ± 3.7 minutes. Radiation dose per study visit prior to the introduction of the MAGEC clinic was 0.42 ± 0.39 mSv. Given an ideal patient schedule, the MAGEC clinic could reduce radiation dose by 1.3 to 2.5 mSv annually, with 95% confidence.
Conclusion:
This quality improvement study demonstrated a reduction in radiation exposure and imaging time. The added benefits were providing a successful multidisciplinary imaging clinic and creation of a new exam that aligned with the “ultrasound first” initiative.
The appearance of early onset scoliosis (EOS) is defined as a three-dimensional spinal deformity in which the spine is curved greater than or equal to 10° in the frontal plane before the age of five.1,2 EOS is usually divided into three groups: neuromuscular, congenital, and idiopathic.3–6 Neuromuscular and congenital forms are usually most severe, with continued progression of spinal curvature well into adulthood. Left untreated, this condition can persist and compromise the pulmonary and cardiac systems as well as induce pain and physical deformity. 7 This can result in severe deterioration to the quality of life and a significantly increased mortality. 8 Once the spinal curve reaches greater than 45°, surgical intervention usually occurs. Spinal deformity in such a young age group is quite challenging given the fact that the spine, thorax, and its contents are rapidly growing. Conservative measures such as bracing and casting often fail to prevent progression of the curvature. In children with EOS, it is essential to both stabilize the curve and provide for growth of the spine. Prior to 2014, the most common operative solution was traditional growing rods (TGR).9,10 These are metal rods affixed to the axial skeleton proximally and distally with a movement segment in the middle. Adjustment requires an operation every six months until skeletal maturity. During surgery, the amount of growth can be measured directly and confirmed with radiographs. The stress of repeat surgeries coupled with the increased chance of infection, possible anesthesia complications, and psychological impact to both parent and child led to the latest technological development: magnetically controlled growing rods (MCGR).3,5,11–13 MCGR surgery is a recent development for the treatment of EOS.3,14-16 Ellipse technologies, makers of the MAGEC system (NuVasive, San Diego, California), were the first company given approval by the US Food and Drug Administration, in February 2014. 17 MCGRs utilize an external magnetic remote control device on the surface of the skin to distract the rods without the need for repetitive surgeries. This allows for more frequent distractions every four to six weeks, which more closely aligns with the normal physiologic growth curve.1,7,14
Although MCGR surgery can improve patient care, it introduced the need for additional radiographs to be performed on the child. Patients with TGR received surgical lengthening radiographs twice a year, whereas MCGR distractions could now be performed six times a year, resulting in 12 (before and after) radiographs a year. The increase in the number of radiographs caused concern for the increased ionizing radiation exposure for these children. 18 Excess amounts of ionizing radiation, even as few as 25 whole spine radiographs, have been reported to increase the risk of breast cancer by 70%.1,4,13,18–20 To reduce the ionizing radiation dose, institutions began looking at alternative ways to image the MCGRs, such as with sonography.1,21 At one particular institution, the staff initially introduced a protocol change by utilizing ultrasound to reduce a patient’s radiation exposure (this also aligned with the campaign known as “ultrasound first"). This subsequently led to the development of a MAGEC rod clinic, which was designed to reduce patient wait times.
Materials and Methods
The study clinic received institutional review board approval for this study as a quality improvement project. The surgeons began performing MAGEC rod surgeries in June 2014, four months after FDA approval. In September 2016, the staff implemented sonographic imaging to document MAGEC rod expansion. The majority of patients at the study institution had had MCGRs placed for nonidiopathic indications.
Prior to formation of the MAGEC rod sonography clinic, patients would receive their predistraction scoliosis series radiographs in a dedicated orthopedic radiography room in a busy orthopedic clinic. After the radiographs, the patients would check in and see the orthopedic surgeon and have their distraction performed in the clinic. After distraction, the patients would once again return to the clinic for postdistraction radiographs. They were then asked to report to a consultation room to discuss results. Occasionally patients would need to have radiographs taken in the main radiology department, which is on a different floor. Delays were not uncommon due to limited access to radiography rooms.
Multidisciplinary Clinic Development
Initial MCGR sonography was performed within the orthopedic clinic. The ultrasound unit, two sonographers and a radiologist, was given a clinic room. It was technically successful but inefficient with excessive downtime between patients. Limitations on ergonomics due to nonmobile tables and lack of computer access in the room were challenging. Having a radiologist and sonographers out of their department for an extended period of time was considered nonproductive.
Therefore, a meeting was set up between radiology and the orthopedic department to discuss an alternate process. Patients were scheduled in the radiology department rather than the orthopedic clinic for imaging and clinic visit to include MCGR expansion with the orthopedic surgeon. Consecutive MAGEC rod patients were scheduled every 30 minutes during a block of time using two sonography exam rooms. Current outpatient blocks consisted of one-hour slots, so this setup allowed for twice as many patients to be imaged. A room was also provided in the radiology department for the orthopedic surgeon to consult with the patients if needed. These modifications enabled the staff to provide the same service but with improved ergonomics and time savings.
