
Abstract
A case of thrombophlebitis of a retroperitoneal varix in a postpartum patient with right lower quadrant pain is presented. The sonographic examination was falsely positive for appendicitis, but the correct diagnosis was made with a subsequent computed tomogram. The thrombosed varix was likely a collateral of the right ovarian vein, analogous to postpartum ovarian vein thrombophlebitis (POVT), an uncommon potentially fatal disorder. POVT is reviewed, emphasizing features useful for distinguishing it from appendicitis at sonography. Sonographers should be aware of the possibility of thrombophlebitis when examining postpartum patients with right lower quadrant pain.
Postpartum ovarian vein thrombophlebitis (POVT) is an uncommon disorder that occurs following delivery. It has an incidence of 0.05% to 0.18% 1 and is higher after cesarean than vaginal births. 2 Nonpuerperal ovarian vein thrombophlebitis (OVT) may occur during pregnancy or in cases of Crohn disease, ovarian torsion, pelvic inflammatory disease, cancer, pelvic surgery, uterine leiomyomata, molar pregnancy, or hypercoagulation disorders.3–5 Morbidity and fatalities from OVT and POVT are caused by pulmonary embolism, septicemia, and septic embolism.
POVT occurs most often on the right side of the pelvis. 3 It presents similarly to appendicitis, typically with right lower quadrant pain, fever, and elevated white blood cell count, and is often initially misdiagnosed as appendicitis.6,7
Ovarian vein collaterals and varices form in response to stenosis, thrombosis, or extrinsic compression of the main ovarian vein. They may result from extrinsic compression from the gravid uterus that occurs during pregnancy or from congenital vascular anomalies that obstruct venous flow. 8 They may also be caused by incompetent valves, either congenital or acquired. High estrogen levels during pregnancy may weaken venous walls, diminishing the pressure needed to dilate the veins and thereby facilitating the formation of varices. 9
A case is presented in which a postpartum patient with right lower quadrant pain was initially examined by sonography, with results that suggested an appendicitis. Due to her puerperal state, the radiologist recommended a computed tomogram (CT) for confirmation. The CT revealed a normal appendix and a thrombosed right retroperitoneal varix.
Case Report
An 18-year-old G1 T1 P1 A0 L1 woman presented to the emergency department (ED) four days after delivery with right lower quadrant pain that had begun two days prior. She rated her pain as 8 on a 0 to 10 scale. Her vital signs were normal, including temperature 36°C, pulse 69 beats per minute, and blood pressure 126/71 mm Hg. She had right lower quadrant tenderness. The white blood cell count was normal at 7800 cells/mm3. The ED physician ordered a pelvic sonogram to evaluate the right ovary and to assess for retained products of conception, as well as a right lower quadrant sonogram to exclude appendicitis.
Sonography of the pelvis revealed no evidence for retained products of conception. The right ovary and right kidney appeared normal. Examination of the right lower quadrant using a 12-MHz linear-array transducer revealed a hypoechoic, laminated tubular structure in the right lower quadrant at the site of pain. It appeared to be blind-ending (Figure 1). It was noncompressible (Figure 2), had a maximum diameter of 15 mm (Figure 3), and was in the expected position of the appendix. The surrounding fat was echogenic. There was no flow with color Doppler, but some flow was detected in the surrounding tissues (Figure 4).
