
Abstract
Stretching and exercise are recommended to prevent work-related musculoskeletal disorders (WRMSD) in sonographers, but evidence is lacking. The purpose of this study was to identify sonographers’ physical activity levels and types and frequency of exercise performed regularly. This quantitative descriptive study used a minimally adapted long-form version of the International Physical Activity Questionnaire, distributed to Society of Diagnostic Medical Sonography members. Consistent with prior research, over 80% of 530 participants scanned in pain or had a WRMSD. A majority (85.6%) reported a high level of physical activity from moderate work and domestic-related activities, with a median of 5 hours daily spent sitting. While 69.1% walked or hiked at least one to three times a week, stretching and strength exercises were not as prevalent. Cumulative effects of everyday activities may increase WRMSD risk. Improving muscular fitness and taking time for muscle recovery might help sonographers avoid or reduce WRMSD pain. Implementing and applying preventative WRMSD strategies may need stakeholder support.
Keywords
Sonographers are highly susceptible to work-related musculoskeletal disorders (WRMSDs). Injurious WRMSDs are inflammatory or degenerative processes that affect soft tissues, nerves, muscles, ligaments, and/or tendons and are a leading cause of workforce discomfort, pain, and disability.1,2 It has been reported that at least 80% to 90% of sonographers scan in pain or have been diagnosed with an WRMSD.3–6 A WRMSD and/or the pain experienced by a sonographer can limit the ability to obtain quality images and affect overall job performance.7,8 Secondary effects of WRMSD pain, such as work absences, increased health care costs, and decreased productivity, are costly for both sonographers and employers.7,9,10 Sonographers may also experience a decreased quality of life as they find it difficult to go about normal daily activities without pain.4,8,11 It is estimated that 20% of sonographers change careers or seek early retirement because of a WRMSD.4,6
Muscle strain, shoulder, arm, and back pain in sonographers were first reported by Craig 12 in 1985, but at that time, ultrasound equipment was large and cumbersome. Also, awareness and application of proper ergonomics was not well known. 13 Over the years, surveys highlighting sonographers’ WRMSD experiences increased awareness and the need for ergonomic standards.5,6,14 Research has shown administrative, equipment, environmental, patient, and sonographer factors are associated with WRMSD development.7,9,15,16 However, even with improvements in technology; smaller, lighter ultrasound machines; greater awareness; and the development of ergonomic guidelines, the incidence of WRMSDs persists. Reportedly, only 10% to 20% of sonographers are pain free.3,4 At the time of this publication, there are approximately 65,790 working sonographers in the United States, which means 52,632 are scanning in pain. 17
Sonographic procedures involve repetitive motions, forceful exertions, awkward postures, and static positions, which are reasons cited for WRMSD development.7,18 Movement is dependent on the interrelationships of the body’s systems (e.g., circulatory, musculoskeletal) and is the result of the interactions of an individual, a task, and an environment.19,20 Consequently, physical activity, which is the movement of skeletal muscle that requires the use of energy, 21 can be limited by an individual’s abilities or functional capacity to complete the demands of a task. Sustaining an awkward posture increases the work and energy expense of the muscles; therefore, the time to muscle fatigue is shortened. 22 In contrast, movement associated with physical activity and exercise (i.e., a structured and planned type of physical activity) increases an individual’s strength, flexibility, and endurance; thus, postural control, the capacity to resist muscle fatigue, muscle recuperation time, and everyday performance are improved.7,9,23
Most ergonomic research in sonography has been confined to the workplace. However, nonwork-related activities, such as a heavy domestic workload and gardening, have been associated with WRMSD development.24,25 When an individual develops a WRMSD, treatment often includes physical therapy that involves stretching and strengthening exercises to enhance postural abilities and to increase range of motion. 26 However, research on stretching and exercise for sonographers is dated and limited. There are no longitudinal studies involving large samples, 27 and there is no evidence that sonographers who exercise regularly have a lower risk for a WRMSD.28,29 Conversely, Alaniz and Veale 27 reported that many sonographers considered stretching to be beneficial and recommendations for stretching and exercise are found throughout the literature; however, sonographer activity level (low, moderate, high) and types of exercise or physical activity have not been studied. Sonographer activities and behaviors beyond the workplace may explain why WRMSDs remain prevalent and why some individuals are unaffected. Thus, the purpose of this quantitative descriptive study was to identify the overall physical activity level of sonographers in relation to their everyday activities (i.e., work, domestic, leisure, transportation) and to describe the types and frequency of structured exercises that sonographers engage in on a regular basis.