The MCGR clinic team includes a radiology nurse, an orthopedic medical assistant (MA), two sonographers, a radiologist, an orthopedic surgeon, and the MAGEC representative, who brought the external remote controller. It was decided to use two adjacent exam rooms to be able to streamline the process. This allowed for a sonographer to be in each room while the physicians and representative move back and forth between patients. Additionally, if the patient required radiographs, orders could be placed and the patient sent across the hall for a radiograph.
The final process implemented for the MAGEC rod clinic was as follows (see Figure 1):
⎕ The patient checks in.
⎕ Front desk contacts nursing and the sonographers that the patient is ready.
⎕ MA retrieves patient and family from the wait area to the holding area.
⎕ Nursing performs vitals.
⎕ MA enters the information, escorts family to a sub-wait area, and notifies the sonographer that the patient is ready.
⎕ Previous imaging is reviewed by a sonographer and a radiologist.
⎕ The MA brings the patient and family into the exam room, and a sonographer performs the preimaging with a radiologist.
⎕ The orthopedic surgeon and representative then come into the exam room. The orthopedic surgeon locates the magnet and then applies the external remote controller for the distraction.
⎕ Once completed, the sonographer performs the postimaging examination.
⎕ The delta (or difference) is determined, and if needed, an additional distraction is performed.
⎕ Occasionally, the patient is in need of a semiannual radiograph.
⎕ If that is the situation, an order is entered by the orthopedic surgeon and the patient is taken for the radiograph.
⎕ Once the radiograph is performed, the MA escorts the patient and family to a consult room, if needed, for the orthopedic surgeon to review the results with the family.
⎕ The patient is then discharged.
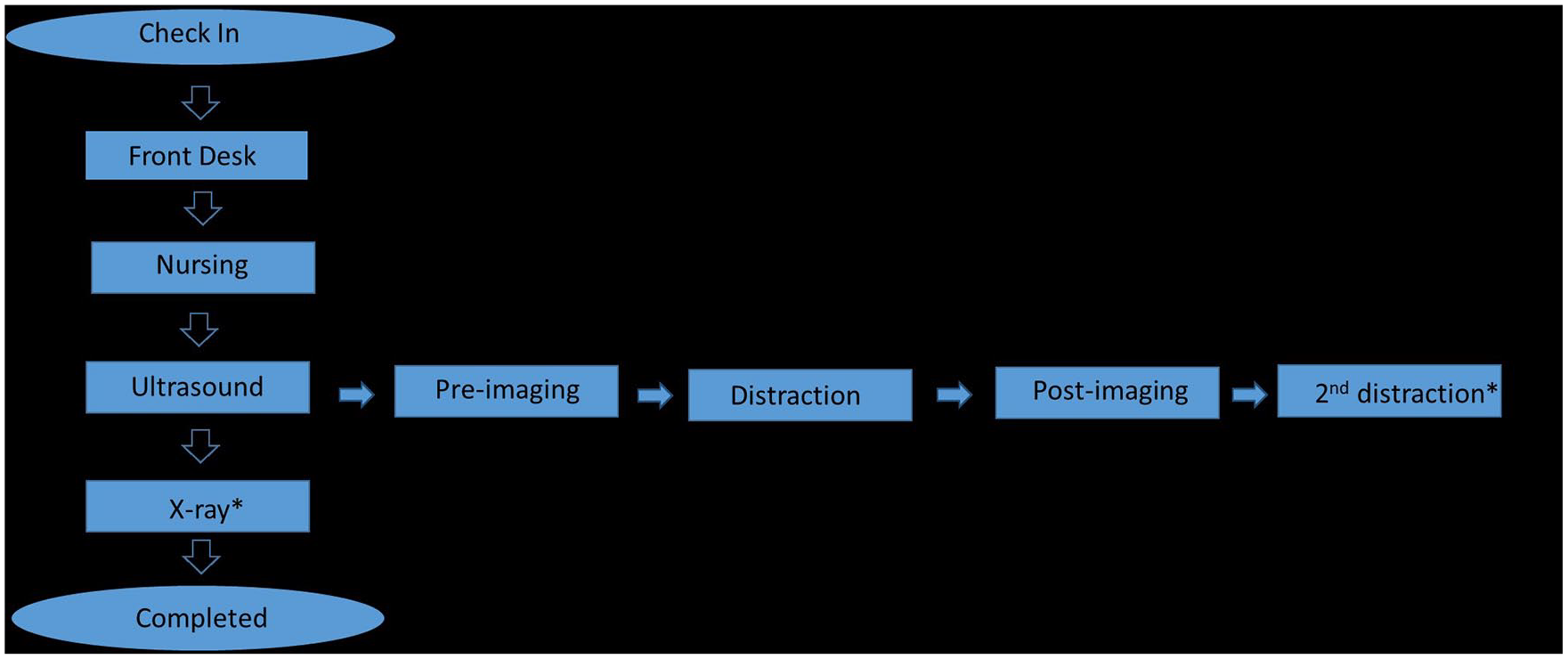
Sonography flow diagram to outline process for MAGEC clinic. * indicates “if needed.”
