
Abstract
A carotid body tumor is typically a benign mass and can have a low malignant potential. It can grow in between, attach to, or surround the internal carotid artery and external carotid artery in the neck. If this mass grows too big, it can compress the two arteries, causing problems in getting blood flow to the brain. The purpose for this sonography examination was to evaluate a patient with the following symptoms: dizziness, facial nerve injury, and sensorineural hearing loss. The carotid body tumor is a highly vascular tumor. This sonography examination provides a good opportunity to teach the importance of the use of color Doppler and proper documentation of this pathology that is often incorrectly documented with improper settings. This case reviews a 69-year-old Caucasian male with a carotid body tumor. The sonographic features, prevalence, common symptoms, prognosis, and treatments of the carotid body tumor are reviewed.
Normal bilateral carotid bodies exist in every human body, although they have the potential of becoming a carotid body tumor. A carotid body is typically described as a 1- to 1.5-mm structure located in the adventitia of the carotid bifurcation that has a role in the control of blood pressure, arterial pH, and blood gasses. 1 The carotid body is a chemoreceptor that modulates cardiovascular and respiratory function primarily through sympathetic tone. 2 The innervation of the carotid body is Hering’s nerve, also known as carotid sinus nerve, a branch of the glossopharyngeal (Cranial Nerve IX), originating 1.5 cm distal to jugular foramen. Two types of receptor cells the carotid body is composed of are chief cells (Type I), which are derived from neural crest and release acetylcholine (Ach), adenosine triphosphate (ATP), and dopamine in response to activation, and sustentacular cells (Type II), which are supporting cells. 2 It is noted that the carotid body tumors can vary in size. Carotid body tumors are classified as paragangliomas and usually are not malignant. 1 Even though carotid body tumors are mostly benign, treatment for removal is important to minimize the risk of any further complications. The tumor can grow quickly and press against nearby vessels and nerves, causing damage to other structures. It is important to adequately document this tumor so that it does not go unnoticed and the patient can receive the proper care.
Case Report
A 69-year-old Caucasian male presented with a history of right-sided paraganglioma with bone involvement. The patient had a magnetic resonance imaging (MRI) of the brain in 2009, which led to the finding of the right-sided paraganglioma. Also, the patient had a computed tomography (CT) of the temporal bones in 2009, which led to the finding of bone involvement. Due to the patient’s symptoms, which included dizziness, facial nerve injury, and sensorineural hearing loss, a carotid sonogram was ordered and performed in January 2012. There were no sonographic examinations prior to this date and no labs recorded at the time.
The sonography examination demonstrated a 1.4 × 1.9 × 3.5 cm hypoechoic mass at the left carotid artery bifurcation (see Figures 1, 2). This mass splayed the internal carotid artery and external carotid artery (see Figure 3). The mass also demonstrated high vascularity with the use of color Doppler (see Figure 4). There was normal color flow and spectral waveforms that demonstrated no hemodynamically significant stenosis within the left carotid arterial system (see Figure 5).
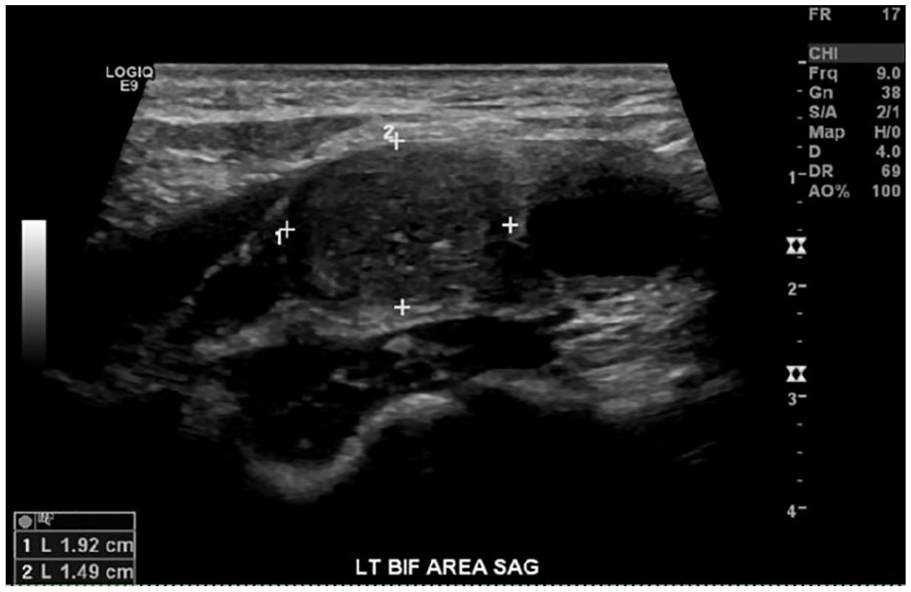
Sagittal gray-scale image of the hypoechoic mass in between the left carotid bifurcation with measurements.
