
Abstract
Polydactyly is a common congenital malformation of the hand and foot characterized by an extra digit or duplication of digits. Polydactyly can present as preaxial, complex, or postaxial types. It has various presentations, and it can be an isolated anomaly or part of other diseases or syndromic conditions. Incidences are more common in European and Asian descent. The first line of treatment commonly practiced is surgery to create an aesthetically normal functioning hand. In this report, we present a case of bilateral hand polydactyly in a 2-year 6-month-old boy of Asian descent. No other abnormalities or malformations were observed elsewhere in his body. He is otherwise a healthy boy with no family history of malformations. The pattern is not consistent with any syndromic disease. He subsequently underwent surgical resection of the extra digits and a follow-up review showed normal function of the hands without contracture and other complications of the surgical site.
Keywords
Introduction
Polydactyly is a congenital anomaly resulting in supernumerary fingers and/or toes. It is also referred to as hyperdactyly. Polydactyly is classified into preaxial, complex, and postaxial types. 1 Preaxial polydactyly (PPD), the most common type, refers to the duplication of the first digital ray. Postaxial polydactyly (PAP) is a congenital hand malformation characterized by fifth-digit duplications in the hand and/or feet. 2
While PPD is more common in people of European and Asian descent, postaxial polydactyly is more common in African heritage. 3
It is more common in African populations with an incidence of one in every 100–300 live births compared to Caucasian children in which the incidence of postaxial polydactyly is one in every 1500–3000 live births.4,5 In those of African descent, postaxial polydactyly tends to be bilateral in the majority of cases and is usually isolated and autosomal dominant. In other populations, it tends to be unilateral and sporadic. 5 The clinical presentation may vary. It may present as an isolated condition or part of another disease condition or congenital syndrome.
Case presentation
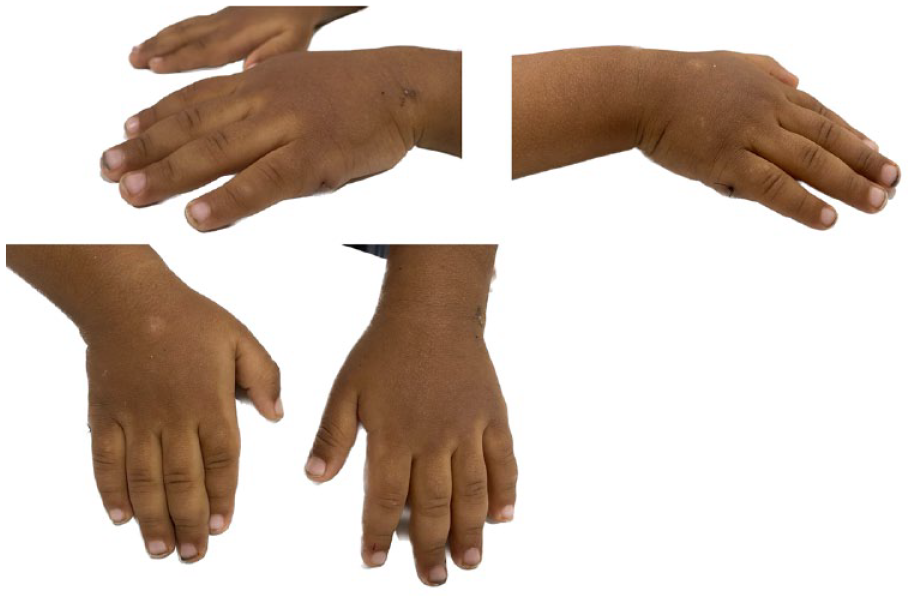
A mother presented to our orthopedic Out patient department with her 2-year 6-month-old boy complaining of extra growth of fingers on both hands. The toddler is otherwise healthy. No other abnormalities were detected elsewhere in the body at birth and thereafter. He is the middle child and has a younger sister and elder sister who is medically free with no history of polydactyly. He is of Asian descent and there is no family history of similar deformities or any genetic disorders. On examination, a postaxial extra digit was noted in bilateral hands (Figure 1). It was noted to be a rudimentary digit with a soft tissue Skin Bridge. The function of the digit was intact with active flexion and extension, and hand grip ability. There were no skin creases noted at the affected site at the Metacarpophalangeal joint region.