Sonographic Technique
A worksheet (see Figure 2) was formulated based on the published work by Stokes et al 1 , Yoon et al 2 , and Cheung et al 7 prior to the first sonographic distraction. The worksheet allowed sonographers to record pre- and postmeasurements as well as the distraction setting. We decided on two measurements each, pre- and postdistraction, as well as confirming the accuracy of the measurements. Additional space was included for a second postmeasurement if a second distraction was needed.
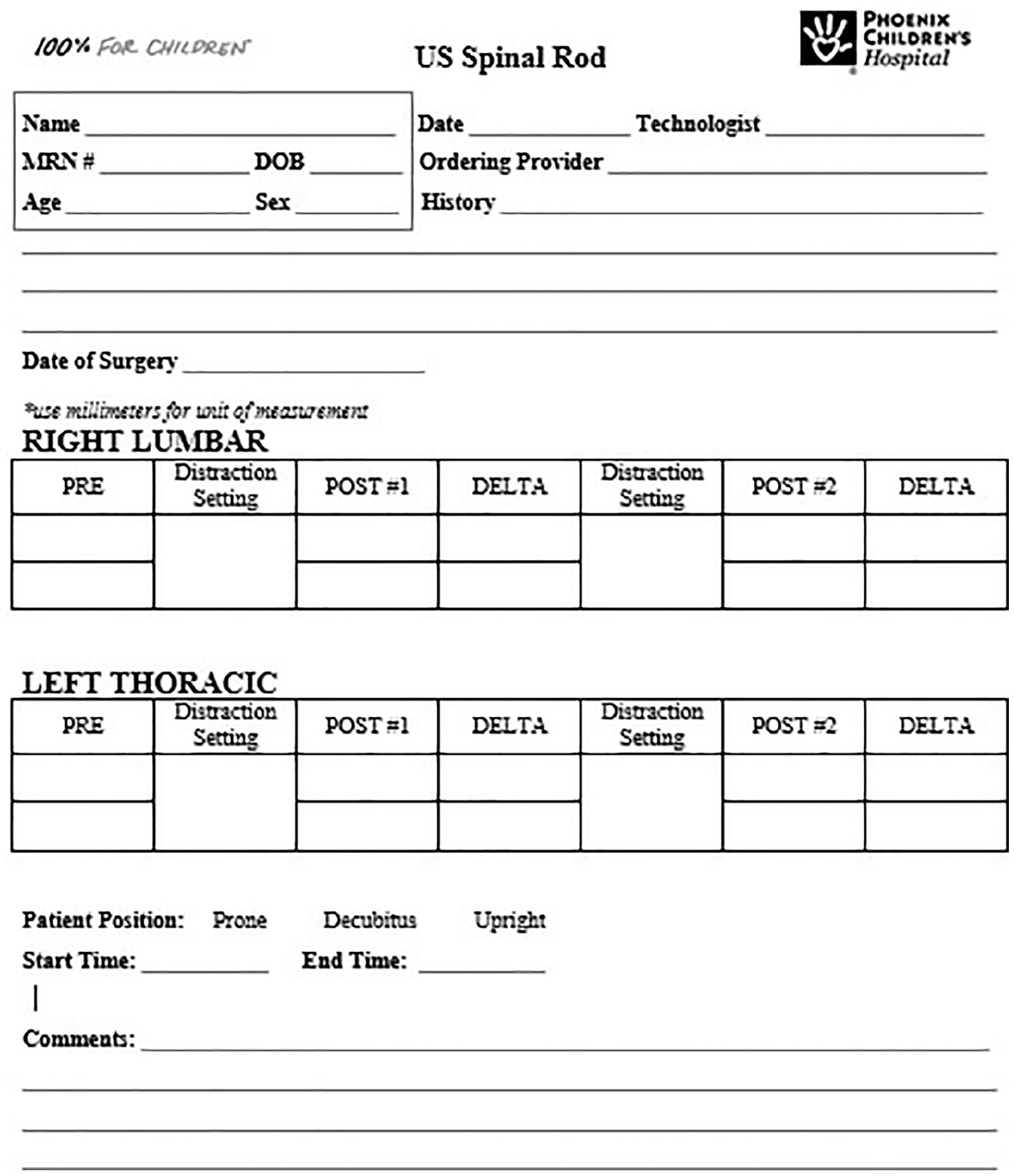
Sonography worksheet.
Patients were imaged either in the prone, left lateral decubitus position or seated on the edge of the stretcher with their back to the sonographer (see Figure 3). The sonographic patient cases were imaged with a Philips IU22 system and a linear 12-5 MHz transducer.