Method
This was a quantitative descriptive study. Data were collected via a descriptive survey. Nonprobability consecutive sampling methodology was used. The Society of Diagnostic Medical Sonography (SDMS), with an accessible population of over 27,000 members, 30 agreed to distribute the survey to its members. The recruitment email with the survey link was sent to 20,177 SDMS members who opted to be included in research emails and who met the inclusion/exclusion criteria. Eligible participants were (a) currently employed as a sonographer, (b) nonstudent members of the SDMS, and (c) US residents. Student memberships and individuals who had an SDMS Corporate, Business, Institution (CBI) membership were excluded from the study. The study was approved by the Thomas Jefferson University and the A. T. Still University Institutional Review Boards.
An adapted self-report online descriptive survey was created using SurveyMonkey software. The survey included the long-form version of the International Physical Activity Questionnaire (IPAQ), 31 which is a validated instrument appropriate for population-based research of physical activity in individuals aged 18 to 65,32–34 and a self-developed segment, which was divided into three sections: demographics, work-related characteristics, and types of structured exercise. All survey items were closed-ended.
Basic demographic questions were asked at the beginning of the survey, which included items pertaining to sex, race, ethnicity, education, marital status, age, height, and weight. A minimally adapted long-form version of the IPAQ, 31 which includes measures of leisure and nonleisure physical activity, as it relates to work, transportation, domestic, leisure, and sedentary behavior (sitting time) followed. The long form 31 consists of 27 items presented in a dichotomous format. Based on a response, branch logic is used to direct respondents to the next appropriate item. The IPAQ instrument was minimally adapted to include sonographer-specific activities and to reflect the Centers for Disease Control and Prevention 35 measures of relative physical activity intensity. Analysis and data-processing guidelines provided with the IPAQ tool were followed and are available on the IPAQ website. 26 The guidelines were used to quantify the intensity and frequency of physical activity and to convert the computed items into a metabolic equivalent of task (MET). The calculated MET, which is the metabolic rate (i.e., the energy cost of activities) based on the intensity and minutes per week of an activity, 36 was used to categorize the level of physical activity. High and moderate intensity levels of activity were classified as per the IPAQ guidelines. 31 Participants who did not qualify for high or moderate levels of activity were considered to have a low level of physical activity. Total minutes spent sitting per week was used to calculate sedentary behavior.
Items pertaining to work-related characteristics included registered or unregistered sonographer, credentials, years of scanning experience, hours spent scanning per week, number of patients scanned in a day, percentage of portables (bedside scans) performed per day, percentage of time scanning right- or left-handed, if diagnosed with a musculoskeletal disorder (MSD) related to scanning or scan in pain, percentage of time spent scanning in pain, if they stretch during working hours, and use of ergonomic principles/techniques. The last portion of the self-developed section involved multiple-choice checklists that included the frequency and intensity of structured exercises and two items regarding child/parental care.
Study participants were contacted via email by the SDMS. The email included the link to the online questionnaire which was available for 48 days. After 3 weeks, a follow-up email was sent. To gain access to the survey and ensure study eligibility, participants were asked to confirm they were currently working as a sonographer, not an ultrasound student, and a US resident. If eligible, a participation statement followed, but if ineligible, a thank you page appeared and the respondent could not access the survey. Survey completion constituted informed consent. Data were collected from mid-August through early October 2017.
