
Abstract
Acute appendicitis is the most common surgical abdominal emergency. Its clinical diagnosis remains a challenge to surgeons, so different imaging options were introduced to improve diagnostic accuracy. Among these imaging modality choices, diagnostic medical sonography (DMS) is a simple, easily available, and cost effective clinical tool. The purpose of this study was to assess the accuracy of DMS, in the diagnosis of acute appendicitis compared to the histopathology report, as a gold standard. Between May 2015 and May 2016, 215 patients with suspected appendicitis were examined with DMS. The DMS findings were recorded as positive and negative for acute appendicitis and compared with the histopathological results, as a gold standard. In all, 173 patients were correctly diagnosed as having acute appendicitis by DMS out of 200 cases, with a final histopathologic result. Similarly, DMS revealed 13 normal appendices out of 15 nonappendicitis patients. This demonstrated that DMS has a sensitivity of 86.5%, specificity of 86.6%, positive predictive value of 99.8%, negative predictive value of 32.5%, and overall accuracy of 86.5%. These results suggest that DMS may be an accurate, sensitive, and specific tool for diagnosing acute appendicitis and reducing unnecessary appendectomies. DMS should be considered as a credible imaging modality for diagnosing acute appendicitis.
Acute appendicitis is the most common cause of acute abdominal pain that can necessitate emergency surgery.1,2 Despite its prevalence, the diagnosis of appendicitis can be difficult and filled with pitfalls because of the absence of a pathognomonic sign or symptom, the poor predictive value of associated laboratory testing, and its different diagnostic presentations.3,4 An incorrect diagnosis of appendicitis has led to a high rate (8–30%) of unnecessary appendectomies.5,6 In fact, following significant progress in accuracy, imaging is now regarded as an essential part of the diagnostic workup of appendicitis. 7 Among the imaging methods currently used in the clinical practice, diagnostic medical sonography (DMS) is simple, easily available, noninvasive, convenient and cost effective choice. The sonographic diagnosis of acute appendicitis was first introduced by Puylaert in 1986, one hundred years after the publication of the first paper on acute appendicitis by Fitz. 8 DMS, with graded compression, is performed and aims to optimize visualization of the appendix.9,10 An inflamed appendix typical is noncompressible and can be imaged as a blind-ended, tubular structure with laminated wall, that arises from the base of the caecum. It is nonperistaltic, and the diameter of the inflamed appendix should be greater than 6 mm (Figure 1). Appendicoliths appear as bright echogenic foci with a distal acoustic shadowing, and their visualization can be an added diagnostic finding. Similarly, there may be increased echogenicity of the periappendiceal fat and point tenderness can be elicited, when pushing with the transducer. 11 Lim and Quillin12,13 have described the utility of color Doppler to detect an inflamed appendix. The inflamed thick walled, noncompressible appendix is usually fixed in position. Compressing the inflamed appendix with the transducer will show circumferential color in contrast to the normal gut. The surrounding intestine should be thin walled and compliant to pressure and demonstrate frequent peristalsis. Doppler reflections disappear when gangrene or perforation has occurred. A recent study demonstrated that increased use of preoperative imaging in patients with acute appendicitis resulted in a cost-effective way to reduce a negative appendectomy rate. 14
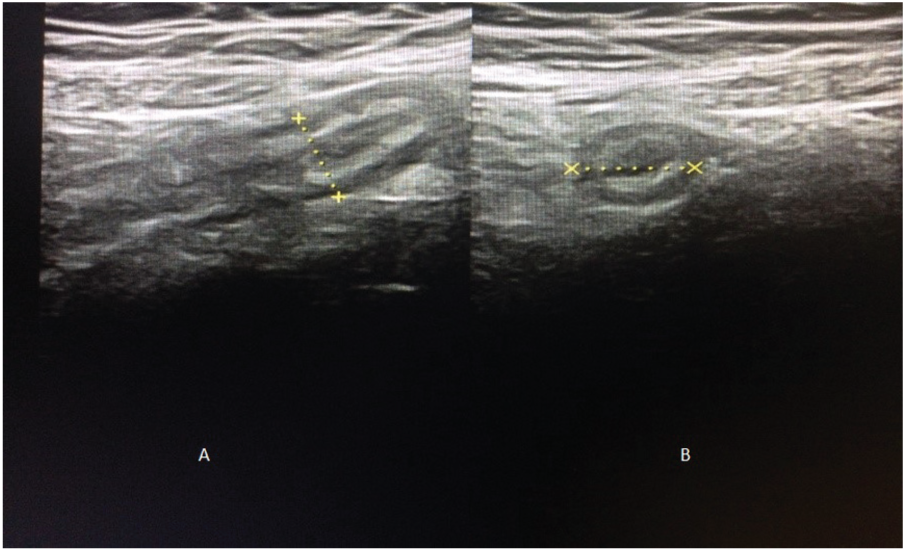
Longitudinal (A) and transverse (B) real-time US scan of acute appendicitis with thickening of the wall, target sign, diameter > 6 mm, and increased echogenicity of the periappendiceal fat.