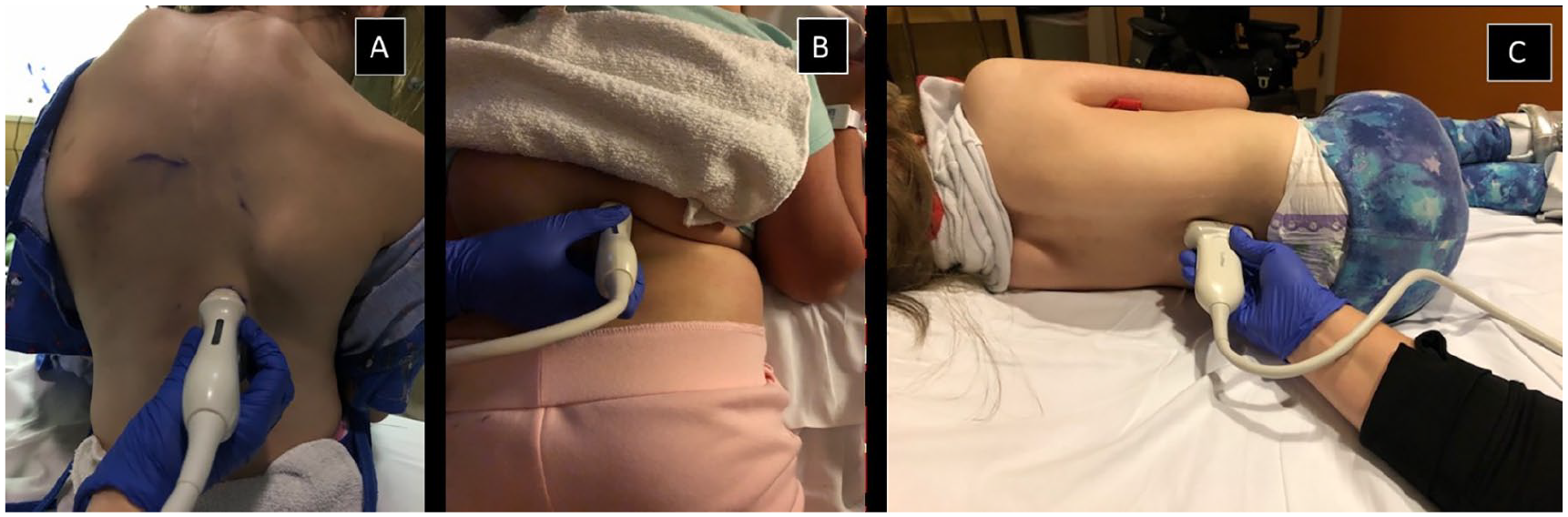
Patient position for magnetically controlled growing rods (MCGR) imaging. (A) Upright. (B) Prone. (C) Left lateral decubitus.
Prior to sonography, the most recent scoliosis radiograph was viewed to determine whether there was a single- or dual-rod system and also to determine the rod orientation and magnet position (Figure 4). Once the location of the rods had been determined, a preexpansion measurement was obtained (see Figure 5). Measurements are made from the tip of the inner rod to the point at which the rod curves.1,2,7,18 The point at which the rod curves is demarcated on the sonogram by a posterior shadow. This occurs due to the change in the angle of the rod coupled with the specular reflection of the ultrasound beam. This shadowing helps to aid in placement of the caliper for measurements and increases the confidence level for reproducibility.
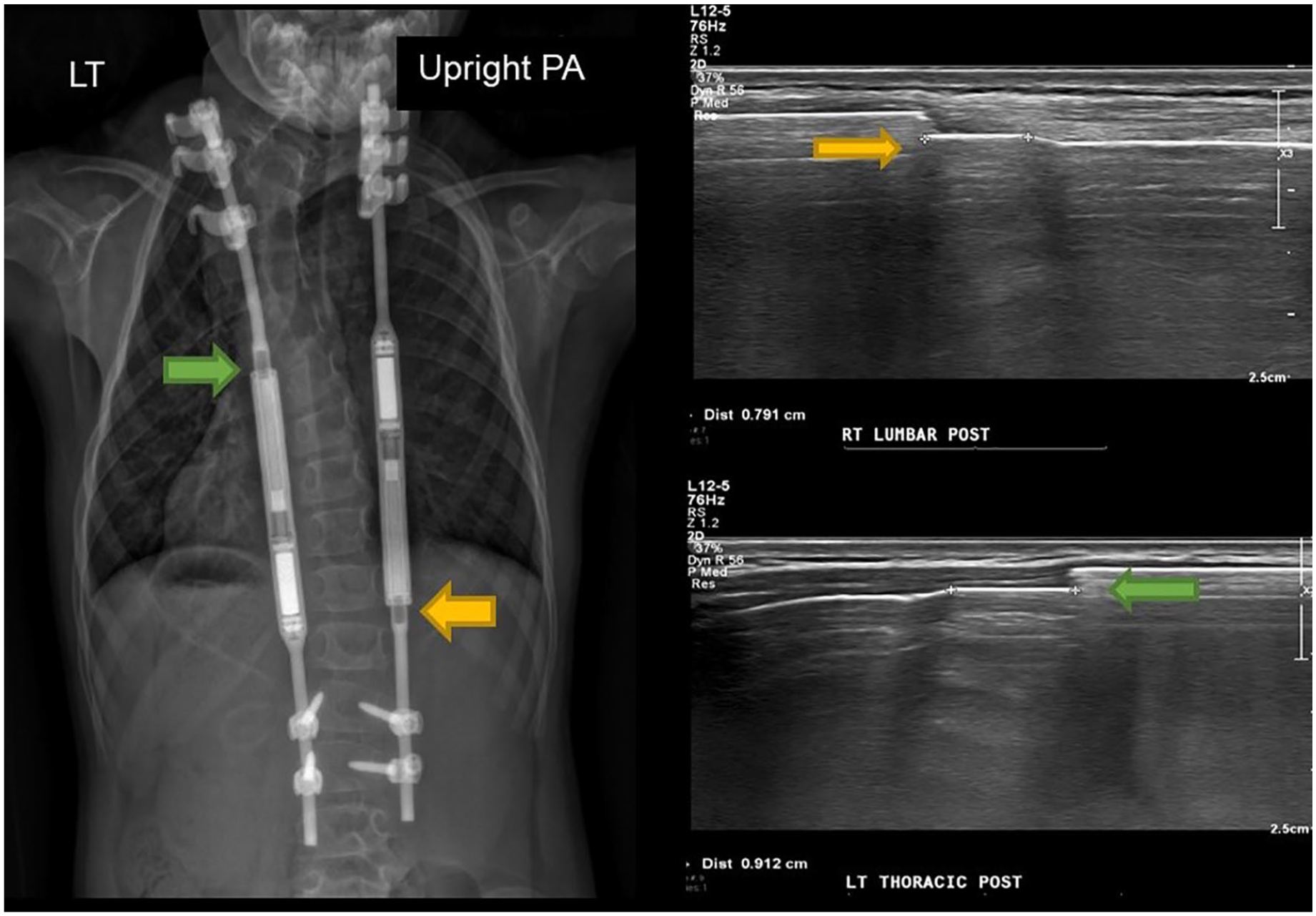
Postsurgical posteroanterior radiograph with associated sonogram that demonstrates offset magnetically controlled growing rods (MCGR) placement. The yellow arrow pushes out toward the lumbar region; the green arrow pushes out toward the thoracic region.