Statistical Analysis
Data analyses were conducted using IBM SPSS Statistics Version 24 (SPSS, Inc, an IBM Company, Chicago, Illinois). Frequencies and valid percentages were calculated for demographic and work-related characteristic data. Data normality was assessed via the Shapiro-Wilk test (P < .05) for age, height, weight, and years of scanning experience. Median and interquartile ranges were reported for the nonnormally distributed variables.
To identify the physical activity level of sonographers, MET-minutes per week were calculated and used to categorize physical activity as low, moderate, or high. Physical activity levels were reported as valid percentages. A Shapiro-Wilk test (P < .05) was used to assess the normality of MET-minutes per week for domain, total activity, and sedentary behavior (time spent sitting) subscores. Medians and interquartile ranges were reported for all nonnormally distributed items.
Descriptive statistics (frequencies, valid percentages) were calculated for the types and frequency (times per week) of structured exercises in which respondents regularly participated. Frequencies and valid percentages were also used for the types (i.e., housework, yard work/gardening, child/parental care) and frequency (times per week) of participation in domestic-related activity.
Results
A total of 20,177 sonographers were invited to participate (see Figure 1). Of 806 individuals who clicked on the survey link, there were 782 responses. Eighty-three respondents did not meet the inclusion criteria; another 169 participants did not adequately complete the survey and thus were not included in data analysis. The final analytic sample was 530, which represented a completion rate for those opening the survey of 75.8%.
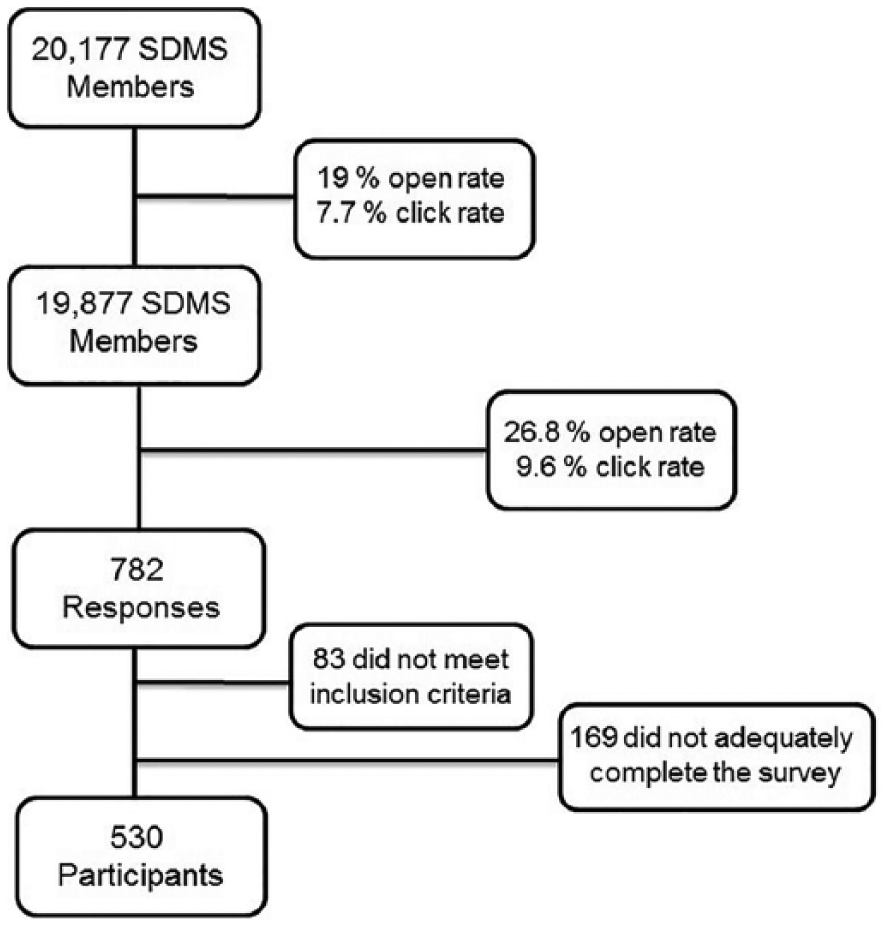
Chart demonstrating how the final number of participants was obtained. Open and click rate information was provided by the Society of Diagnostic Medical Sonography (SDMS). Open rate is the percentage of SDMS members/accessible population who opened the email. Click rate is the percentage of members/potential study participants who clicked on the survey link.