Preoperative clinical picture of patient’s bilateral hands showing extra postaxial digits.
Written and informed consent was obtained from the mother of the minor patient for anonymized patient information to be published in this article.
X-rays of the bilateral hand revealed postaxial polydactyly without bony involvement (Figure 2).

A radiograph of the bilateral hand showed postaxial polydactyly.
Preoperative evaluation revealed no other underlying conditions and the boy was considered healthy with no other abnormalities and malformation detected. The child was operated under general anesthesia. An elliptical incision was made. Dissection was done, and the vessels supplying the extra digit were ligated and excision of the pedunculated postaxial digit was performed. There was no nerve identified that supplied the extra digit. The wound was closed using 4-0 nylon Ethicon (Figure 3).

Post-excision of the extra postaxial digit from bilateral hand.
Immediate postoperative follow-up and review at the orthopedic ward were uneventful. The patient was admitted for 2 days following surgery for observation of any complications at the surgical site. Wound care was provided at the ward.
The patient was advised to follow up on postoperative day 7 for wound evaluation. On follow-up examination, the surgical site wound was noted to be healthy and healed with no other complications (Figure 4). The child’s range of motion of the hand and function was intact as it was preoperatively. He did not have any pain or tenderness at the surgical site. The suture was removed on postoperative day 10 and the patient was advised to resume normal activity of the hands. Follow-up after a period of 1 month showed no adverse events. The functional outcome was noted to be good.
Follow-up of the patient after a week post-excision of polydactyly.
Discussion