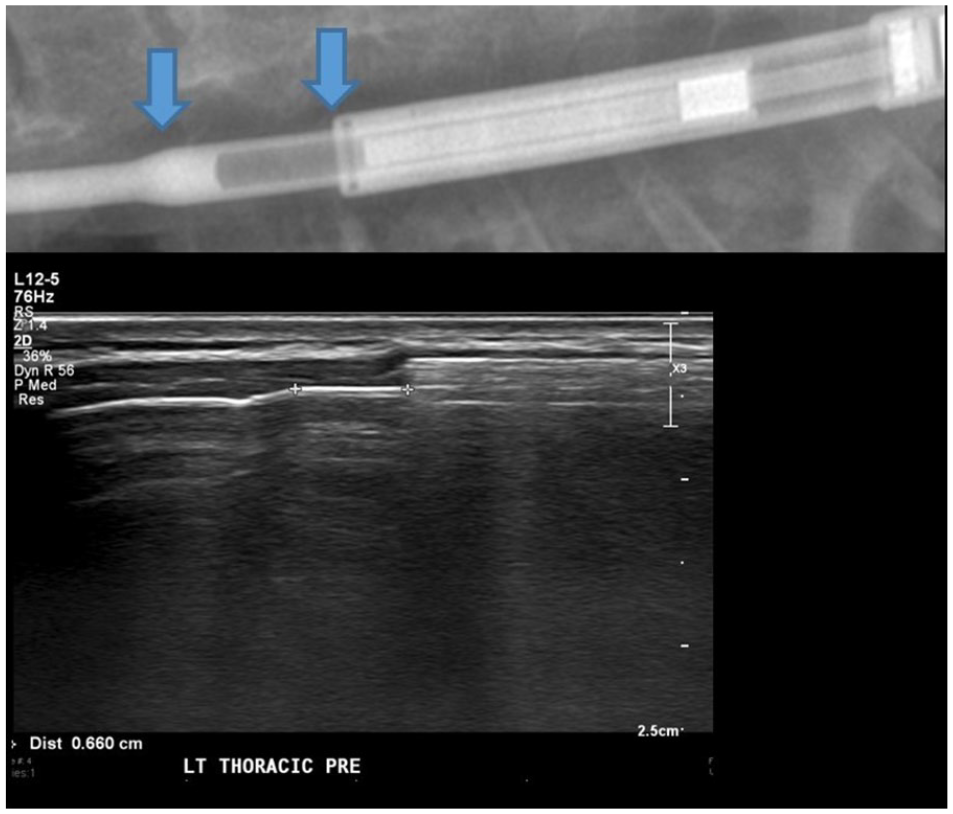
Radiograph with blue arrows indicating the levels where calipers are placed on the corresponding sonogram.
Next, the orthopedic surgeon located the rod’s magnet with a handheld magnet placed over the patient’s back (see Figure 6). Once identified and marked, the external remote controller was then placed over the mark and when activated, caused the rod to rotate and lengthen. This elicited a wobbling sensation for the patient and a distinct rotational sound for the orthopedic surgeon (see Figure 7). Sonographic measurements were repeated once the rod expansion was completed and the difference between the pre- and postmeasurements equaled the actual total length distracted. In some cases, the measurements do not always match the set distance. This mismatch can make an audible sound and usually indicates a slipping of the rod’s internal magnet against a stiff spine, inhibiting a full rotational measurement.9,18

Identifying and marking magnet location.

