
Abstract
Portal hypertensive cholangiopathy is a rare complication of extrahepatic portal vein obstruction and portal cavernoma. It is usually asymptomatic but may be associated with jaundice, biliary colic, and fever. Abdominal sonography and Doppler are ideal initial diagnostic modalities, followed by magnetic resonance cholangiopancreatography or endoscopic retrograde cholangiopancreatography. These imaging modalities are important if an intervention is planned for the management of portal hypertension and for relieving biliary obstruction. If computed tomography (CT) is performed in isolation, it may be challenging to distinguish this entity from acute on chronic portal vein thrombosis. The diagnostic results should be interpreted cautiously. This case report of an abdomen CT performed on a patient with a history of portal vein thrombosis masqueraded as an acute on chronic portal vein thrombosis with cavernous collaterals. Doppler confirmed the diagnosis of portal hypertensive cholangiopathy. Correlation with clinical symptoms and Doppler may be necessary to distinguish portal hypertensive cholangiopathy from acute portal vein thrombus.
Keywords
Portal hypertensive cholangiopathy, also known as portal biliopathy, portal cavernoma–associated cholangiopathy, or pseudosclerosing cholangitis, is a consequence of portal hypertension due to extrahepatic portal vein obstruction. It may present as abnormalities in the extrahepatic and intrahepatic biliary tree. It occurs due to mechanical compression of bile ducts and ischemia caused by altered vascularization.1,2 Most of these patients are asymptomatic, but 5% to 38% of affected individuals develop jaundice, cholelithiasis, cholangitis, or even biliary cirrhosis. 3 The most commonly used diagnostic modalities include abdominal or endoscopic ultrasonography (EUS) with Doppler, computed tomography (CT) of the abdomen, and endoscopic retrograde cholangiopancreatography (ERCP). As the spectrum of radiologic findings can be broad and include dilatation, stricture, angulation, and irregularity of the biliary duct, this clinical entity can be difficult to diagnose. This is a case report of an abdomen CT performed on an asymptomatic patient with a history of portal vein thrombosis, masquerading as acute on chronic portal vein thrombosis. The use of Doppler sonography confirmed the diagnosis of portal hypertensive cholangiopathy.
Case Report
A 46-year-old asymptomatic woman presented to a hematology clinic for a second opinion regarding long-term anticoagulation due to a history of portal, superior mesenteric, and splenic vein thrombosis, previously diagnosed seven years ago. The splanchnic vein thrombosis was considered to be secondary to an appendectomy complicated by sepsis and small bowel ischemia. This required that the patient undergo a repeat laparotomy, with small bowel resection and ileostomy. Medical laboratory testing, performed at the time of this incident, provided a hypercoagulable workup and was used to investigate an underlying congenital or acquired thrombotic diathesis. The overall results were unremarkable, except for a small 4% clone of JAK2 V167F mutation in peripheral blood leukocytes. There was no morphologic evidence of myeloproliferative neoplasm (MPN) on bone marrow biopsy. The patient remained on anticoagulation for three years, but in the meantime, she developed gastrointestinal bleeding from esophageal varices and two episodes of an intracranial hemorrhage. Based on these side effects, anticoagulation therapy was discontinued. Tests performed during the current evaluation included magnetic resonance imaging (MRI) of the brain that revealed a left thalamic/periventricular arteriovenous malformation. This abnormality was subsequently surgically resected. An esophagogastroduodenoscopy (EGD) and colonoscopy showed esophagitis and small esophageal varices. Abdomen and pelvis CT venogram demonstrated an apparent filling defect that was interpreted as an acute or subacute nonocclusive thrombus in the portal vein. This defect extended into the right and left portal veins along with chronic portal, superior mesenteric, and splenic vein thrombosis, with cavernous transformation and collateral vessels (Figure 1A,B). As the patient was asymptomatic, there was reluctance to reinitiate anticoagulant therapy due to her history of hemorrhagic complications. Therefore, given the patient’s history, additional imaging studies were performed. Doppler sonography of the abdomen and pelvic vessels revealed several small venous collaterals surrounding the bile duct and a chronically occluded portal vein, which could be seen with portal hypertensive cholangiopathy. There was no evidence of acute or subacute portal vein thrombus (Figure 2). Since the patient had no clear evidence of an acute or recurrent portal vein thrombosis, overt MPN, but had a significant bleeding risk, she was not recommended to restart anticoagulation.
