
Abstract
A case is described of a patient who presented with signs and symptoms suggestive of endometriosis. She underwent a diagnostic laparoscopy, which failed to identify any features of endometriosis. The patient subsequently underwent a 3D transvaginal sonogram that demonstrated evidence of a deep infiltrating endometriosis, affecting the right uterosacral ligament. This case demonstrates the diagnostic ability of 3D transvaginal sonography and, at the same time, the potential deficiency of laparoscopy to make the diagnosis of deep infiltrating endometriosis.
The diagnosis of deep infiltrating endometriosis (DIE), indicating the presence of retroperitoneal endometrial glands and stroma, is often difficult to make, due to the range of symptoms and presentations associated with this pathology. When peritoneal endometriosis exists, the definitive diagnosis can usually be made from laparoscopic visualization and/or histologic sampling. However, the existence of DIE can sometimes be missed because the presence of endometriotic implants in anatomic sites is not easily visualized laparoscopically (e.g., retroperitoneal rectal lesions or intra-uterosacral ligament endometriosis). A case is described in which diagnostic laparoscopy did not demonstrate the presence of endometriotic lesions in a patient with symptoms consistent with that diagnosis. Fortunately for this patient, 3D transvaginal sonography (3DTVS) was performed, revealing that diagnosis and allowing for therapeutic measures to be offered to the patient.
Case Report
The patient is a 46-year-old G2 T2 P0 A0 L2 woman with a previous history of tubal ligation and appendectomy. She presented to the emergency department with 1 week of acute pain and lower abdominal pain, occurring over the past month, located primarily in the right lower quadrant. As the primary care team had thought the pain may have been due to constipation, according to imaging that was performed and their clinical assessment, they provided an aggressive bowel regimen, but the pain persisted despite this treatment. Of note, a