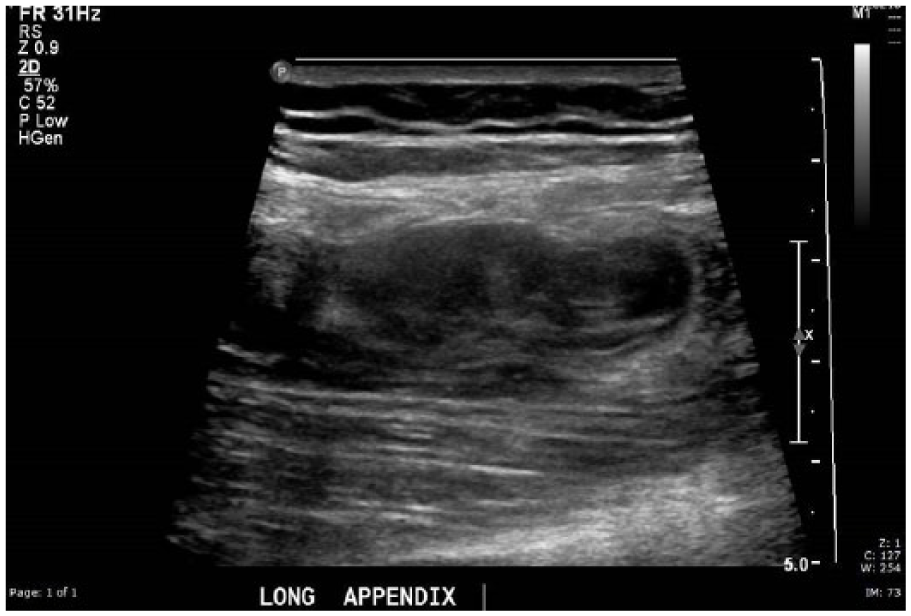
Hypoechoic, laminated, apparently blind-ended tubular structure in the area of pain in the patient’s right lower quadrant.
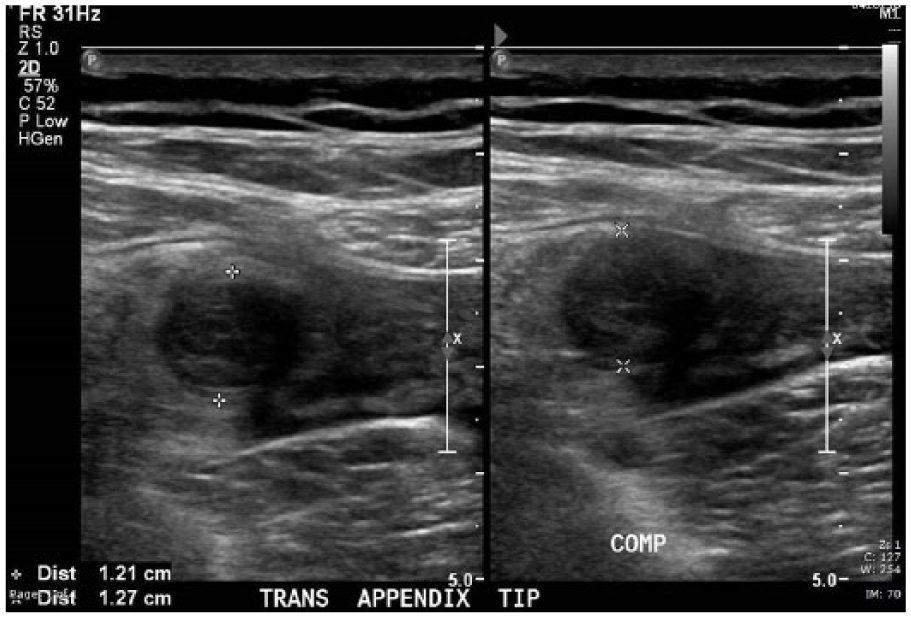
Hypoechoic tubular structure found in the area of pain was noncompressible. The patient experienced increased pain with the attempt to compress.