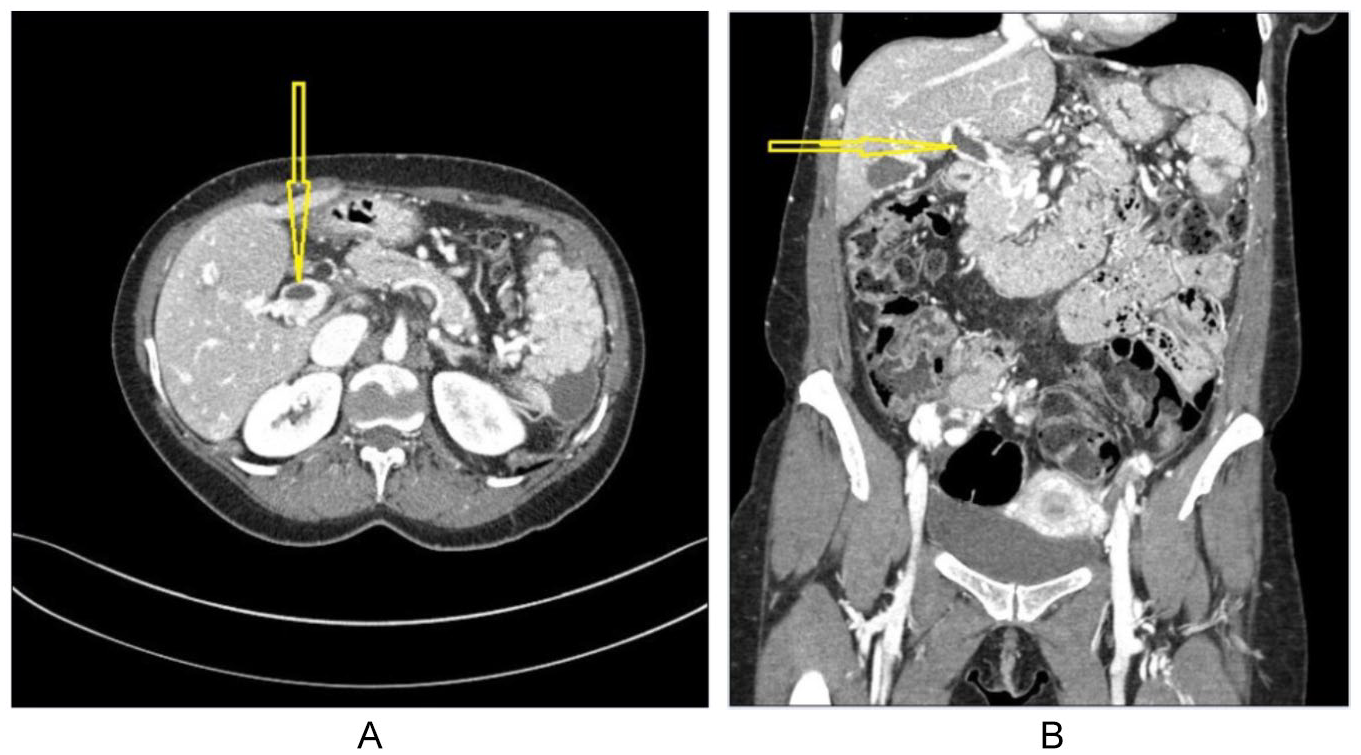
(A) Axial plane of a contrast-enhanced abdominal computed tomography (CT) image demonstrating an “apparent venous filling defect” (yellow arrow) that was interpreted as an acute or subacute nonocclusive thrombus in the main portal vein. (B) The same “apparent filling defect” is visualized on the coronal plane of CT venogram (yellow arrow).