Demographic and Work-Related Characteristic Findings
Demographic data results are provided in Table 1. Participants were predominately female (88.7%), white (90.6%), married (74.4%), and had either an associate’s (37.5%) or bachelor’s degree (33.4%). Age ranged from 23 to 73, with a median age of 52 (interquartile range [IQR] = 4). The median height and weight for participants were 65 inches (IQR = 4) and 155 pounds, respectively (IQR = 49).
Participant Demographics (N = 530).
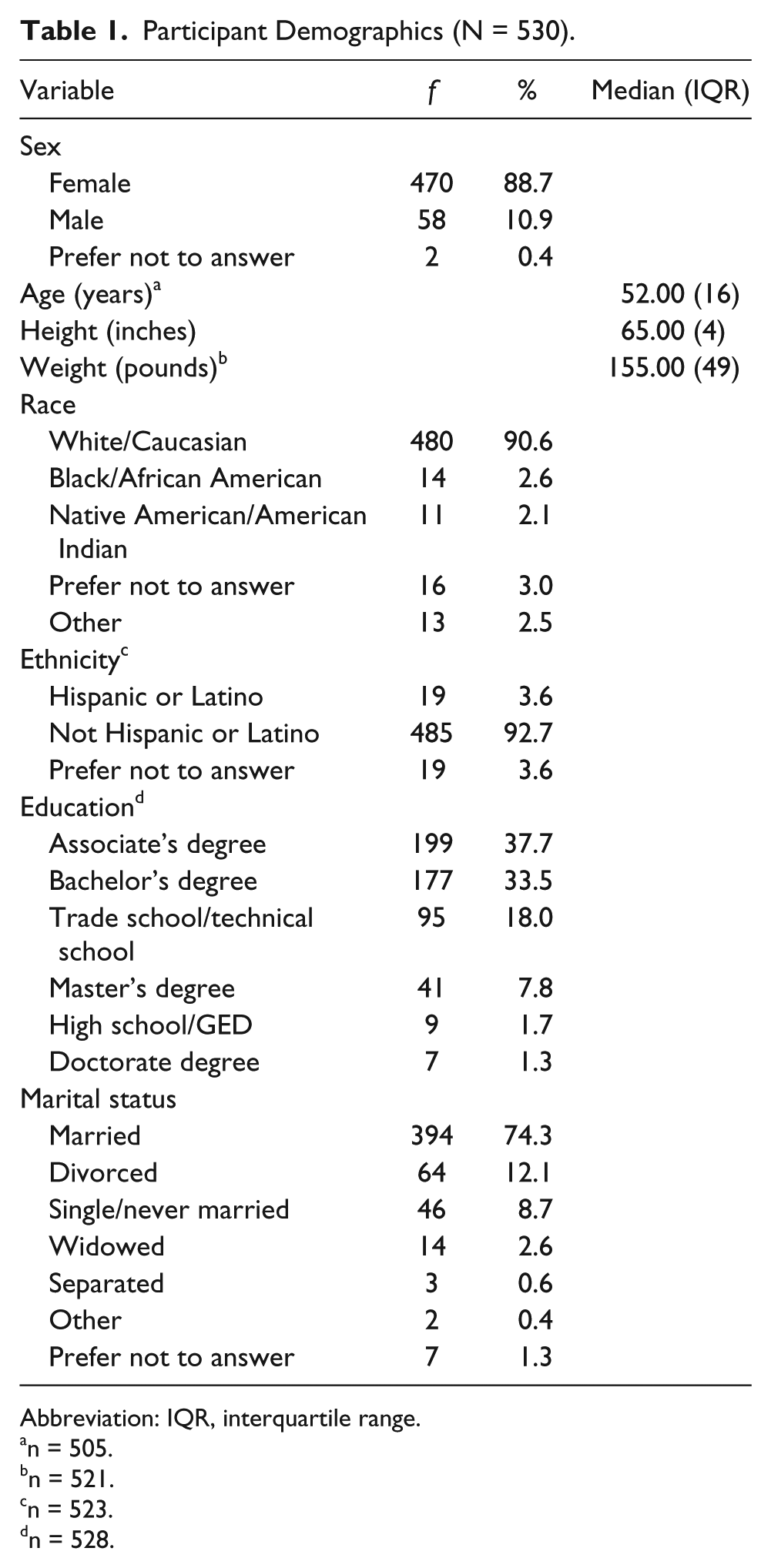
Abbreviation: IQR, interquartile range.