In fact, DMS is not globally used to rule out an acutely inflamed appendix and this is likely due to the operator’s skill and experience required for a quality sonogram. Very few studies have been conducted in our country and sufficient data were not available regarding the role of sonography in the evaluation of clinically suspected cases of appendicitis. Accordingly, the purpose of this study was to investigate the accuracy of the DMS as a tool in the diagnosis of acute appendicitis with histopathologic results as a gold standard.
Materials and Methods
This cross-sectional prospective study was carried out from May 2015 to May 2016. All patients irrespective of age and sex that were clinically suspected of having acute appendicitis, composed a convenient sample of 215 patients. Exclusion criteria included patients not ready for surgery, patients not ready for further management, those who did not consent, and pregnant patients. Prior to the study, ethical approval from the institutional ethical committee was obtained. Informed consent was taken from all the patients involved in the study and their personal health information was safeguarded.
A structured preprepared data form was used to record the complete history, hematologic data, DMS results, preoperative findings, and the final histopathological report. All DMS examinations were performed by an expert radiologist, with a minimum of 5 years of experience on performing graded compression for suspected appendicitis. A General Electric Voluson ultrasound machine with 3.5 MHZ convex and 7.5 MHZ linear probes were used for this study. To detect the vermiform appendix clearly, graded compression technique was used. This technique requires uniform pressure to be applied in right iliac fossa (RIF) with the ultrasound transducer, so normal and gas-filled loops of intestine are either displaced from the field of view or compressed between anterior and posterior abdominal walls. The DMS findings were recorded as positive and negative for acute appendicitis. Visualization of an appendix that had a noncompressible, tubular, blind-ended, nonperistaltic appearance was imaged. A measured diameter of 6 mm or more, in the RIF, was considered positive for the diagnosis of appendicitis. This inflamed appendix has a target appearance, on transverse DMS images. Other supportive criteria for a