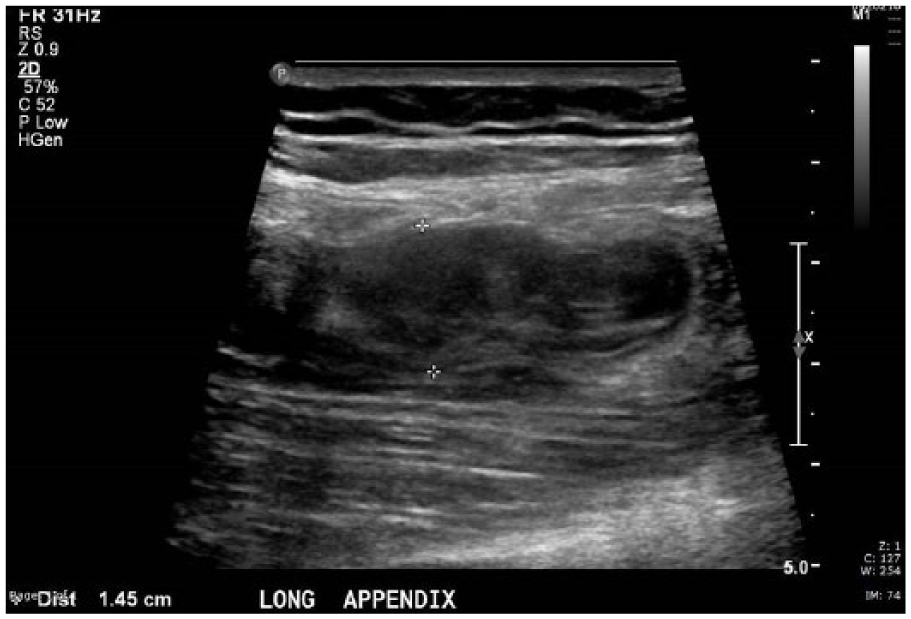
Tubular structure in the patient’s area of pain, in the expected position of the appendix, measured 15 mm.
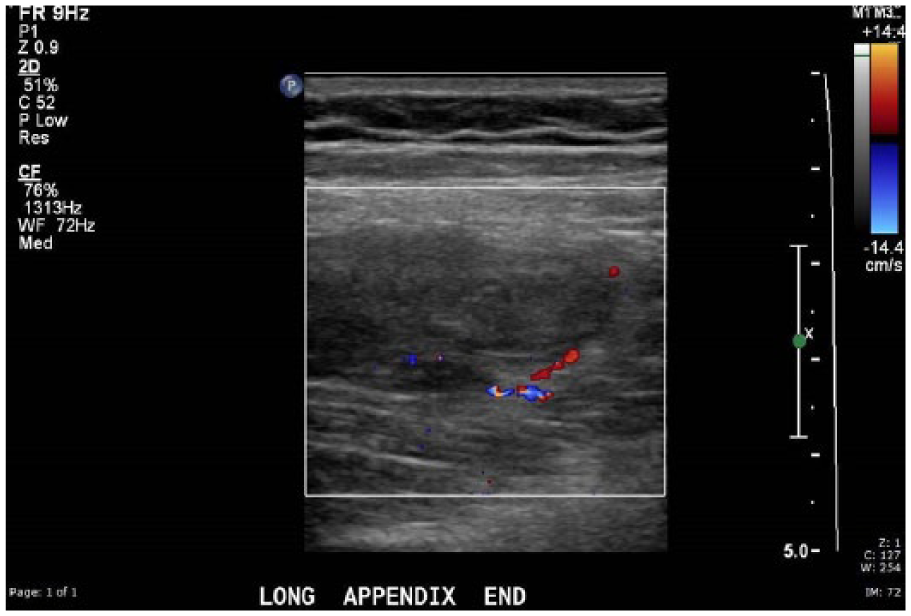
No color Doppler flow was seen within the tubular structure in the area of pain. Color Doppler flow was seen on the periphery of the structure.
Although the sonogram was suspicious for appendicitis, the radiologist recommended a CT for further evaluation. Instead of confirming the presence of appendicitis, the CT revealed a normal appendix (Figure 5) and a tortuous, acutely thrombosed retroperitoneal varix, likely a collateral of the right ovarian vein (Figure 6). The main right ovarian vein was equivocal for thrombus by density (Figure 7), but thrombosis is unlikely based on its normal size and difference in appearance from the thrombosed adjacent varix.

Computed tomogram of the lower abdomen and pelvis revealed a normal appendix.