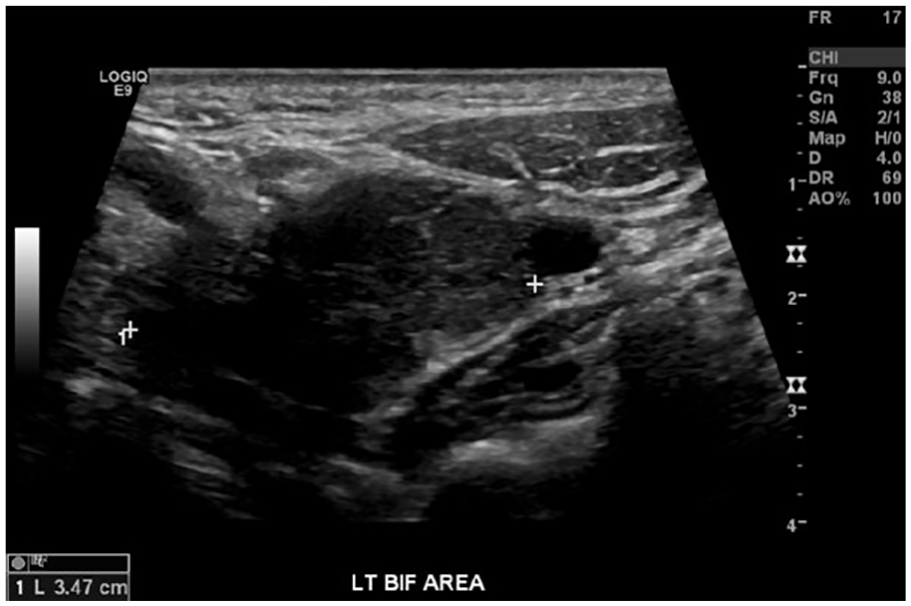
Transverse gray-scale image of the hypoechoic mass in between the left carotid bifurcation with measurements.
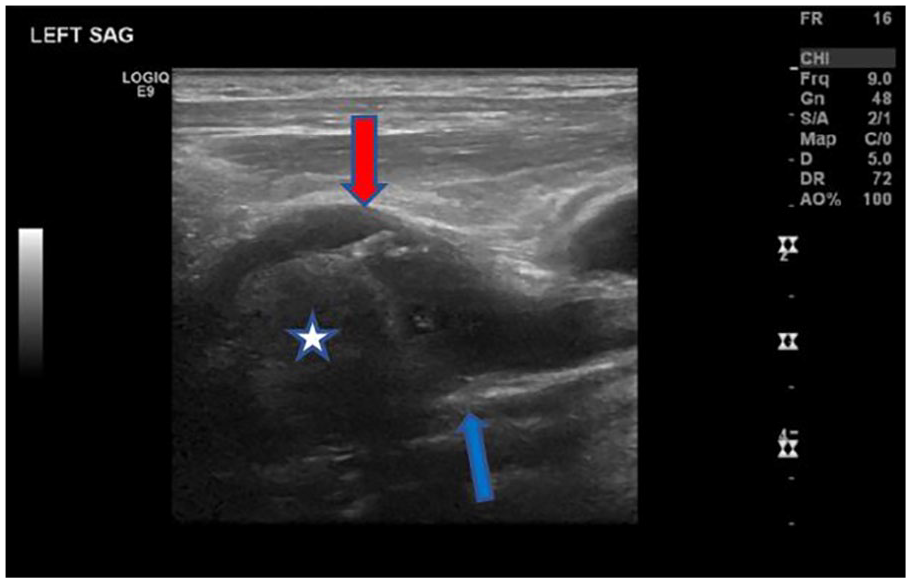
Sagittal gray-scale image demonstrating the carotid body tumor splaying the left internal carotid artery (ICA) and the left external carotid artery (ECA). The red arrow is pointing to the left ECA. The blue arrow is pointing to the left ICA. The white star is identifying the carotid body tumor.