positive sonographic diagnosis included the demonstration of appendicoliths, transducer point tenderness, increased echogenicity of the periappendiceal fat, and free intraperitoneal fluid, particularly in RIF or pelvis. Visualization of an appendix of less than 6 mm in diameter or nonvisualization was recorded as a negative result. Positive and negative appendices on histopathology were graded in accordance with the following criteria: Negative appendectomy was defined as normal looking appendix and absence of acute inflammation on histopathology, while positive cases included appendices showing acute inflammatory changes. The histopathologic report was considered to be the gold standard and the final diagnosis of acute appendicitis. Therefore in this study, the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of DMS was based on the reported findings of histopathology.
Data were entered into computer package SPSS 19 for statistical analysis. The level of significance (P value) was set at ≤.05. The study sensitivity, specificity, positive predictive value, negative predictive value, and accuracy were calculated.
Results
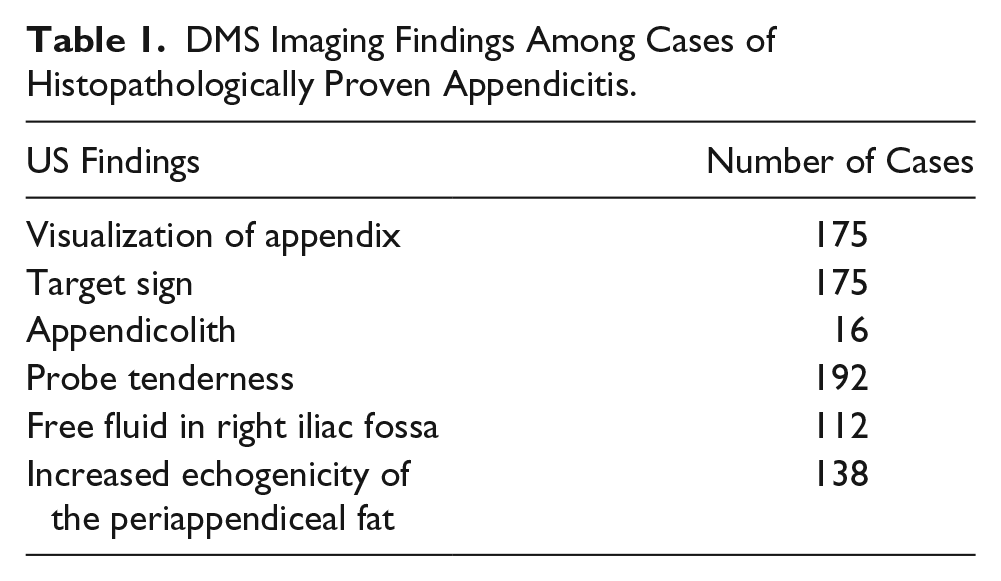
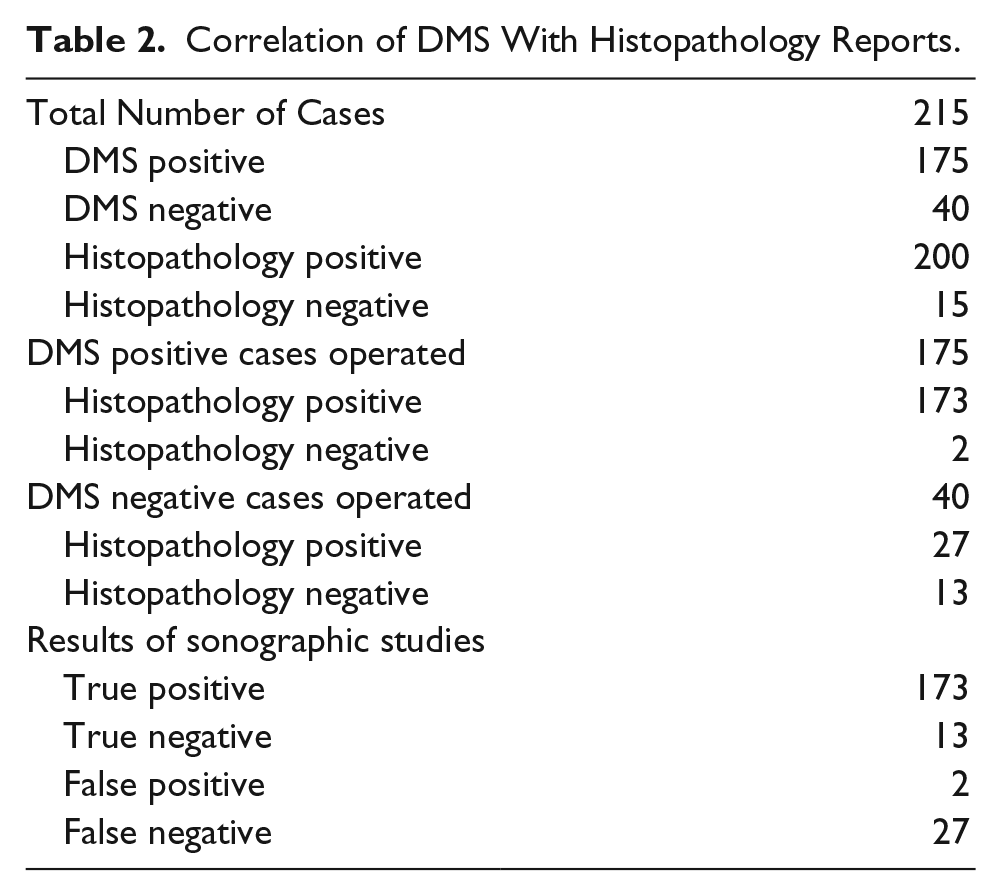
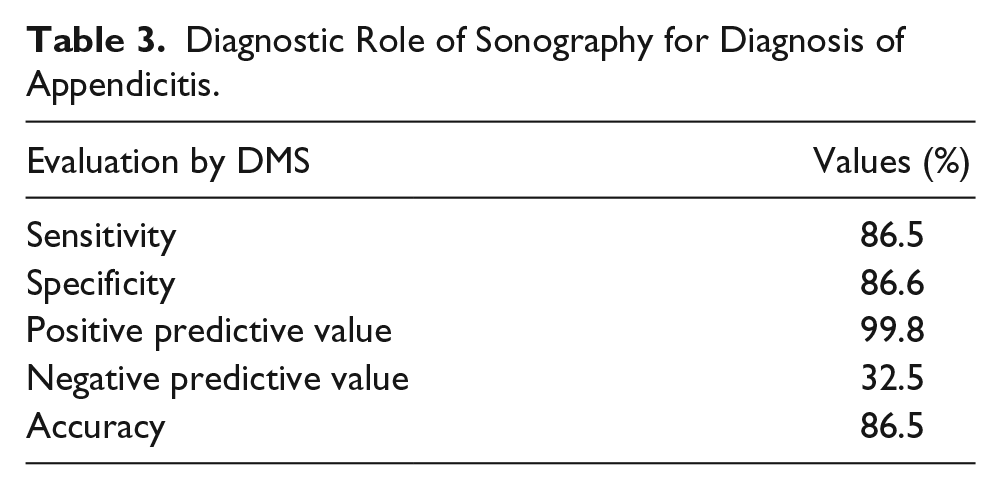
A total number of 215 patients, with suspected acute appendicitis, were included in this study. The mean age of the patients was 23.49 ± 10.93 years, of which there were 112 males and 103 females. The DMS and histopathological examinations were completed on all patient cases. The appendix was visualized in a total of 200 cases and 175 exhibited imaging features of inflammation as described in Table 1. The appendix was not visualized, with DMS, in 15 study patients. DMS results were positive in 175 patients, true positive in 173 patients and false positive in 2 patients. DMS results were negative in 40 patients, true negative in 13 patients and false negative in 27 patients as shown in Table 2. Regarding the histopathological findings, the results indicated that an acutely inflamed appendix existed in 200 cases and a normal appendix in 15 cases (Table 2). Statistical analysis showed that DMS with graded compression yielded a sensitivity of 86.5%, specificity of 86.6%, diagnostic accuracy of 86.5%, positive predictability power of 99.8%, and negative predictability power of 32.5% (see Table 3).