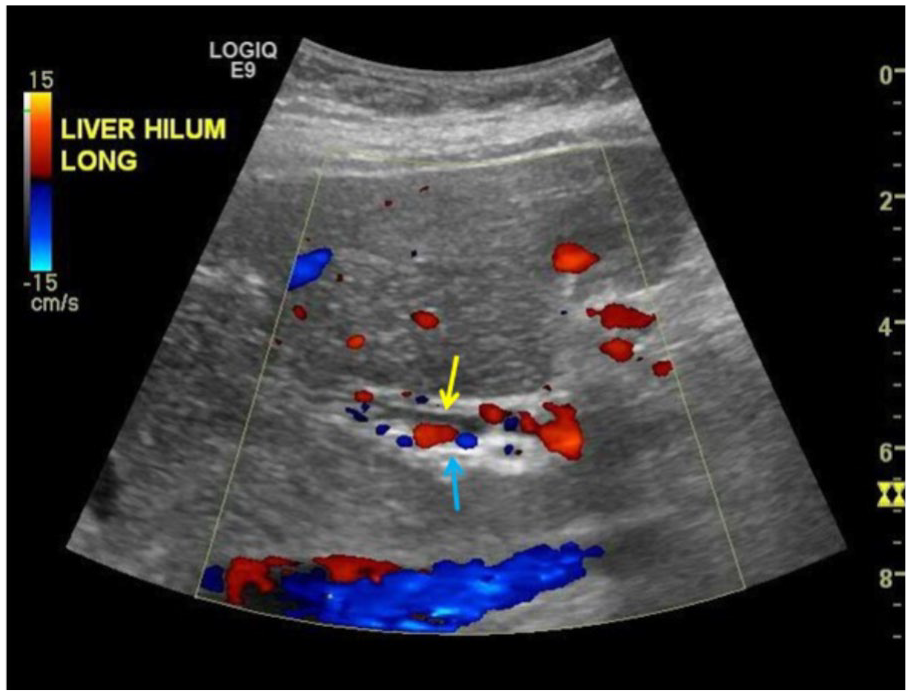
Color Doppler sonography indicates multiple venous collaterals (blue arrow) surrounding the bile duct (yellow arrow). The main portal vein is chronically occluded and no acute thrombus is present.
Discussion
Portal hypertensive cholangiopathy was first reported in 1944 by Fraser and Brown. 4 It is an anatomical and functional abnormality of part or the entire biliary tract, which may include the intrahepatic and extrahepatic bile ducts, cystic duct, and gallbladder. This is more common in patients with extrahepatic portal vein obstruction (EHPVO) and with a portal cavernoma. EHPVO is vascular blockage at a prehepatic level, which develops after a prothrombotic event, intra-abdominal infection, catheterization of the umbilical vein, or portal vein anomaly, such as with atresia or stenosis. A portal cavernoma forms when thrombosis of the portal vein is rapidly followed by a compensatory attempt to restore intrahepatic blood flow by recanalization of the portal vein. It may also cause the development of new collaterals around the occluded vein, which also engulf the surrounding biliary system. 5 This can lead to scarring of the biliary duct lining, causing strictures, and cholangiectasias.6,7 The left hepatic duct is more commonly and severely affected (55%–100%) compared to the right hepatic duct (40%–56%). 3
Portal hypertensive cholangiopathy occurs in 78% to 100% of patients with EHPVO, 8 but it is rare in cirrhotic portal hypertension, where blocking of portal circulation occurs at the level of the hepatic sinusoid. 7 Only 5% to 38% of individuals are symptomatic and develop jaundice, recurrent abdominal pain, fever, cholangitis, and cholecystitis, which are the most common presentations. Older age, longer duration of disease, gallstones, common bile duct calculi, and abnormal liver function tests are associated with an increased risk of symptomatic presentation. 3 The diagnosis of portal hypertensive cholangiopathy can be established based on diagnostic imaging results, especially magnetic resonance cholangiopancreatography (MRCP), ERCP, abdominal or EUS with Doppler, or CT.
