
Abstract
Carotid body tumors (CBT) are a rare form of paragangliomas of the head and neck. They are described as rare, slow-growing, mostly benign, clinically silent tumors of neural crest cells. This tumor should be considered as a differential diagnosis when evaluating a lateral neck mass. A report of a rare case, a carotid body tumor, is presented that was incidentally noted as a lateral neck mass during a screening sonogram. A mass located at the level of the left carotid bifurcation demonstrated significant vascular flow with the use of contrast enhanced ultrasound (CEUS) techniques. Computed tomography angiography (CTA) was also performed to further analyze the tumor’s anatomical relation to the extra cranial vessels.
Case Report
A 72-year-old female with a past medical history of hypertension and hyperlipidemia presented to the cardiology office for a consultation. The patient was noted to have carotid atherosclerotic plaque seen on an outside screening examination. She was asymptomatic at presentation for the sonogram. To further evaluate this abnormal screening exam result, a carotid duplex imaging was performed. The carotid duplex gray-scale imaging showed that her right and left common and internal carotid arteries contained very mild atherosclerotic plaque. Additionally, a 1.6 × 1.8 × 1.5 cm mass was noted at the left common carotid bifurcation (Figure 1).
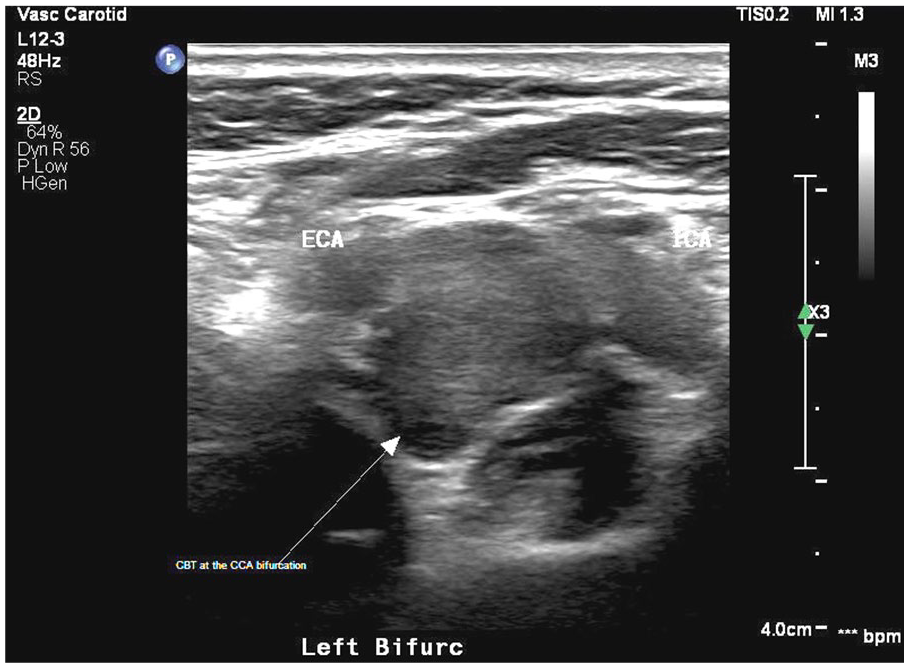
Short-axis view showing the carotid body tumor at the common carotid artery bifurcation as demonstrated by carotid duplex gray scale sonogram.
Pulsed wave spectral Doppler analysis revealed a low-resistance flow signal within the mass (Figure 2).