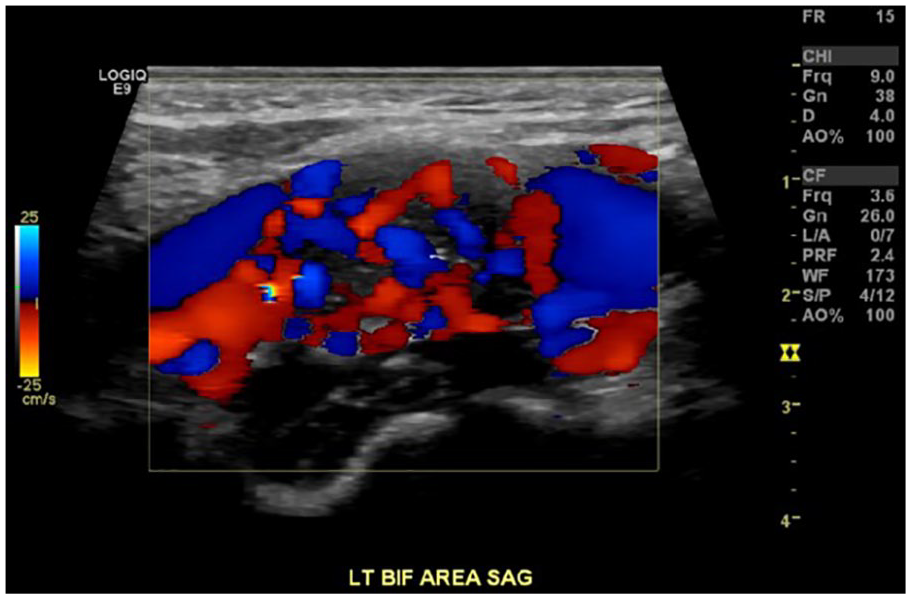
Sagittal image with color Doppler demonstrating the high vascularity of the carotid body tumor.
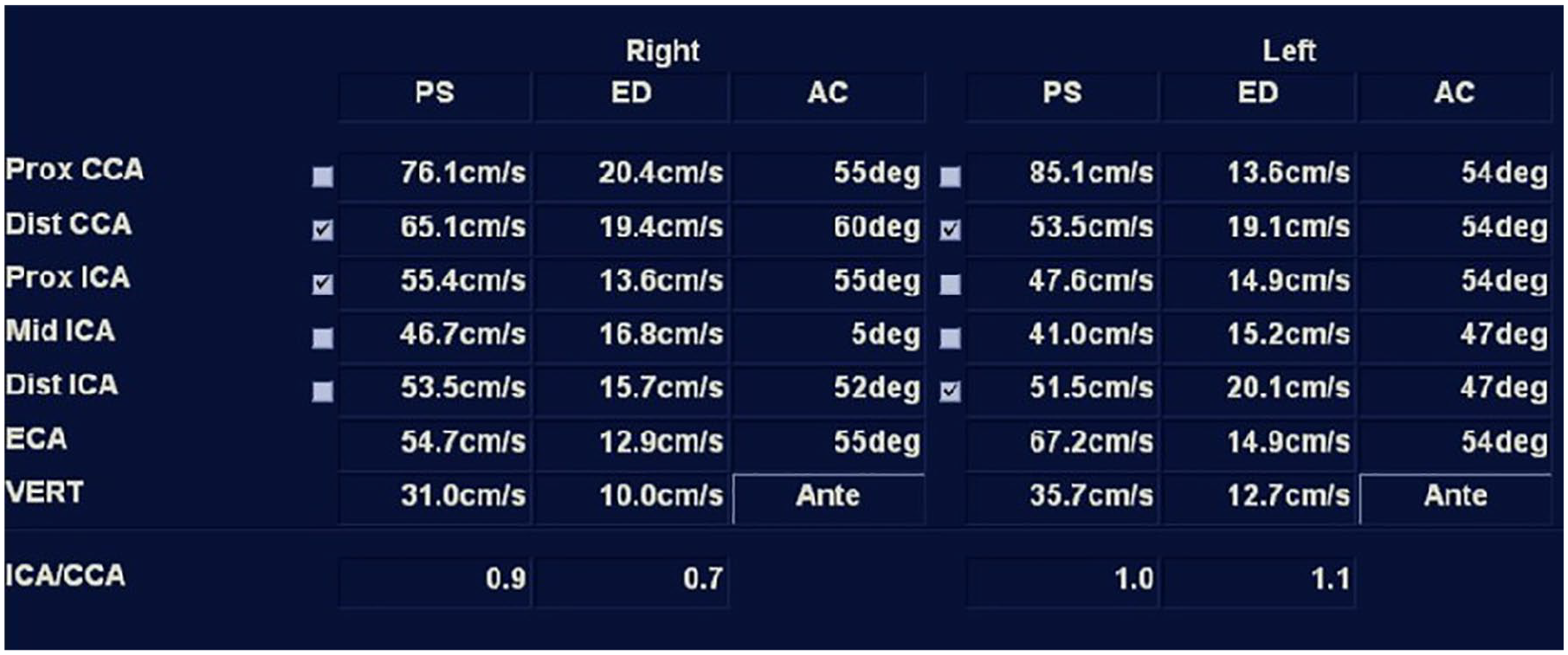
The vessel summary report page of all the velocities in the carotid sonography study. This demonstrates the patient had no significant stenosis visualized.