ERCP was considered the gold-standard diagnostic test, but due to its invasive nature, radiation exposure, and risk of complications, it has been replaced by less invasive diagnostic modalities. Reported cholangiographic abnormalities include biliary ductal extrinsic indentations, shallow indentations, irregular ductal contour, strictures, filling defects, bile duct angulations, upstream dilatations, and ectasia. 8
MRCP is a less invasive imaging modality and excludes other possible disorders of the liver and biliary tracts, including neoplasms, stones, or varices. It is as accurate as ERCP in delineating biliary abnormalities and the relationship of biliary changes with collateral veins, and it helps identify a shuntable vein. 3 Currently, ERCP is performed only when endoscopic therapy is planned, especially when a common bile duct stone is discovered on noninvasive diagnostic tests or in the presence of cholangitis.
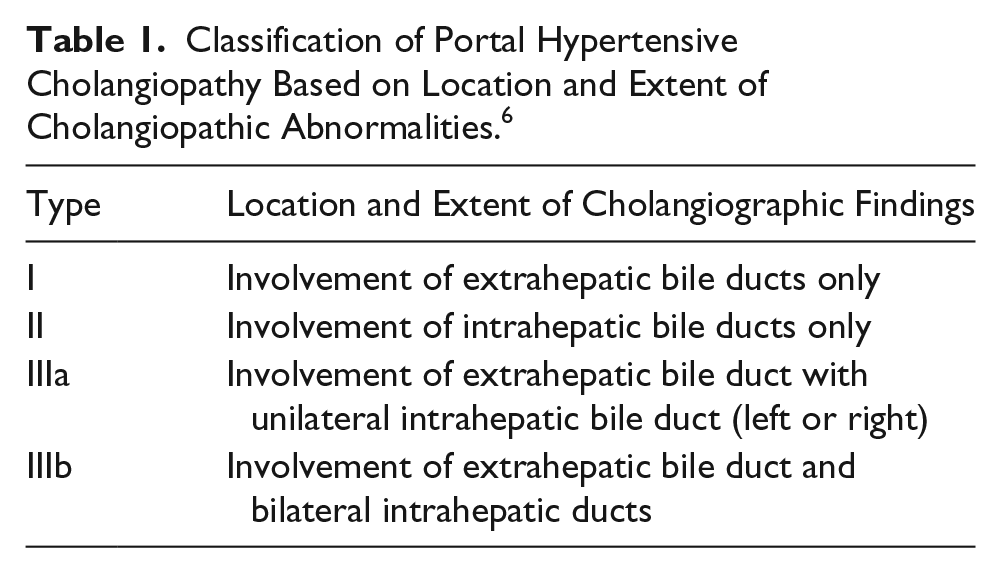
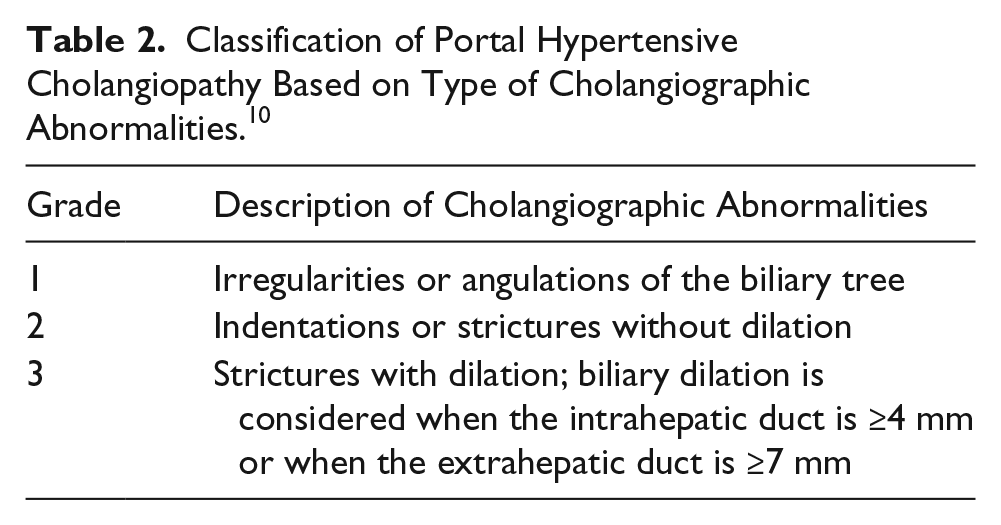
Some authors have proposed a classification of portal hypertensive cholangiopathy based on the location and extent of cholangiopathic abnormalities. These classifications are as follows: type I, changes that affect extrahepatic bile ducts only; type II, changes in only the intrahepatic bile ducts; type IIIa, changes in the extrahepatic bile duct with the unilateral intrahepatic bile duct; and type IIIb, changes in the extrahepatic bile duct and bilateral intrahepatic ducts (Table 1). Other authors have graded severity of the portal hypertensive cholangiopathy based on type of abnormalities. Presence of irregularities or angulations of the biliary tree is classified as grade 1, indentations or strictures without dilation as grade 2, and strictures with dilation as grade 3 (Table 2).
Classification of Portal Hypertensive Cholangiopathy Based on Location and Extent of Cholangiopathic Abnormalities. 6
Classification of Portal Hypertensive Cholangiopathy Based on Type of Cholangiographic Abnormalities. 10