External remote controller (EMR). The device is placed over the skin and activated to distract the internal magnet, thereby lengthening the rod.
Occasionally, a second distraction was needed. Failure of rod distraction can be due to the rod slipping, cross-talking (if dual rods are placed too close to each other and not offset), an increased distance from the skin to the magnet actuator (body habitus), a gradual loss of effectiveness (most often after the fourth distraction), compete blockage (rod fails to distract), or blockage followed by backtracking (rod fails to distract and slips back). It is most often seen in patients with marked postoperative thoracic kyphosis as well as patients with syndromic or neuromuscular conditions.9,21
Once the worksheet is completed, it can be used to assist the radiologist during interpretation of the images. Additionally, the worksheet is scanned into the patient archiving system (PACS) for future reference.
Data Collection
The effective dose for radiography exams associated with MAGEC rods was estimated by tabulating the radiography unit output as it appeared in the DICOM headers of the image files and was stored on PACS. Dose area product (DAP) was recorded from the DICOM tag (0018, 115e). DAP is given by the air of the beam in cm2 multiplied by the air kerma of the beam measured in mGy. Air kerma is a quantity that is proportional to the intensity of the X-radiation beam. DAP therefore provides a measure of radiation output that incorporates both field size and radiographic intensity.
For each exam, prior to the introducing the sonography MAGEC rod clinic, the DAP was summed from all ionizing radiation exposures to determine the DAP per visit. The technical factors for the radiation exposures varied from patient to patient based on their size as well as the number of exposures per visit, which could have varied from one stitched image to four stitched images. The maximum number of exposures was taken when both an anteroposterior and lateral projection of the patient were taken prior to and following rod distraction as part of a single visit. Total DAP per visit was converted to effective dose by multiplying by a factor, 0.3 mSv/Gy·cm2, to account for average body size and radiosensitivity. This factor was derived in Ernst et al 22 through Monte Carlo simulation. Effective dose may be interpreted as a cancer risk, and the units are millisieverts (mSv).
The times associated with MAGEC rods were obtained directly from the radiographs performed before and after distraction (the time of the first radiograph before distraction and the time of the last radiograph after distraction) for pre-MAGEC rod clinic. The post-MAGEC rod clinic times were taken from the sonograms directly (the time of the first image predistraction to the time of the last image postdistraction).
Statistical Methodology
All statistical calculations were performed in Matlab R2018b (Mathworks, Natick, MA). Confidence intervals for the difference in the mean total study visit times were calculated with a 95% confidence level based on a two-sample t test assuming unequal variances and the assumption of normally distributed data. Ionizing radiation doses were assumed to be log-normally distributed.22,23 Confidence intervals for DAP and effective dose per study visit were calculated according to the modified Cox method, as presented in McDonald et al. 24
For the purposes of this study, it was assumed that the radiation dose delivered to a patient per visit was a random variable, independent of the number of patient visits, for rod distention. This was reasonable because the patient radiation dose was largely dependent on patient size and the amount of image noise that the radiologists were willing to tolerate. Meanwhile, the number of visits a patient had was largely dependent on the patient’s ability to attend regularly scheduled appointments.
The randomness in the effective dose per visit was due to variation in the technical factors for radiation exposures based on patient body habitus. Additionally, the number of ionizing radiation exposures per visit varied from one stitched image to four stitched images for the visits. The maximum number of exposures was taken when both an AP and lateral projection on the patient were taken prior to and following rod distraction in a single visit.
Due to the limited number of patients, there was no attempt made to provide statistics for the number of visits a patient had per year. The ideal schedule for a patient was determined as sonography every other month (six per year) with radiographs every third visit (two per year).
Results
The average age of the patients at the time of implant was 7.5 ± 1.94 years (see Table 1). A total of 21 patients (8 male, 13 female) with a current average age of 11.4 ± 2.82 years were evaluated pre- and postdistraction using either radiographs or sonography from July 2014 to May 2018. The radiation dose per study visit prior to the introduction of the MAGEC clinic was 0.42 ± 0.39 mSv. The CI for the effective dose per visit was 0.33 to 0.63 mSv. Under an ideal schedule, a patient who received strictly sonography for rod distraction could be expected to have two visits with radiographs per year. Without using sonography for rod distraction, a patient could expect to receive six radiographs per year. The 95% CI for the difference of means for six radiographic exams per year versus two exams per year was 1.32 to 2.52 mSv. These statistics assume that the radiation dose per visit is a random variable; the number of study visits per year is fixed.
Patient Characteristics.