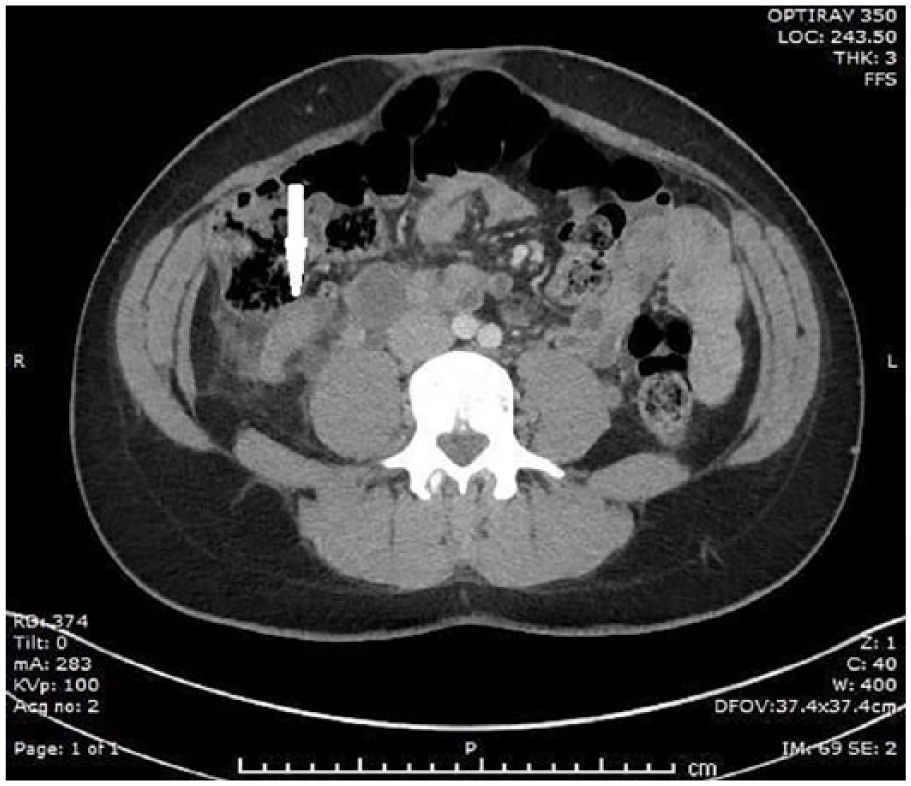
Computed tomogram showed an acutely thrombosed, tortuous varix near the appendix, likely a collateral of the right ovarian vein.
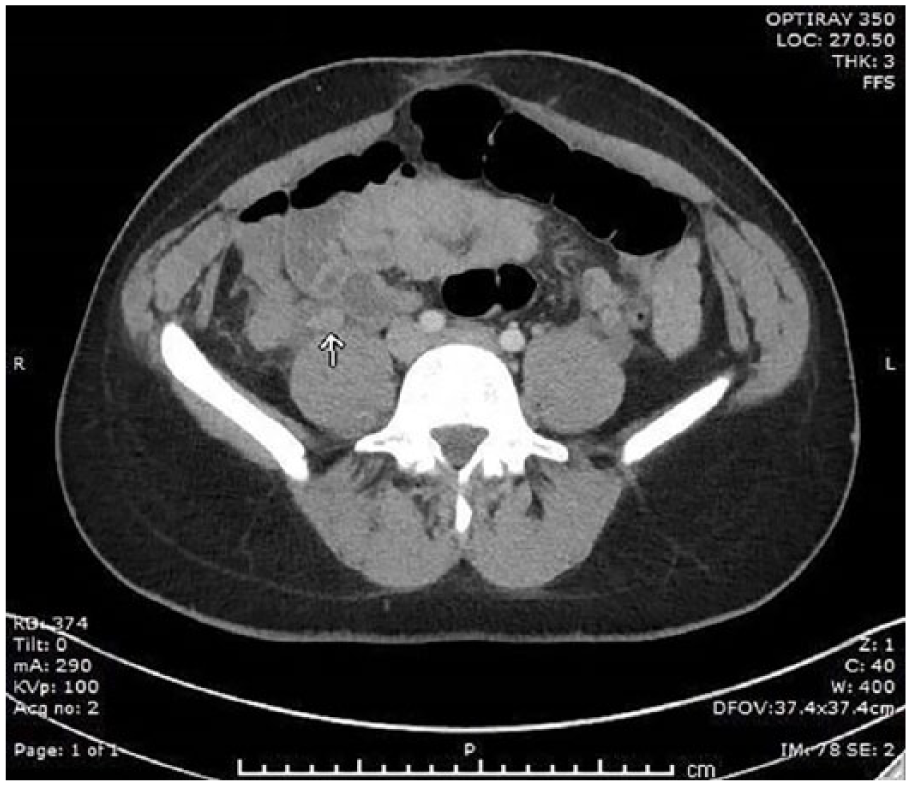
The main right ovarian vein was equivocal for thrombus.