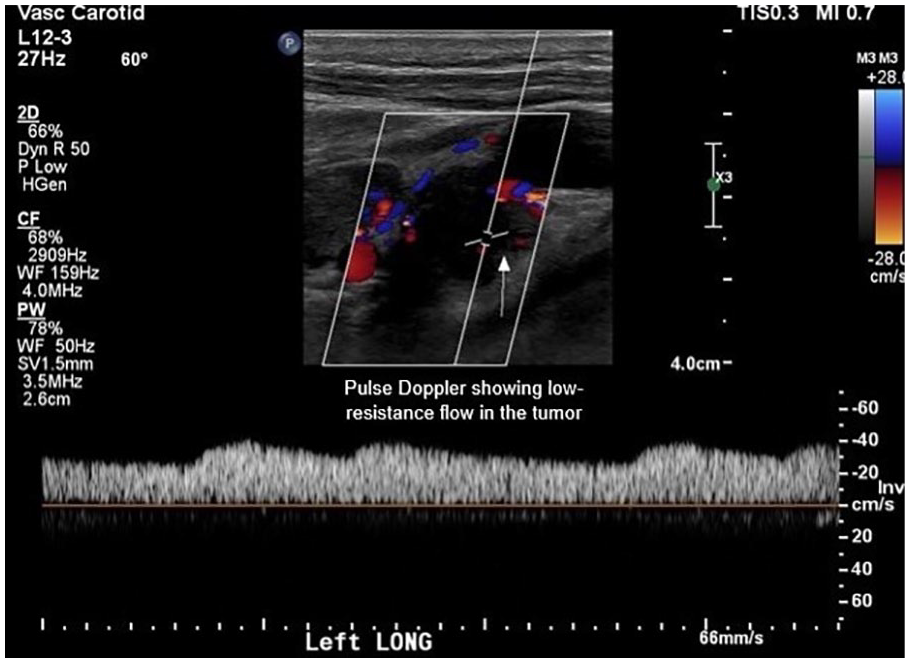
Pulsed wave spectral Doppler analysis showing a low-resistance flow signal within the carotid body tumor.
Color Doppler imaging of this mass was suggestive of a carotid body tumor (CBT), demonstrating the vascularity of the mass (Figure 3).
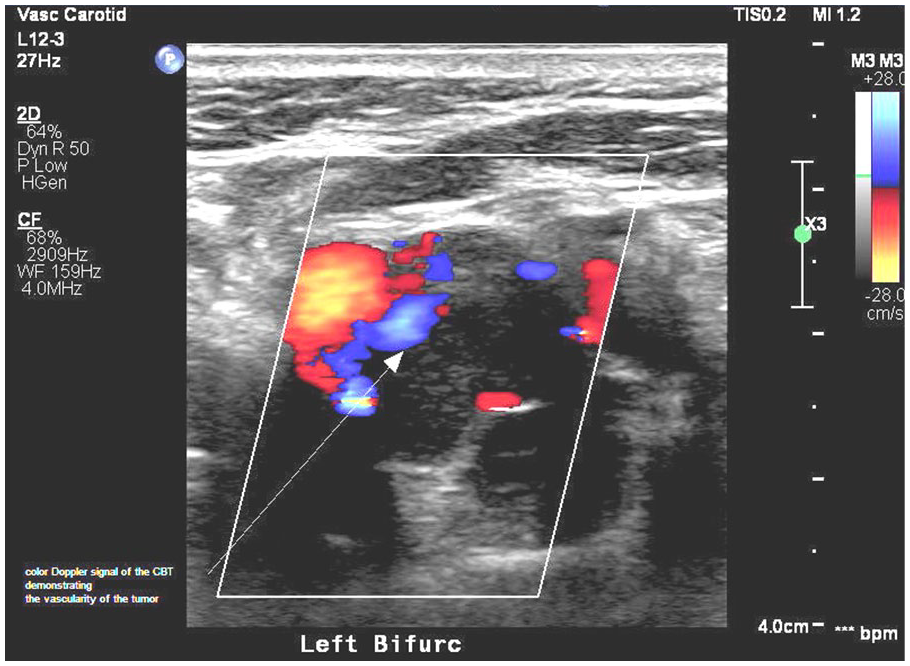
Color Doppler signal of the carotid body tumor demonstrating the vascularity of the tumor.
To differentiate this mass from the other masses in the neck and confirm the vascularity of this possible carotid body tumor, the staff administered 2 cc of diluted Definity contrast agent. Definity (Lantheus Medical Imaging Corporation, Billarica, MA) is currently FDA approved for use in echocardiography to opacify the left ventricle to better detect endocardial borders. Definity has the generic name of Perflutren and is octofluropropane gas that is suspended in a lipid shell. Definity is marketed outside the United States as Luminity and has established use in areas other than echocardiography. The Definity contrast was prepared in the usual fashion, established in echocardiography, with a dilution of 1.6 ml of Definity, 7 ml of saline, and loaded in a 10 cc syringe. Intravenous access (IV) was established with a 22 gauge catheter via a right antecubital approach. It should be noted that the sonographers have privileges to establish intravenous access and inject contrast agents since this practice fell within their institutional scope of practice.