DMS Imaging Findings Among Cases of Histopathologically Proven Appendicitis.
Correlation of DMS With Histopathology Reports.
Diagnostic Role of Sonography for Diagnosis of Appendicitis.
Discussion
Although DMS is frequently used to diagnose acute appendicitis, the accuracy of this imaging examination remains unclear because of a great variability in its reported performance. In this study, the accuracy rate of DMS in diagnosing acute appendicitis in comparison to histopathology results was 86.5% with sensitivity and specificity 86.5% and 86.6%, respectively. These results regarding the accuracy and sensitivity agree with the study completed by Hiwa, 15 where the author reported the accuracy and sensitivity of DMS as 83.3% and 82.1%, respectively. However that study reported a high specificity that reached 100%. This stands in contrast to the present study that did not achieve that specificity. Moreover, the present study findings are inconsistent with results of a study by Hanna et al., 16 who reported the accuracy of DMS to be 96.6%, sensitivity 96%, and specificity 93%. The present study results agree with the results of Pinto et al., 17 which demonstrated an overall sensitivity of DMS as 86%, specificity 81%, and accuracy of 84%.
A meta-analysis was published on the role of DMS with graded compression, in the diagnosis of acute appendicitis which was conducted a few years ago and included 22 articles. 18 The overall sensitivity and specificity was reported to be 86.7% and 90.0%, respectively. This study suggested that DMS could be useful for the diagnosis of acute appendicitis, especially when patients were younger males and highly clinically suggestive. These findings are very comparable to the present study results provided.
However DMS accuracy in diagnosing acute appendicitis, in the present study, was better than in Parsijani et al., 19 who reported DMS accuracy as 73.6%, sensitivity as 75%, and specificity as 69.2%.
The variations in the results of these cited articles may be attributed to many factors. First, given that DMS is an operator-dependent technique, the individual skill becomes a variable in determining the diagnostic imaging accuracy of appendicitis. 10 Furthermore, challenges to examine populations of young females may be linked to an overlap of symptoms and gynecologic complaints, as well as acute abdominal diseases. 20 Obese patients, as well as individuals who sustained an earlier laparotomy, present difficulties achieving enough graded compression of the right lower quadrant and high quality examinations. 21 Variability in the appendix site is a well-known cause for clinical misdiagnosis, and a false negative DMS diagnosis can occur, especially in cases of a retro-cecal location for the appendix. This anatomical variant can be a reason for not appropriately visualizing the structure.
PPV and NPV of DMS in the present study were 99.8% and 32.5%, respectively. The NPV was consistent with Hanna et al., 16 and this indicates that with an appendix that appears normal on DMS, it is important to add clinical findings as well as a possible computed tomogram (CT). The present study results regarding PPV and NPV were very comparable to those in other studies by Nasiri et al. 22 (97.4% for PPV and 25% for NPV) and Hiwa 15 (100% for PPV and 26.6% for NPV).
The results of this study are limited due to the research design and the sample of patient cases analyzed. It does provide a low level of evidence that a positive DMS study may be an accurate diagnosis for acute appendicitis. However, a negative DMS study is not sufficient to disregard a possible diagnosis of appendicitis without additional diagnostic evidence.
Van Atta et al. 23 recommended using DMS as a primary modality to evaluate pediatric patients with suspected acute appendicitis. Also, they suggested using CT only in equivocal cases. This would match with the concerns for a possible missed diagnosis based on DMS alone. Interestingly, the American College of Radiology (ACR) recommends CT as the most appropriate imaging choice with DMS using graded compression as a secondary option. 24
Conclusions
Imaging is an important diagnostic component for patients deemed to be clinically suspicious for acute appendicitis. DMS has the potential to improve the patient outcome and to reduce the risk for a negative appendectomy. DMS should be a first imaging choice for diagnosing acute appendicitis. The findings of this study add to the data concerning the accuracy, sensitivity, and specificity of using DMS to detect acute appendicitis. We believed that nonvisualization of the appendix should lead to a clinical reassessment. The role for CT and DMS, with graded compression, maintains its ranking by the ACR, until higher level evidence is available.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.