diagnosis of endometriosis had been made many years previously. The department of gynecology was then consulted for further evaluation. After a 2D pelvic sonogram failed to identify the right ovary, laparoscopy (Figure 1) and a bilateral salpingectomy were performed. Laparoscopic visualization failed to reveal any evidence of endometriosis, and pathologic examination of the fallopian tubes revealed normal histology. A 3DTVS was subsequently performed, revealing evidence of DIE (Figures 2 and 3). A Voluson E8 system (GE Healthcare Ultrasound, Milwaukee, WI) with transvaginal probe (RIC 5- to 9-MHz transducer) was used for this imaging. A plan for the future management of this diagnosed condition, which had not yet resolved at the time of publication, was discussed with the patient.

Normal laparoscopic findings of patient. Note the absence of any visible signs of endometriotic lesions on the ovaries, tubes, peritoneum, or cul-de-sac.
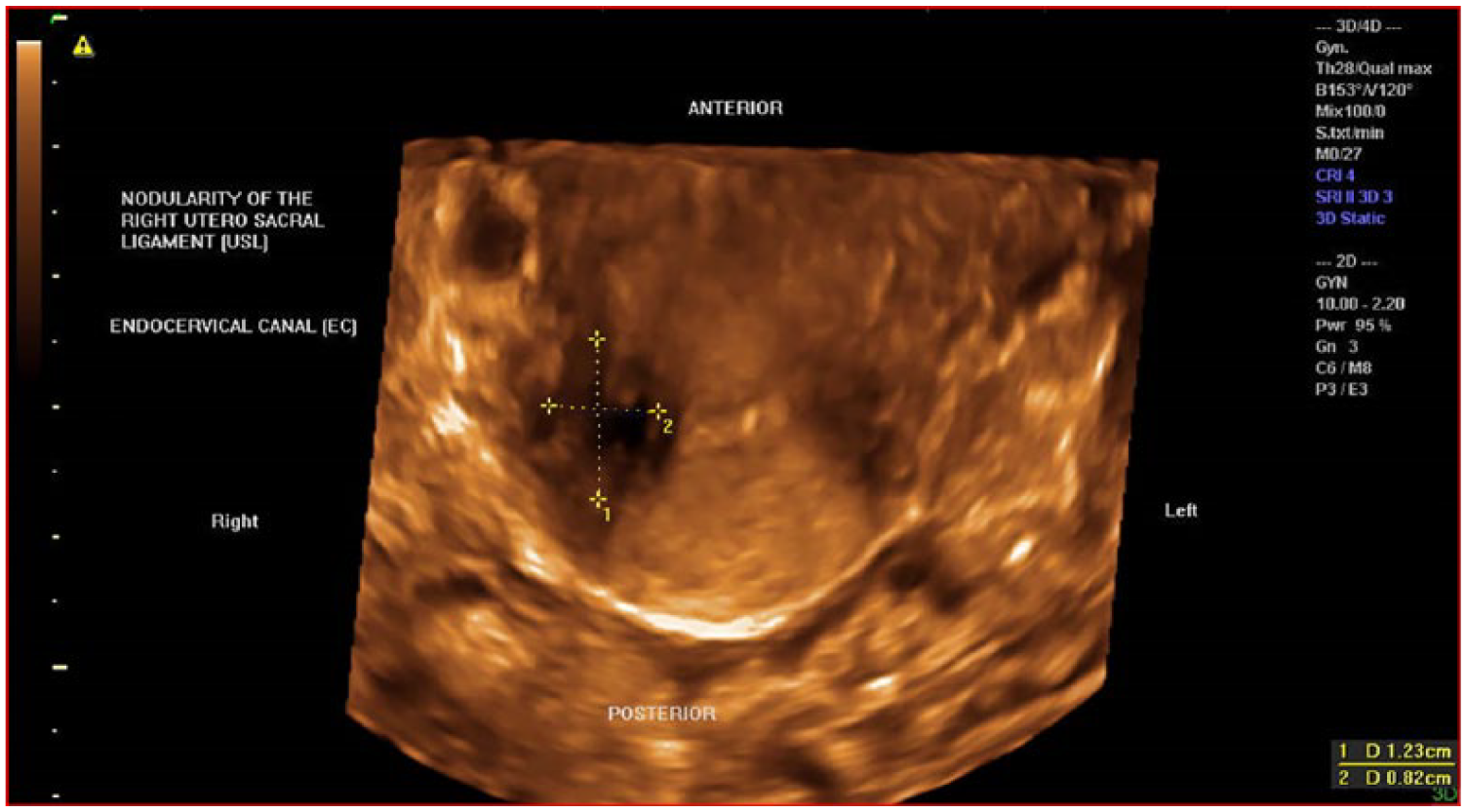
3DTVS rendering mode of the transverse view of the cervix demonstrating a nodularity of the right uterosacral ligament (USL) measuring 1.23 × 0.82 cm, subsequent to laparoscopic visualization.
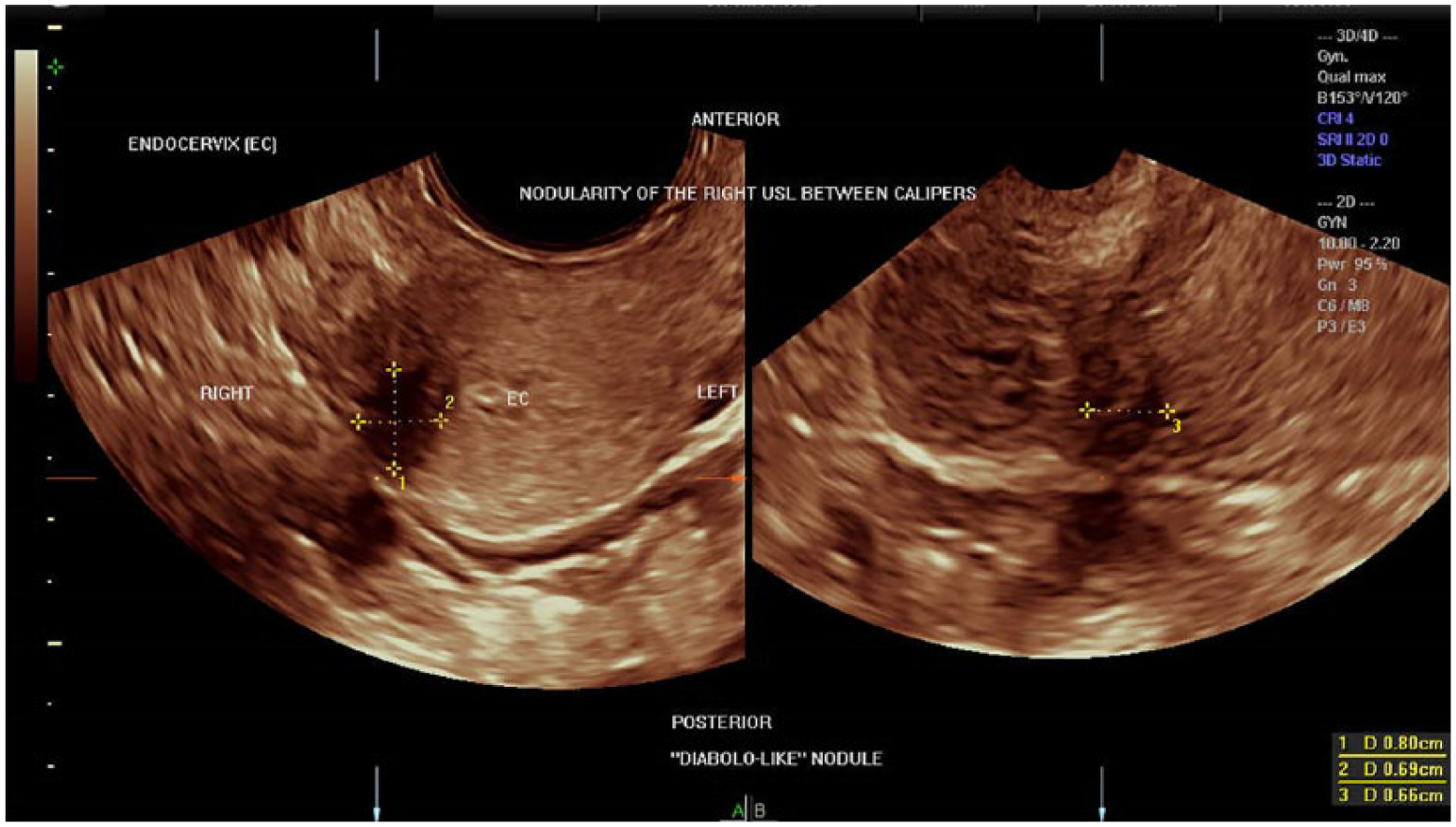
2D image obtained from a 3D volume manipulation demonstrating a nodularity of the right uterosacral ligament between calipers in a combination of two planes: transverse volume acquisition of the cervix on plane A and right parasagittal of the cervix on plane B.
Discussion
Endometriosis, which can disturb the lives of many women, is at times difficult to clinically diagnose. Surgical confirmation of the clinical diagnosis of endometriosis is often thought to be best done via laparoscopy. 1 However, laparoscopy being considered the “gold standard” for its diagnosis has recently been questioned, 2 since DIE can possibly exist without its laparoscopic visualization in symptomatic patients. This is due to the possible presence of retroperitoneal endometriotic lesions (i.e., outside of the peritoneal cavity). While superficial peritoneal and ovarian endometriosis can be seen laparoscopically, DIE cannot often be visualized. Instead, a variety of imaging tools have been evaluated for the ability to diagnose this condition.3–8 Of course, 2D transvaginal sonography (2DTVS) can often noninvasively illustrate the presence of ovarian endometriomas. 9