The 2 ml of a diluted bolus was injected while the left carotid bifurcation was monitored using a Philips Epiq 7 ultrasound system, utilizing a L12-3 linear phased array transducer. Because there were no established settings for this particular application, the staff chose to adjust the system settings as indicated for a contrast echocardiogram. The mechanical index (MI) was lowered to 0.07 with the flash MI set at 0.78. The flash control was used intermittently to destroy any previous microbubbles to observe the vascular uptake of the tumor in question in real time. Increased contrast uptake was noted by this mass, which suggests that it is highly vascular 1 and is consistent with a diagnosis of a carotid body tumor in our patient (Figures 4 and 5).
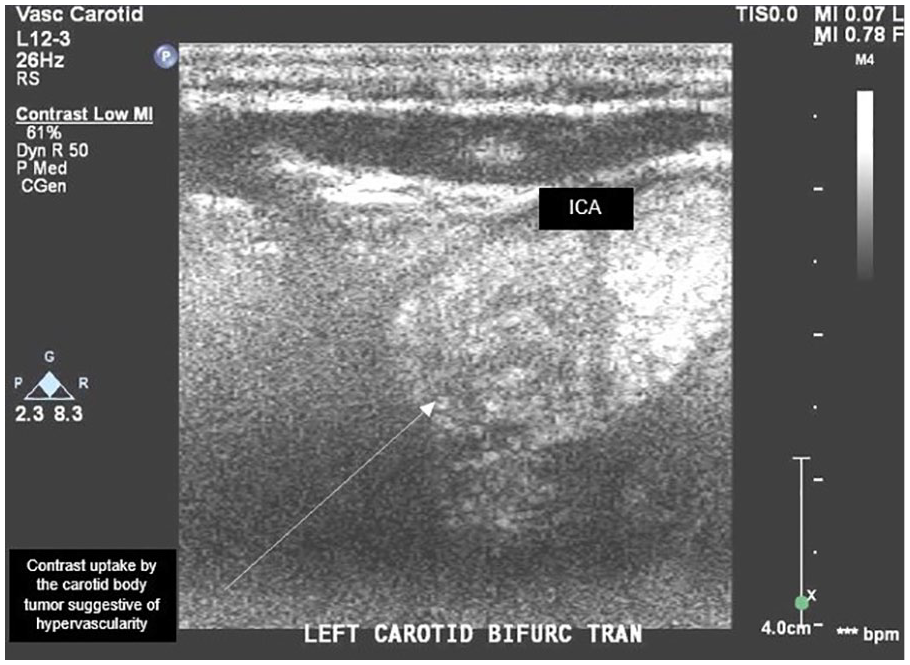
Transverse duplex sonographic view. Contrast enhanced ultrasound demonstrated hyper vascularity of the mass, demonstrated by the contrast uptake.
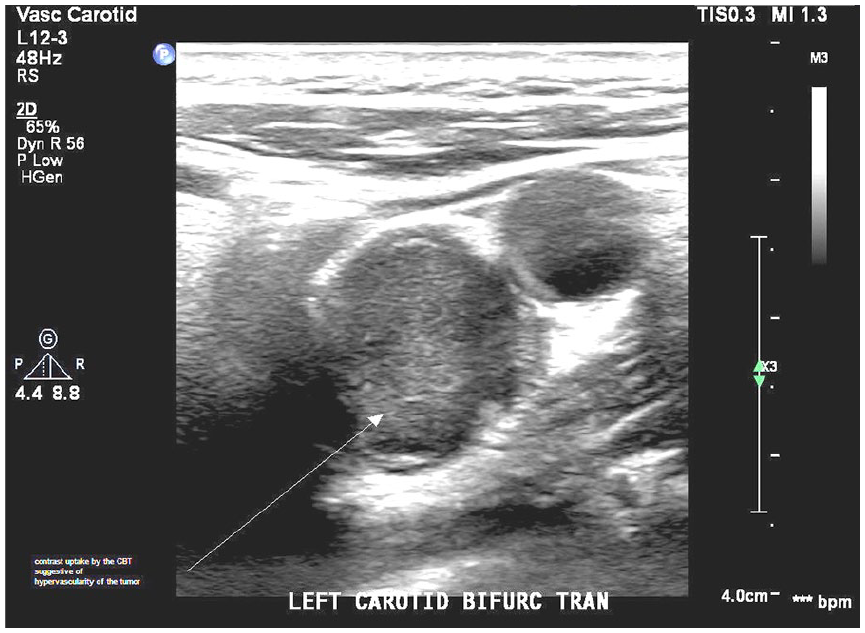
Duplex ultrasound transverse view. Post–contrast administered image of the carotid body tumor.