The clinical presentation of polydactyly may be classified as syndromic or non-syndromic. It may present as a non-syndromic condition that is an isolated condition or syndromic, as part of other disease conditions or congenital syndrome. 6 For polydactyly cases associated with other diseases or syndromes, a genetic workup and thorough medical examination are recommended when available.
Non-syndromic polydactyly is classified as pre-axial, complex, and PAP as represented in Figure 5. PPD is associated with GLI3 on the chr7p13 and SHH on the chr7q36 gene. PAP is associated with GLI3 on chr7p13, and PAPA2 and PAPA3 on chr13q21-q32 and chr19p13.2-p13.1 gene, respectively. It is also associated with SHH mutations, MIPOLI, and PITXI. 1
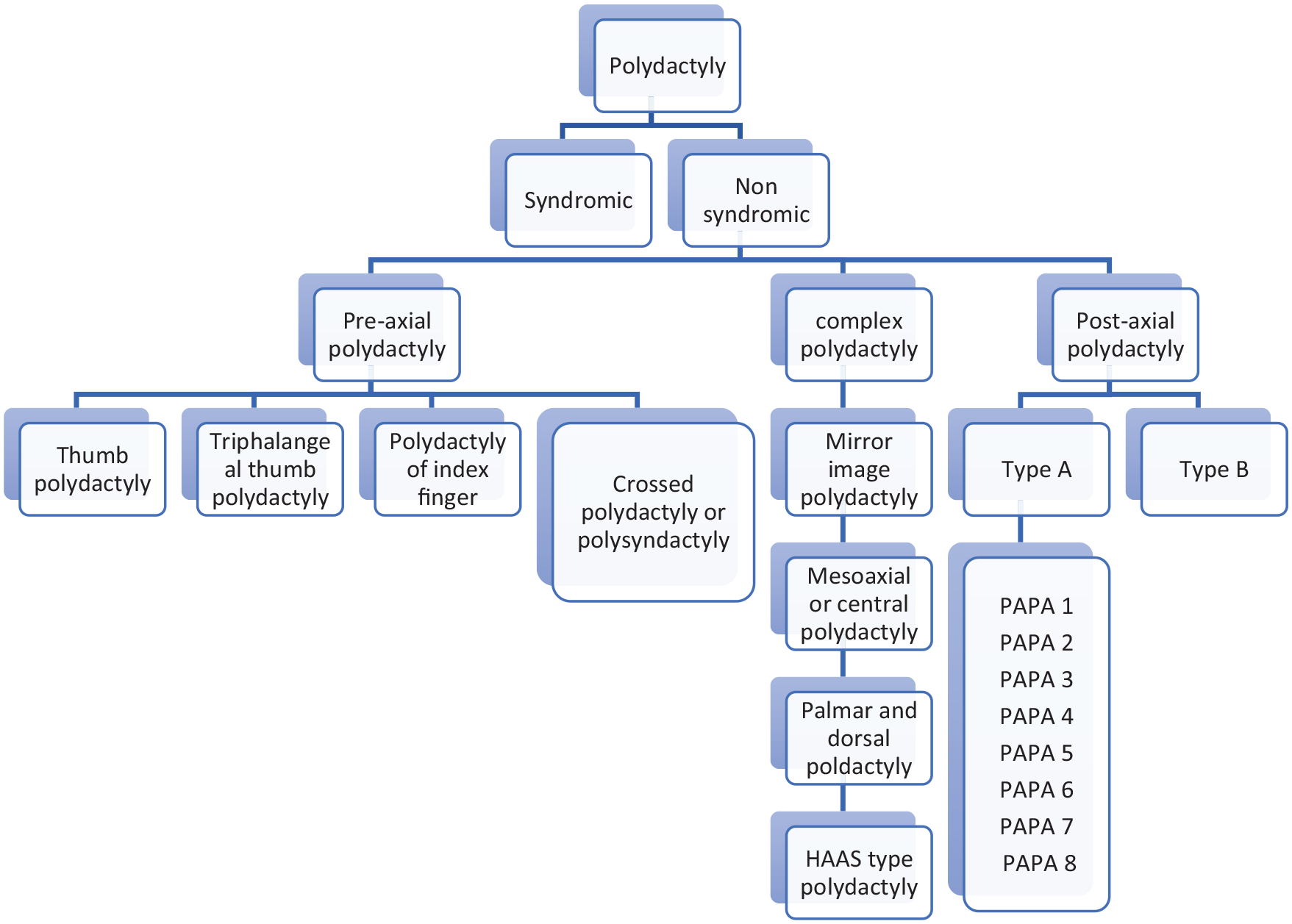
Types of polydactyly classification as per Temtamy and MCKusick. 6
Temtamy and McKusick scheme classifies polydactyly into three types, that is, PPD, PAP, and complex types. PAP is 75% more common than PPD, and about 8% of bilateral PAP cases with lower and upper limbs are associated with many other congenital syndromic defects. 6
Two phenotypic varieties of postaxial polydactyly described by Temtamy and McKusick are type A (PAP A) and type B (PAP B).2,3,6,7 In type A, the extra digit is well formed and articulates with the fifth metacarpal/metatarsal (bifid) or an extra metacarpal/metatarsal. Type B is characterized by a rudimentary extra fifth digit and is usually represented by an extra skin tag. The vestigial sixth finger is attached by a narrow neurovascular pedicle to the lateral aspect of the hand or foot at the level of the metacarpal-phalangeal joint or the metatarsal-phalangeal joint. Postaxial polydactyly type B: It is the most common type of polydactyly.3,2,6
Treatment options for PAP depend on the type and the underlying features. To guide the surgical management, postaxial polydactyly is further classified as per Stelling and Turek classification. 8 Type 1 denotes a rudimentary digit attached via a soft tissue skin bridge. Type 2 refers to partial duplication in which the normal digit articulates with an osseous structure. Type 3 represents the complete duplication where there is a fully developed extra digit.