The patient had surgery for removal of the carotid body tumor done at a different facility, thus there was no documentation noted. Although, he did have a follow-up sonography examination performed in July 2018, which demonstrated plaque within the carotid arteries bilaterally and no significant stenosis. Velocities were obtained of both the left internal carotid artery (ICA) and common carotid artery (CCA). His ICA/CCA ratio on the left was 0.57 and on the right was 0.8, which is considered within normal limits. Although this case presented unilaterally, it is important to document the contralateral side because carotid body tumors can occur bilaterally.
Discussion
Carotid body tumors can develop in any patient. There is no specific element that contributes to a risk for development. The incidence of a carotid body tumor is less than 1 in 30 000. Recent studies have reported that carotid body tumors are more common in females rather than males. There is a wide variety of ages in which the carotid body tumor can appear. Lesions occurring before the age of 20 are rare. 3 The typical age of occurrence ranges between 35.9 and 71.7 years old, and a majority of the patients were female (60.4%). 4 This coincides with the age of the 69-year-old patient at the time of his diagnosis.
A carotid body tumor is usually asymptomatic, but it can cause external pressure on the ICA. This would lead to symptoms of neck pain, dizziness, palpable mass, hoarseness, dysphasia, syncope, and headaches. 1 Most of these symptoms are similar to the patient’s symptoms of dizziness, facial nerve injury, and sensorineural hearing loss. Recent studies have shown that carotid body tumors are the cause of high blood pressure. 5 Resection of the tumor has successfully lowered blood pressure. 5 These factors can be taken into consideration when diagnosing a carotid body tumor.
A succinate dehydrogenase (SDH) mutation is the most common predisposition gene that can present in some cases of carotid body tumor. 6 There are familial and sporadic causes for this tumor. In the cases of familial history, genetic testing is recommended for early detection. In both familial and sporadic cases, the tumor usually includes a genetic predisposition with a link to higher elevations, 2000 meters above sea level in most cases. 6 Interestingly, at sea level, the male to female ratio is closer to one to one, whereas at a higher altitude, the ratio changes to about one to eight. There is currently not an explanation for this ratio change. However, hypoxia seems to enhance the SDH mutation. 6
Sonography paired with contrast CT and MRI is optimal when diagnosing a carotid body tumor. Together, they can pinpoint the location and vascularity of the tumor. They also help when determining the difference of carotid body tumors from other types of tumors. These images together provide information on the spread of the tumor. Another example is that the “salt and pepper” image appearance in contrast MRI that can help in distinguishing a carotid body tumor from other tumors. CT images provide better visualization for those tumors that may be located in the base of the skull. The gold standard used to study the highly vascular flow of the carotid body tumor is digital subtraction angiography. The angiography is usually performed 24 to 48 hours before surgery to enable embolization of the feeding vessels. 6 It is also interesting to note that the use of a positron emission tomography (PET) has been extremely successful when dealing with carotid body tumors because it detects large numbers of somatostatin receptors. PET images are also useful in detecting metastatic disease. 6
Even though carotid body tumors are most frequently seen in the carotid body, they are known to arise from parasympathetic nerves and may develop at any site from the skull base to the arch of the aorta. 7 One of the common sonographic features is a well-defined mass in between the external carotid artery (ECA) and ICA. It is a highly vascular tumor that is fed by the ECA branches through the Mayer’s ligament that provides attachment to carotids; however, other vessels like vertebral arteries may contribute to the vascular flow, particularly to large tumors. 2 Spectral Doppler will typically demonstrate low-resistance waveforms within the tumor due to the need for a plentiful blood supply. It is important for sonographers to demonstrate blood flow within the tumor to help in the diagnosis. To detect blood flow, sonographers may need to decrease the color scale to identify small vessels feeding the tumor. 1 It is important to know the proper methods for documenting a carotid body tumor so the patient can be accurately diagnosed. In this case, the sonographer failed to use the pulsed-wave Doppler to demonstrate the type of flow that was in the tumor. However, the sonographer did properly use color Doppler to document flow within the hypoechoic mass. In this case, the accurate use of color Doppler was sufficient to diagnosis a carotid body tumor; however, it is better to gather the maximum amount of information to further a patient’s diagnosis.