This patient was referred to a vascular surgeon for further evaluation and management of this carotid body tumor. A computed tomographic angiogram (CTA) of the neck was performed. Axial images were acquired at 1.25 cm intervals from the upper thorax through the skull base utilizing an arteriogram protocol. Coronal and sagittal reconstruction was acquired from the axial images. A unilateral left carotid body enhancing tumor splaying the internal and external carotid arteries was identified (Figures 6 and 7).
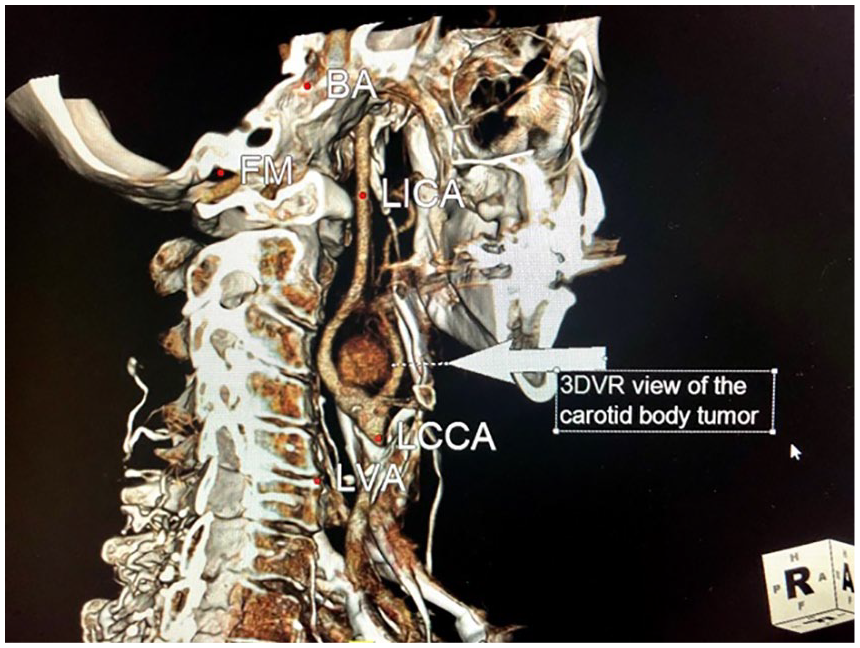
Computed tomographic angiogram neck: 3D volume rendered (3DVR) TeraRecon workstation reformatted image of the left carotid body tumor.

Computed tomographic angiogram neck 2 × 2 maximum intensity projection (MIP) view. TeraRecon workstation reformatted image of the left carotid body tumor, which splays the internal carotid and external carotid arteries.
Carotid body tumors are classified into three groups for surgical treatment planning based on their relative size and relationship with carotid arteries. 2 Surgical excision can usually be carried out without difficulty in Shamblin I tumors as they are small and minimally attached to the carotid arteries. Surgical excision can be carried out with caution in Shamblin II tumors, which are usually larger and show moderate arterial attachment. Surgical excision can be carried out with great care with consideration to vessel replacement for Shamblin III tumors, which are usually large and incarcerate the carotids. The patient underwent Shamblin II 2 left carotid body tumor resection by a vascular surgeon. The mass was resected in total under general anesthesia. The patient remained stable and was discharged home postoperatively with no complications. Because paragangliomas have been shown to be caused by germline mutations in three of the four succinate dehydrogenase genes—SDHB, SDHC, and SDHD, 3 the physicians recommended for this patient to have her first-degree relatives screened.