The patient was hospitalized for four days and treated with antibiotics and subcutaneous heparin injections. After discharge, anticoagulation therapy with Lovenox was prescribed for six weeks. She received no additional treatment. Notes from her gynecologist eight weeks later mention no further symptoms or adverse sequelae of POVT, suggesting a complete recovery.
Discussion
This case is an unusual variant of POVT in which a varix adjacent to the main ovarian vein rather than the ovarian vein itself was thrombosed. This retroperitoneal varix might have formed during late pregnancy as a collateral to a compressed right ovarian vein. It could then have collapsed after birth when decreasing size of the uterus allowed normal flow to resume in the main right ovarian vein, slowing flow through the varix and precipitating thrombus formation. Although findings on her sonogram were suspicious for appendicitis, the correct diagnosis was made at CT. Surgery was avoided, and she recovered uneventfully after treatment with anticoagulants and antibiotics.
The pathogenesis, clinical considerations, imaging, and treatment of POVT are presented below. These factors also apply to the thrombosed retroperitoneal varix in this patient.
Pathogenesis
Numerous small veins feed from the ovaries into venous plexuses in the broad ligaments of the uterus. These veins converge to form the right and left ovarian veins that extend cranially, anterior to the psoas muscles. The left ovarian vein empties into the left renal vein. The right ovarian vein joins the inferior vena cava (IVC). During pregnancy, the ovarian veins increase in diameter 3-fold, increasing their capacity 60-fold. 10
Three factors contribute to thrombus formation in any vein. They are known as Virchow’s triad 11 : venous stasis, intimal injury, and hypercoagulability. All three factors may be present postpartum.
Venous Stasis
The ovarian veins, their volume increased during pregnancy, have been observed to collapse immediately after delivery. Subsequent flow in the veins is greatly decreased.10,12 The valves in these long, unbranched veins may become incompetent, exacerbating stasis. Valve leaflets can create areas of stagnant blood on the downstream side, serving as a nidus for clot formation. 13
The right-sided prevalence of POVT is attributed to the dextrorotation of the uterus during pregnancy and in the initial postpartum period. The sigmoid colon on the left side of the pelvis causes the uterus to rotate rightward as it expands. This may compress the right ovarian vein, causing venous stasis and possible mechanical injury to the vein. 13 In addition, several clinical studies suggest that postpartum retrograde flow in the left ovarian vein protects it against ascending infection,14,15 a mitigating factor not present on the right.
Intimal Injury
Endometritis is often associated with postpartum ovarian vein thrombosis.1,6 Since the ovarian veins have extensive communication with the uterine and vaginal venous plexuses, infection can extend fairly easily from the endometrium into the ovarian veins, injuring the intima of the veins. Various organisms, including Escherichia coli and various species of Streptococcus, Bacteroides, Proteus, Staphylococcus, and Klebsiella, have been cultured from veins or from thrombus taken from veins of patients with POVT. 1 Organisms causing endometritis may be present antepartum or may be introduced by cesarean section, instrumentation such as forceps, or manual manipulation of the fetus during vaginal delivery. 16
Alternatively, there may be mechanical injury to the intima during pregnancy or childbirth. This could be caused by the gravid uterus compressing the ovarian vein as it crosses the bony pelvic brim. The ovarian veins, unlike the veins of the extremities, lack a restrictive fibrous sheath. This allows them to expand during pregnancy but may render them more vulnerable to injury by compression from the uterus. 13
Hypercoagulability
Clotting factors I, II, VII, IX, and X are elevated during pregnancy and for up to six weeks postpartum. Adhesiveness of platelets may also be increased. 13 The resulting hypercoagulative state helps to limit blood loss at delivery but also creates the conditions for POVT.