Abdominal sonography with Doppler is frequently the initial diagnostic test as it is noninvasive, inexpensive, and safe. It helps to visualize the portal vein cavernoma, which can be depicted as multiple tortuous structures in the porta hepatis, with color and spectral Doppler. The abnormalities in the common bile duct and common hepatic duct are mainly strictures and ductal caliber irregularities, whereas intrahepatic ducts are frequently noted to be dilated, likely secondary to extrahepatic obstruction. 9 Spectral Doppler analysis helps distinguish the tortuous vascular cavernoma form the tubular biliary duct. In addition, abdominal sonography can be useful in detecting gallbladder varices. EUS occasionally helps identify bile duct stones, strictures, varices, or tumors when other diagnostic modalities are not revealing pathology.
A CT is inferior to MRCP for describing biliary anatomy, compared to abdominal sonography with Doppler, as it can be misleading in differentiating acute nonocclusive portal vein thrombus from cavernous collaterals, as presented in this case study.
Currently, treatment of portal hypertensive cholangiopathy is reserved for symptomatic patients only. Asymptomatic individuals with normal liver function tests can be carefully observed. Signs of infection, abdominal pain, and rising alkaline phosphatase require further investigation, and abdominal sonography and MRCP are initial diagnostic modality choices. If a common bile duct stone or choledochal stenosis is suspected, further endoscopic or occasionally surgical treatment is warranted. The goal is to relieve biliary obstruction and improve portal hypertension. Endoscopic procedures include sphincterotomy, stone extraction, mechanical lithotripsy, biliary stricture dilatation, stent, or drain placement. If successful, most patients become asymptomatic, but some will require periodical stent exchange. In case of endoscopic treatment failure, surgical management is considered in the form of portosystemic shunt placement, second-stage biliary bypass, or rarely liver transplantation.1,3,7
Conclusion
Portal hypertensive cholangiopathy may masquerade as acute-subacute portal vein thrombosis on CT. Correlation with clinical symptoms and Doppler sonography of the portal venous system and biliary ducts may be necessary to distinguish this entity from an acute portal vein thrombus.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.