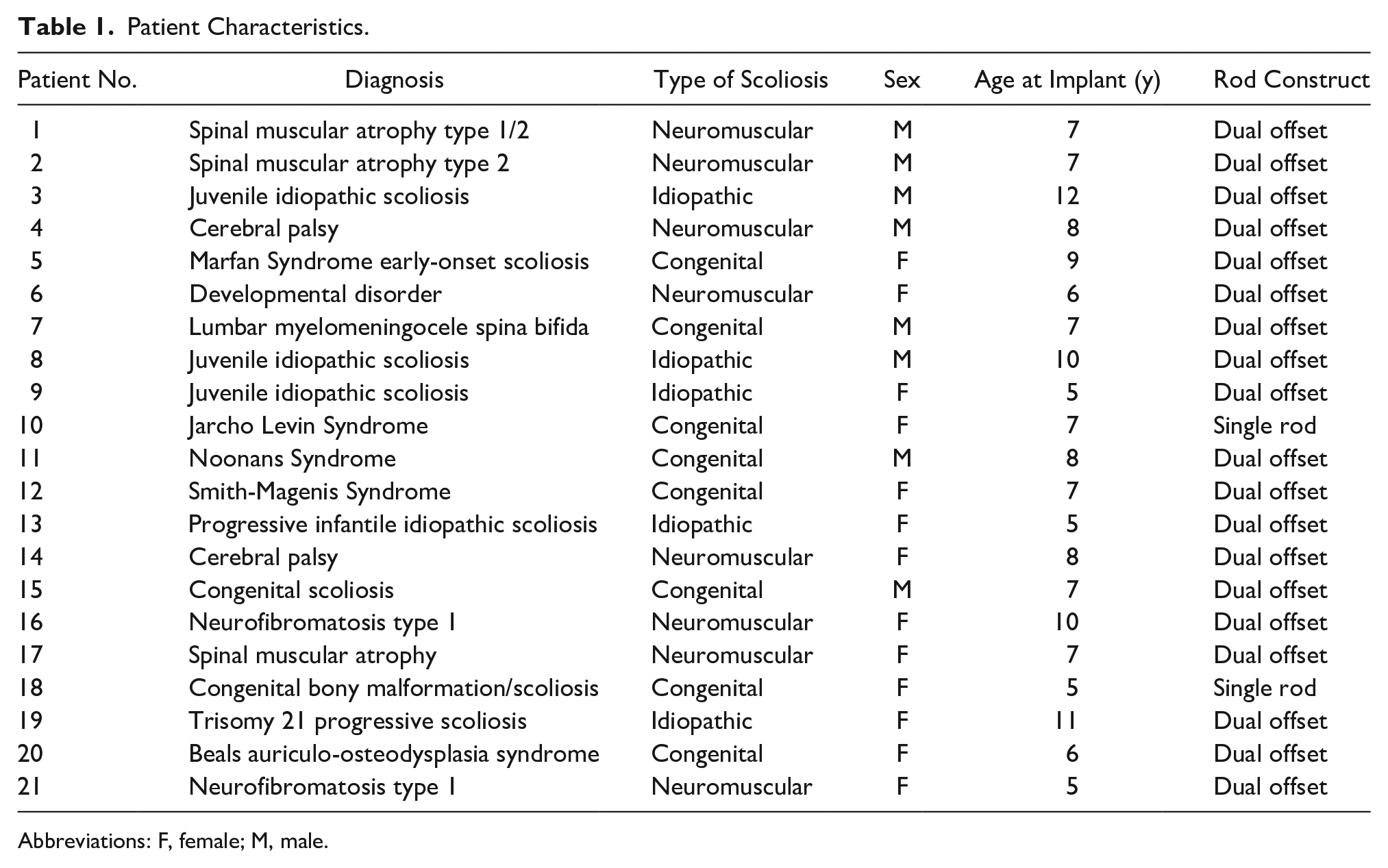
Abbreviations: F, female; M, male.
To evaluate time (see Figure 8), it was recorded on the PACS from the first preradiograph to the end time of the last postradiograph performed on the day of distraction. The pre- and posttimes for sonography completed in the orthopedic clinic were based on the time from entry to exiting the ultrasound department. The result was a 73.7% reduction in the mean study visit time.
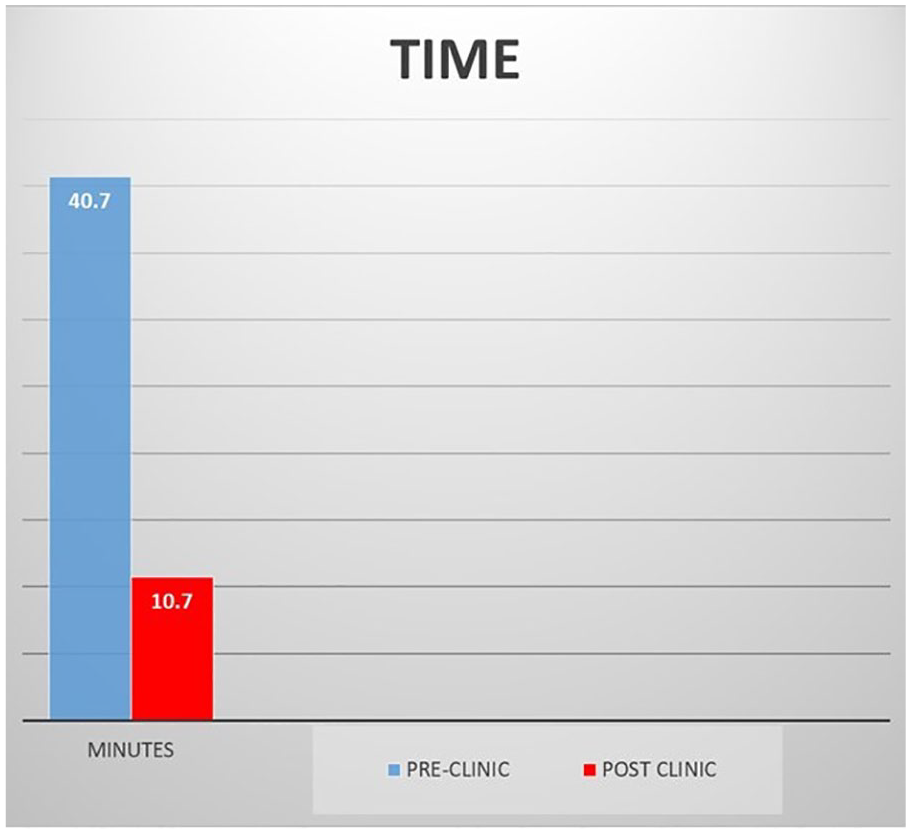
Chart showing pre- and postultrasound implementation imaging demonstrating a 75% decrease in imaging exam time.