n = 505.
n = 521.
n = 523.
n = 528.
Results for work-related characteristics are found in Table 2. A majority of respondents were registered sonographers (98.9%), with registered diagnostic medical sonographer (RDMS) the credential most frequently reported (86.6%). The years of scanning experience ranged from 1 to 45 with a median of 23 years (IQR = 19). The median for hours scanning patients per week was 35 (IQR = 14), median number of patients scanned per day was 10 (IQR = 4), and median percentage of portables was 1 (IQR = 10). More participants scanned 100% of the time with their right hand (67.9%) compared to the left hand (6.8%). While 40% of respondents reported never having been diagnosed with a musculoskeletal injury related to scanning, 82.8% indicated having scanned in pain. The median for the percentage of time spent scanning with pain was 25 (IQR = 59). Pain and musculoskeletal injuries were reported most frequently (see Figure 2) in the shoulder (78.3%; 51.7%, respectively) and the neck (85.1%; 41.5% respectively). Only 19.1% of participants indicated they always stretched during working hours; however, 39.4% employed ergonomic principles and techniques more than 76% of the time.
Work-Related Characteristics (N = 530).
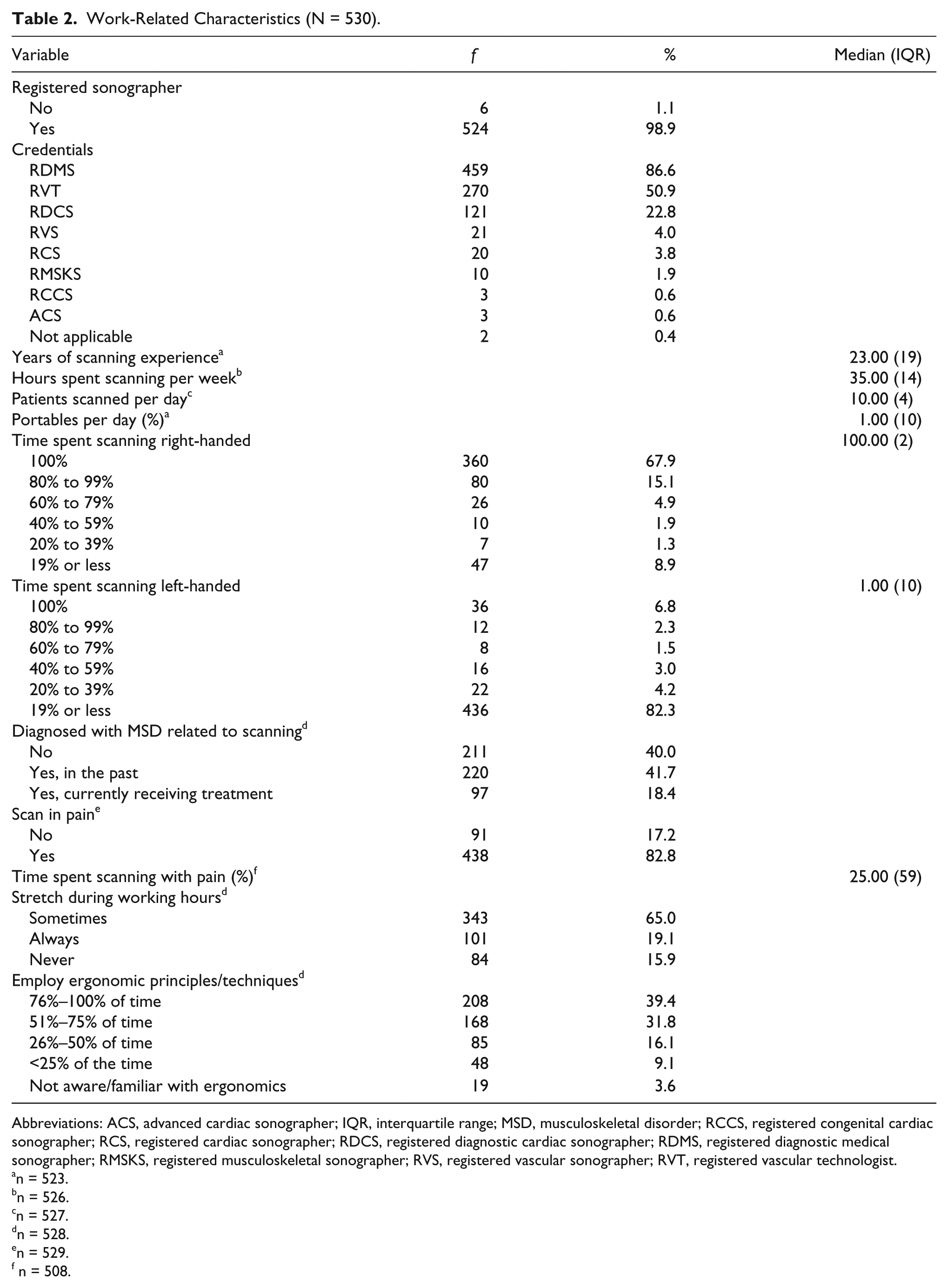
Abbreviations: ACS, advanced cardiac sonographer; IQR, interquartile range; MSD, musculoskeletal disorder; RCCS, registered congenital cardiac sonographer; RCS, registered cardiac sonographer; RDCS, registered diagnostic cardiac sonographer; RDMS, registered diagnostic medical sonographer; RMSKS, registered musculoskeletal sonographer; RVS, registered vascular sonographer; RVT, registered vascular technologist.
n = 523.
n = 526.
n = 527.
n = 528.
n = 529.
n = 508.
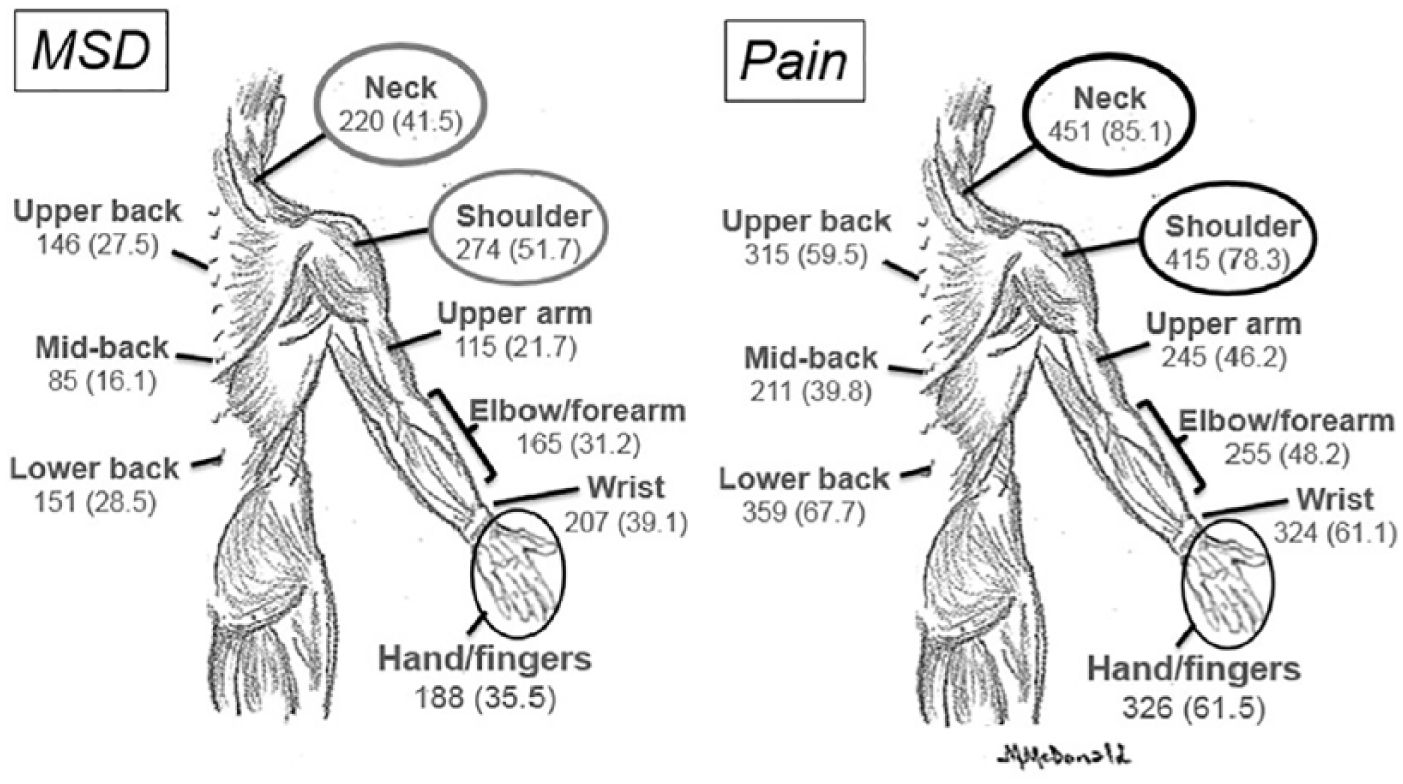
The frequency and percentage of respondents (N = 530) who reported work-related musculoskeletal disorders (WRMSDs) and/or pain for each region of the body. MSD, musculoskeletal disorder.
Physical Activity Findings
The level of physical activity associated with the work, domestic, leisure, and transportation-related domains was assessed (see Table 3). A majority of respondents (85.6%) described their physical activity level as high. Normality testing for all domain subscores, total activity subscores, and sedentary subscores was assessed using a Shapiro-Wilk test, and all were found to have nonnormal distribution, yielding P = .000 for all variables. The highest calculated physical activity domain MET value was work-related endeavors (median = 3600.00; IQR = 4118) while moderate activities (median = 4452.00; IQR = 5609) across all domains contributed the most to the total physical activity level. A median of 300 minutes was reported for time spent sitting on weekdays (IQR = 240) and weekend days (IQR = 240); this did not include sitting in a motor vehicle for daily transportation, which had a median of 131 minutes (IQR = 74).
Metabolic Equivalent (MET) Physical Activity and Sedentary Behavior Scores (N = 530).