Clinical Considerations
The most common clinical findings in patients with POVT are right lower quadrant pain, fever, and increased white blood cell count, making this condition almost indistinguishable from appendicitis.1,3 Two retrospective studies,6,14 prior to the widespread adoption of diagnostic sonography and CT, showed that one-third of POVT cases were initially diagnosed as appendicitis. Less common misdiagnoses are ovarian torsion, nephrolithiasis, pyelonephritis, salpingitis, tubo-ovarian abscess, and broad ligament hematoma.1,6,7 Other potential clinical findings in POVT are tachycardia, flank pain, vomiting, and ileus.1,7 If a pulmonary embolism has occurred, dyspnea, tachypnea, and hypoxia can also be present. POVT symptoms most commonly begin 2 to 3 days postpartum.1,14 Some patients have a palpable tender mass in the right lower quadrant, tubular in shape and extending cranially as well as laterally. This ropelike or sausage-shaped tender mass is nearly pathognomonic for POVT.1,6 The vein and surrounding phlegmon can become quite large. Dunnihoo et al. 1 describe a case in which the vein and associated phlegmon measured 18 by 10 cm at CT.
POVT can affect adjacent retroperitoneal structures. It can cause concurrent renal pathology in two ways. The right ovarian vein crosses over the right ureter at the bony pelvic brim, and a large thrombosed vein can compress the ureter against the brim causing hydronephrosis. In addition, infection and inflammation can spread contiguously from the ovarian vein to the ureter, causing ureteral and periureteral inflammation.17,18 Untreated ovarian vein thrombus can spread to the IVC and via the IVC to the renal, iliac, femoral, and popliteal veins.
Fatalities attributable to POVT are usually due to sepsis, pulmonary emboli, or septic emboli. 19
Imaging and Treatment
Imaging identification and treatment of POVT have greatly improved, and morbidity and mortality have greatly decreased over the past century. 20 Before modern cross-sectional imaging techniques were available, POVT was diagnosed through clinical observation and often through surgical exploration. Late diagnosis and surgical complications contributed to a high mortality rate during this time. 21
Prior to the mid-1960s, treatment of POVT was often surgical. Ligation and sometimes excision of one or both ovarian veins were performed, and if the thrombus had spread to the IVC, it was ligated as well. Complications from surgical treatment were common and included lower extremity edema, ulcers, pulmonary embolisms provoked by the surgery, and death.21,22
Shaffer et al. 23 reported the first CT diagnosis of OVT in 1981. The condition was first diagnosed by sonography in 1983 24 and by magnetic resonance imaging (MRI) in 1986. 25 Current sensitivities of sonography, CT, and MRI are 50% to 56%, 78% to 100%, and 92% to 100%, respectively. Specificities are 41%, 63% to 99%, and 100%, respectively.26,27 MRI can sometimes determine the chronicity of the thrombus. 25 The relatively wide ranges in CT sensitivity and specificity for POVT may be attributed to different statistical techniques used 28 and possibly to CT contrast injection timing. Standard timing of CT contrast injections best opacifies the portal vein and solid organs, while a longer injection time is required to routinely opacify the retroperitoneal ovarian veins. 29
Once antibiotics and anticoagulants became available in the 1940s and late 1960s, respectively, they largely replaced surgery as the preferred treatment for POVT. Currently, a typical treatment regimen for OVT consists of anticoagulation with intravenous heparin, concurrent with a broad-spectrum antibiotic if there is evidence of infection. If specific organisms can be cultured from vaginal, cervical, or blood samples, more targeted antibiotic therapy can be given. The patient is often discharged on self-administered heparin injections or oral coumadin for a few weeks to several months depending on the extent of the thrombus and other risk factors.30,31 In some patients, an IVC filter is placed in the vena cava. 32 Surgery is now reserved for patients who are refractory to heparin therapy or for whom heparin therapy is contraindicated, for patients unable or unlikely to follow up with postdischarge treatment, or for patients who have already incurred a pulmonary embolism.17,32 Earlier diagnosis through modern imaging modalities and nonsurgical treatment have contributed to a precipitous drop in morbidity and mortality of POVT. 20
Practical Imaging Considerations for Sonographers