Discussion
Carotid body tumors, also known as paragangliomas, are tumors arising from the paraganglion system. These are rare neuroendocrine tumors that arise from the extra-adrenal autonomic paraganglia, originating from the embryonic neural crest cells. With normal embryological development, most paraganglia sites disappear after birth except around the sympathetic nervous system and in the adrenal medulla. In the head and neck, the main areas with paraganglia that may form, tumors are located around the jugulo-tympanic area, the carotid body, vagal nerve, and tympanic area, as previously discussed in a retrospective study. 4 Carotid body tumors derived from neural-crest progenitor cells at the level of the common carotid artery bifurcation are the most common paragangliomas, accounting for 60% to 70% of head and neck paragangliomas. These present as slow-growing lateral neck masses. As they enlarge, they may cause symptoms due to local compression of the adjacent structures, causing dysphagia, hoarseness of voice, or symptoms related to crania nerve or sympathetic neuropathies.1,5 Most paragangliomas appear to be benign, but over time about 5% of these tumors may display malignant behavior, mostly spreading to the adjacent and/or metastatic lymph nodes.6,7 Due to the high vascularity and potentially catecholamine secreting nature of these tumors, fine needle aspiration biopsy is relatively contraindicated. 1
Duplex sonography with color and spectral analysis is a safe, portable, and noninvasive method for evaluating this lateral neck mass. As this mass is a slow-growing tumor, it may not be readily identified during a routine physical examination. As in this case, the CBT was detected while performing an outside screening examination of the carotid arteries. A high level of suspicion for a CBT should be considered when evaluating incidental lateral neck masses as this diagnosis may be difficult due to a broad range of differential diagnosis. Causes of localized neck swelling may include but are not limited to enlarged lymph nodes due to lymphadenopathy, thyroid disease, metastatic lesions, thyroglossal duct cysts, brachial cleft cysts, laryngocele, lipomas, and extracranial carotid artery aneurysms.5,8 As carotid body tumors are highly vascular in about 80% of the cases described in the literature, contrast enhancement ultrasound (CEUS) using Definity was used to provide a confirmatory diagnosis of vascularity. This allowed for the staff to appropriately triage and refer the patient to vascular surgery for further medical management. This case report demonstrates the utilization of CEUS as an emerging method in the noninvasive vascular imaging. Magnetic resonance imaging (MRI), CTA, and contrast angiography have all been previously described in literature as identifying tumor relationship to the adjacent structures, identifying if unilateral or bilateral, and investigating metastatic infiltration to regional lymph nodes.9–11 However, all of these imaging modalities are not available for use at the bedside to confirm the diagnosis. Utilizing portable diagnostic sonography with CEUS may avoid unnecessary invasive procedures such as fine needle aspiration, biopsy, or further expensive testing.
The use of ultrasound contrast agents has historically been limited to echocardiography in the United States. In 2016, one agent (Lumason) was FDA approved for use in general sonography to opacify structures in the liver and urinary tract. There are currently no FDA-approved agents for use in vascular sonography. It should be noted that the use of these ultrasound contrast agents outside of the United States is more widely accepted and is a common practice in Europe, Asia, and Canada.
A previous case report 2 mentioned utilizing CEUS to achieve higher diagnostic accuracy in the identification of carotid body tumors. However, this case was published approximately ten years ago. Now that the use of CEUS is becoming more widely accepted outside the cardiology realm, our case serves to not only increase awareness but also reiterate the value of this noninvasive technique to increase diagnostic accuracy in a cost-effective manner as well as eliminating ionizing radiation. In this case report, the neck mass was detected at bedside as a possible carotid body tumor. The staff decided to administer Definity to demonstrate the level of vascularity that narrowed the differential diagnosis to be a CBT and were able to appropriately triage the patient to the vascular surgeon. A CTA of the neck was then performed to demonstrate the tumor’s anatomical relationship to the adjacent neck structures. In our case, it was a unilateral left carotid body enhancing tumor splaying the internal and external carotid arteries. A single, seemingly reactive lymph node was identified lateral to the distal internal carotid artery. No other enlarged lymph nodes were identified during the surgery, which indicates that this could be a benign tumor.
Conclusion
Carotid duplex imaging is a valuable, noninvasive, inexpensive bedside imaging modality that is extremely useful for diagnosing a carotid body tumor when evaluating a lateral neck mass. Since most carotid body tumors are vascular, color Doppler evaluation to demonstrate tumor vascularity was previously used. In this case, the staff went further and performed CEUS to demonstrate vascularity of the tumor, which subsequently helped confirm the tumor as a carotid vascular tumor through a noninvasive modality. Identifying the vascularity and location of the mass helped with rapidly identifying and differentiating the carotid body tumor from other causes of a localized neck swelling, such as lymph nodes, thyroid disease, metastatic lesions, and so on. CEUS is emerging as a new technique to further enhance diagnostic capability in the noninvasive imaging sector. This technique may offer promise in increasing the sensitivity of conventional carotid duplex imaging and help in appropriately triaging the patient to the respective fields for further management, especially in the setting of limited access to more specialized and expensive imaging modalities such as CTA, MRI, and contrast angiography.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.