A careful physical examination will provide all the necessary information. The presence or absence of a well-formed osteoarticular base to the extra digit will guide treatment. Radiographs of the affected limb are recommended to know the nature of the osseous involvement of the extra digit. This will guide the preoperative surgical planning.
In cases where the polydactylous finger is well formed and connected by more than just a skin pedicle, examination of the flexion and extension creases over the interphalangeal joints will provide information regarding joint formation and tendon function; in cases where the digit is extended, stiff, and without skin creases, it is unlikely that any meaningful flexor or extensor tendons are attached to the extra finger. 3
The objective of the surgery is to enhance cosmesis and improve the function of a single finger. While some families/patients choose not to treat postaxial polydactyly due to personal, cultural, or religious reasons, in most situations, surgery is recommended to remove the extra digit and provide a more aesthetically normal, functioning hand. 3
The surgery is typically performed around 1 year of age, before the development of pinch and fine motor function. Although a congenital condition, some patients may be seen for the first time in adulthood. Excision must be carefully carried out to prevent complications. 9
There is no gold standard management of postaxial polydactyly and the treatment options range as per the presentation and type of postaxial polydactyly. The management of postaxial polydactyly ranges from suture ligation to surgical excision depending on the contents of the extra digit. 10 Ligation is a safe and effective option when the extra digit is mainly composed of soft tissues. 11 After the suture ligation, there is an increased risk of painful neuroma formation. Surgical excision is an alternative for postaxial polydactyly to avoid neuroma formation. 1 The first line of treatment is surgical resection and reconstruction taking into account the type and severity of duplication and the digits involved. 8
This case report depicts an isolated presentation of postaxial polydactyly, which is noted in bilateral hand and there is no family history to suggest an autosomal dominant mode of inheritance. Molecular and genetic studies could not be performed due to the unavailability of such cases in the country. In this case, since the duplication was mainly via soft tissue attachment, surgical resection was performed rather than ligation, and the postoperative outcomes were promising.
Early ligature in such a case would have been more advantageous had the patient presented earlier. Ligation can be easily performed without the need for anesthesia. There may be the possibility of a small risk of infection and bleeding. The ligated site may be aesthetically displeasing due to the remnant of soft tissue. Surgical excision can prevent this minor complication of bleeding as it allows for coagulation or ligation of the vessels and prevents neuroma by transection of nerve if any is present in the pedicle. However, surgical excision requires anesthesia, and complications related to anesthesia may be inevitable. Therefore, the optimal treatment of type B PAP cannot be concluded.
More cases may need to be observed to conclude the optimum mode of management and the functional outcome.
Conclusions
Polydactyly is the most common congenital hand anomaly with PPD being more common than central and PAP. The two variants of PAP are type A and type B, type B being more common. Although most studies suggest surgery is usually the main modality of treatment in polydactyly, it is controversial in the case of postaxial polydactyly. Some surgeons prefer suture ligation to surgical resection for PAP.
In this case report of isolated, bilateral PAP, surgical excision of the extra digit was performed with excellent postoperative results. The patient was followed up for any postoperative complications including contracture, deformities, and function to ensure a good outcome of the surgery. Polydactyly may be associated with other disease conditions or syndromes. Therefore, a thorough preoperative assessment with detailed physical examination and radiological imaging is required for surgical planning and to avoid complications and improve function postoperatively. The treatment plan depends on the type of the PAP and surgeon’s preference after discussing it with the patient and the family. The patient should be followed up for early detection of any complications. The functional outcome in our case was excellent.
Footnotes
Acknowledgements
The author is grateful for the cooperation of the patient and the guardian in providing consent for this report.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Human ethics
Written informed consent was obtained from the child’s guardian (Mother).
Informed consent
Written and informed consent was obtained from the mother of the minor patient for anonymized patient information to be published in this article.