When using color Doppler, it is important for sonographers to optimize the color PRF and gain settings to avoid “color bleed” and to ensure that the relationship of the mass to the bifurcations vessels is not masked by the color display. A sonographer will have to lower the PRF to be able to demonstrate the highly vascular blood flow in the tumor. Gray-scale, color, and/or power Doppler images should routinely be included in the examination to show the spatial relationship of the tumor to the bifurcation vessels.
Some complications may occur that may warrant further investigation. There are many types of differential diagnoses that are similar to carotid body tumors. One differential diagnosis is an abnormal/malignant cervical lymph nodes that is located along the lymphatic channels of the neck and has been classified for staging of cancers. These are common sites of pathologic involvement with metastasis, lymphoma, lymphadenitis, and reactive adenitis. 8 Normal nodes are oval or bean-shaped or hypoechoic with echogenic hilum, and vascularity should be present within the hilum. Abnormal/malignant lymph nodes have a wide variety of appearances but typically can have the sonographic features of hypoechoic or hyperechoic or round or lobulated, lose their fatty hilum, or be peripheral or mixed vascularity and high resistive. 8 These lymph nodes are common in head and neck cancers. Symptoms may be tenderness, pain, swelling, fever, and weight loss. 8
The combination of sonography with guided fine needle aspiration cytology increases the sonographic diagnostic specificity. 8 CT, contrast-enhanced CT, MRI, and PET/CT are other imaging modalities that can be used to help diagnosis a malignant cervical lymph node. Although, when assessing for malignant cervical nodes, sonography has the highest sensitivity, whereas PET/CT has the highest specificity in the diagnosis. 8 Even though carotid body tumors and abnormal/malignant lymph nodes can appear very similar, they are vastly different structures. Also, the vascular beds of an abnormal cervical lymph node are highly resistive compared to a carotid body tumor, which has a low vascular resistance. It is important for sonographers to use gray-scale, color, power, and spectral Doppler to aid in this differential diagnosis.
Carotid body tumors are known as benign tumors. Therefore, the malignancy rate is reported to be 10% to 20% of all cases. 9 If the tumor is malignant, there is a less than 5% chance it will spread to other areas of the body. 10 Whether the tumor is benign or malignant, the growth of the tumor can affect the patient by obstructing other structures in the body or by causing symptoms that disrupt a patient’s way of life. That is a reason why treatment options for this pathology are important to explore. Treatment methods of paragangliomas include surgical resection, external beam radiotherapy, and stereotactic radiation therapy. 3 Although there is a wide variety of treatments a patient can undergo, there is still one treatment option that is highly recommended. The treatment of choice is a complete surgical excision of carotid body tumor because the tumor has a 5% or greater incidence of metastases; radiation therapy and chemotherapy are options but are unsatisfactory. 11 Because the treatment of choice is a complete surgical excision, the sonographer must include accurate measurements of the length and width of the tumor and demonstrate its relationship to the ICA, ECA, and CCA using gray-scale imaging and multiple planes of the view. There can be fear for reoccurrence; however, it is highly unlikely to happen. There is a 5% to 10% chance of reoccurrence of another carotid body tumor after surgery. 10
Patients also need to be mindful that with every surgery there are possibilities of injury. Early attempts at surgical excision of carotid body tumors began in 1880 but were treacherous, resulting in high rates of nerve damage, stroke, hemorrhage, and death. 4 Surgical removal of a small, asymptomatic carotid body tumor is recommended because it has a much lower risk of cranial nerve and carotid artery injuries than excision of a large tumor. 11 Another possible complication is a stroke, but this is rare and happens in less than 2% of carotid body tumor removals. 10 Through experience and further study, it seems that tumor embolization can aid in total tumor removal while lowering the risks of intraoperative bleeding and cranial nerve paralysis. 6 Because it is important to keep the risk factors of surgery in mind, the outcome of removing the tumor can outweigh the risks. A patient’s quality of life and care is the most important factor.
Conclusion
Although the majority of carotid body tumors are considered benign, they have the potential to affect the patient’s daily living. It is important for a sonographer to be able to recognize a carotid body tumor and use the proper machine settings to help in diagnosing the tumor. Given that this tumor is highly vascular, there will be a need to lower the pulse repetition frequency to detect blood flow feeding the tumor. Thus, having the proper knowledge of ultrasound physics and characteristics of a carotid body tumor aids in obtaining high-quality imaging as well as achieving an accurate diagnosis.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.