The total study visit times for patients who were strictly receiving radiography was 40.7 ± 20.7 minutes. The total study visit times for patients who were strictly receiving sonography after introduction of the MAGEC rod clinic was 10.7 ± 3.7 minutes. The 95% CI for the difference in means of the total visit time was 20.1 to 39.9 minutes.
Discussion
This quality improvement project for a reduction of patient radiation exposure aligned very well with the “ultrasound first” campaign and was linked to the Image Gently Alliance. As a pediatric institution, any time radiation, sedation, or anesthesia can be reduced or eliminated by performing sonography to obtain a same or similar result is a success. This is particularly true in children with chronic conditions that require many hospital visits and imaging exams. The addition of a new sonographic exam not only reduced radiation dose but also became a new revenue source for the ultrasound department.
Although MCGRs are a novel technique, it is worth mentioning that the MAGEC system has a complication rate of 36% to 42%, which improves on TGRs’ complication rate of 58%.25,26 Therefore, it is beneficial to learn this imaging technique given its national growth and overall benefit for children with EOS. Aside from the time savings and improved efficiency, bringing the clinic to the radiology department allowed for cross-training staff (sonographers, nurses, radiologists) on the new exam and flow process. There was a learning curve involved in the imaging of MCGRs that needs to be taken into consideration.20,27 The current study began with more experienced sonographers, but then it enabled more junior staff to learn the protocol. The study team of seven professionals may seem rather large, but it needed to include staff from both the radiology and orthopedic departments. Other departments may find they are able to perform these patient care visits with fewer staff members. An unexpected benefit of the clinic was the strong community of support created in the waiting room among the families with children of similar health challenges. This support also led to the creation of a Facebook page for those families.
There were some limitations to this study. The calculated radiation dose savings and study visit time reduction were based on the study hospital’s patient population and procedures. Because the study was performed in a pediatric hospital, the radiographic techniques were optimized for pediatric patients. If a hospital’s radiologic protocols are not optimized for pediatrics, the radiation dose per patient could be larger. This would underscore a greater potential dose savings by switching to sonography. The dose savings that was stated in this study was likely a conservative estimate of dose savings per visit. The small number of patients in this study limited the ability to provide statistical estimates for the number of visits per patient per year. In presenting dose savings, it is assumed that each patient goes from a schedule of six visits per year with radiographs to a decrease of two visits per year that involve radiographs. This assumption was made without investigating how well patients adhered to this schedule.
When examining the total study visit times, it is possible that other institutions might implement a more efficient process for a visit that only involved a radiograph. The current study presented only savings in total visit time. The savings in the visit time are essentially due to logistical reasons rather than performing radiography or sonography. The actual image acquisition portion of the visits is relatively brief. The time savings result from logistical changes to the imaging process. Other institutions might see greater or lesser time savings than these based on their institutional processes and patient volume. In the first MAGEC rod clinic, the staff imaged eight patients. At their most recent clinic, they were able to image 15 patients with an average of 8.4 minutes per patient. Despite the growth of the study clinic, they have managed to continue to improve time savings.
Conclusion
After implementation of sonography with MAGEC rod expansion procedures, radiation exposure may be reduced by up to 2.5 mSv per year. Additionally, it is possible to decrease imaging time by 73.7%. The added benefits for the physicians and staff were a successful multidisciplinary imaging clinic and the unanticipated creation of a new sonographic examination that aligned with the ultrasound first initiative. As a result of this quality improvement project, the physicians have been able to create a successful imaging clinic that has shown its ability to remain effective and efficient over time despite its growth. Most rewarding was the strong community of support among the families created in the MAGEC rod clinic waiting area. This study illustrates the potential of this quality improvement project and hopefully inspires other children’s hospitals to replicate these services for their patients.
Footnotes
Acknowledgements
The authors extend appreciation to Siddhartha Angadi, PhD, for his data analysis assistance and Andrew Mason, MA, for his data collection assistance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.