Sonography is usually the first-line imaging modality used in patients with postpartum complications. Sonographers should consider the possibility of thrombophlebitis as well as appendicitis in patients with postpartum low abdominal pain because both conditions are closely similar clinically. They should also be aware that POVT mimics appendicitis by sonography and take care to differentiate them. Prior case studies have shown that the sonographic appearance of POVT and appendicitis can be similar, especially if the ovarian vein is displaced laterally, which is common in the early postpartum period or if it is tortuous.17,33 The present case shows that a thrombosed tortuous varix is potentially more similar to an abnormal appendix than is a thrombosed ovarian vein. This is because the serpiginous course of the varix can create the false impression of a blind end, one of the sonographic hallmarks of the appendix, if the vein is imaged along its axis and turns abruptly out of the field of view. Doppler was not helpful since in both cases, the tubular structure contains no central flow, and there may be increased flow in the surrounding inflamed tissue.
There are several strategies useful for distinguishing between appendicitis and thrombophlebitis by sonography. If the patient is in a puerperal state and an apparent appendicitis is found, the sonographer should entertain the suspicion that it could be a thrombosed right ovarian vein or venous collateral. An apparent blind end should be closely examined to confirm that it is real. If possible, a laminar wall structure should be identified at the end, although a normal wall might not be present in cases of ruptured appendicitis. Examining the IVC around the level of the renal veins can be helpful, as clot extension into the vena cava can occur with POVT. The liver and right kidney can provide good sonographic windows for visualization of the IVC near the right renal vein.17,33 The sonographer should also attempt to visualize a normal appendix, excluding appendicitis if it is found.
One of the most important things the sonographer should do is to attempt to follow the structure to the cecum. Placing the patient in a left lateral decubitus position or left posterior oblique position and applying graded compression may displace the bowel, improving views of the area of pathology. If it is the ovarian vein, it could become apparent that it extends not toward the cecum but toward the IVC. If a connection cannot be found between the tubular mass and the cecum, the sonographer should alert the radiologist to the possibility of an alternative diagnosis.
CT and MRI have higher sensitivity and specificity for OVT than sonography. CT or MRI should be considered as a first-line modality when POVT is suspected highly or as a follow-up to sonography when the findings are nondiagnostic. CT is often preferred due to its rapid access and lower cost compared to MRI. 29 On CT, right OVT appears as tubular mass with hyperenhancing walls and a low-attenuation luminal filling defect. 29 The thrombosed vein courses from the pelvis to the IVC. Appendicitis may also appear similarly as a tubular structure with enhancing walls and a low-attenuation lumen, but its connection to the cecum and its blind end can often be identified. Even if the sonographic examination is diagnostic of or highly suspicious for POVT, a CT may still be useful to get a more comprehensive view of the area, checking for clot extension, secondary pathology, and pulmonary embolism. Both sonography and CT can be used to follow the resolution of the thrombus on successive examinations.7,17
Conclusion
Postpartum ovarian vein thrombosis is an uncommon and potentially fatal disorder. The symptoms and other clinical findings can be identical to those of appendicitis. Sonographically, the two conditions are similar and can be indistinguishable without meticulous attention to detail. Herein an unusual case of postpartum thrombophlebitis of a retroperitoneal varix is presented to which many of the same clinical and imaging principles apply.
Sonography is often the first-line imaging modality in patients with postpartum complications. In a postpartum patient with right lower quadrant pain, thrombophlebitis should be considered, even if blood tests and vital signs are normal. If a right lower quadrant tender tubular mass is found with a sonogram, measures should be taken to try to distinguish between appendicitis and thrombophlebitis. If a definite blind end and a clear connection to the cecum cannot be established with certainty, the diagnostic uncertainty should be communicated to the interpreting radiologist.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.