However, the use of 3DTVS has been shown to be effective for at least making the diagnosis of this variant of endometriosis, which is necessary before treating this condition, medically or surgically. Though there may be a degree of operator dependence, for image quality, there are steps that can be followed that can result in a diagnostic benefit.10,11 With the increasing availability of 3DTVS, it should be used to diagnose this condition, so effective therapeutic measures can be offered to patients who may have continued to suffer from the associated chronic pelvic pain, dysmenorrhea, and dyspareunia, with which it is often associated.
Surgical treatment of DIE has been associated with difficulty and complications.12–16 The optimal treatment of DIE will likely continue to be debated until practical trials are performed comparing medical and surgical therapies, resulting in definitive evidence. However, this may be difficult, since several choices of medical and specific surgical treatments are available, many of which can be used in combination (e.g., laparoscopic excision followed by gonadotropin-releasing hormone agonists). Given the difficulties and complications that can often accompany the surgical procedures employed for the removal of ectopically placed endometriotic tissue, its optimal treatment may still need to be determined. Producing evidence-based treatment comparisons will likely be quite challenging. The earlier a diagnosis can be made, the earlier optimal therapy can be provided, and further suffering and internal spread of this condition (i.e., endometriosis) can be limited. Therefore, the proper diagnosis of this potentially complicated condition is the first step in its ideal management.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.