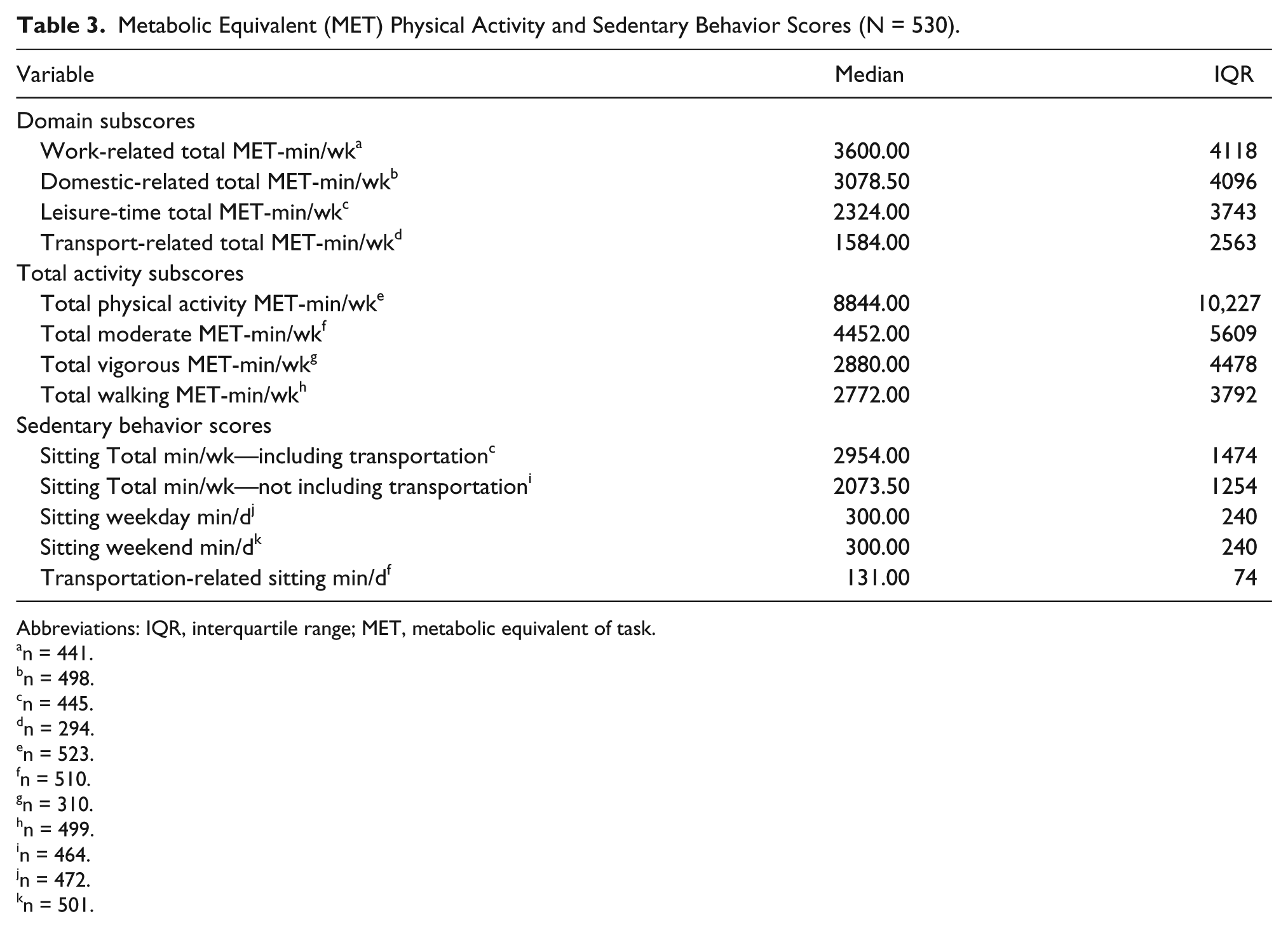
Abbreviations: IQR, interquartile range; MET, metabolic equivalent of task.
n = 441.
n = 498.
n = 445.
n = 294.
n = 523.
n = 510.
n = 310.
n = 499.
n = 464.
n = 472.
n = 501.
Participants were asked to identify the types of structured exercise and their frequency of participation. Respondents reported participating more in individual exercises (see Figure 3) rather than team sports. While there were several individual exercises identified, walking/hiking was reported most frequently (69.1%). Most walkers/hikers did so at least one to three times a week (41.9%). Lifting weights and/or strength training at least one to three times a week (28.7%) was also an activity reported by many (37%), as was yoga (20.3%), biking (20.1%), and running/jogging (19.1%). Most exercises identified, such as yoga, biking, and running/jogging, were performed one to three times a week (18.3%, 17.5%, and 14.3%, respectively), but a small number of exercises were engaged in at least six or seven times a week; walking/hiking was the most common (9.1%).
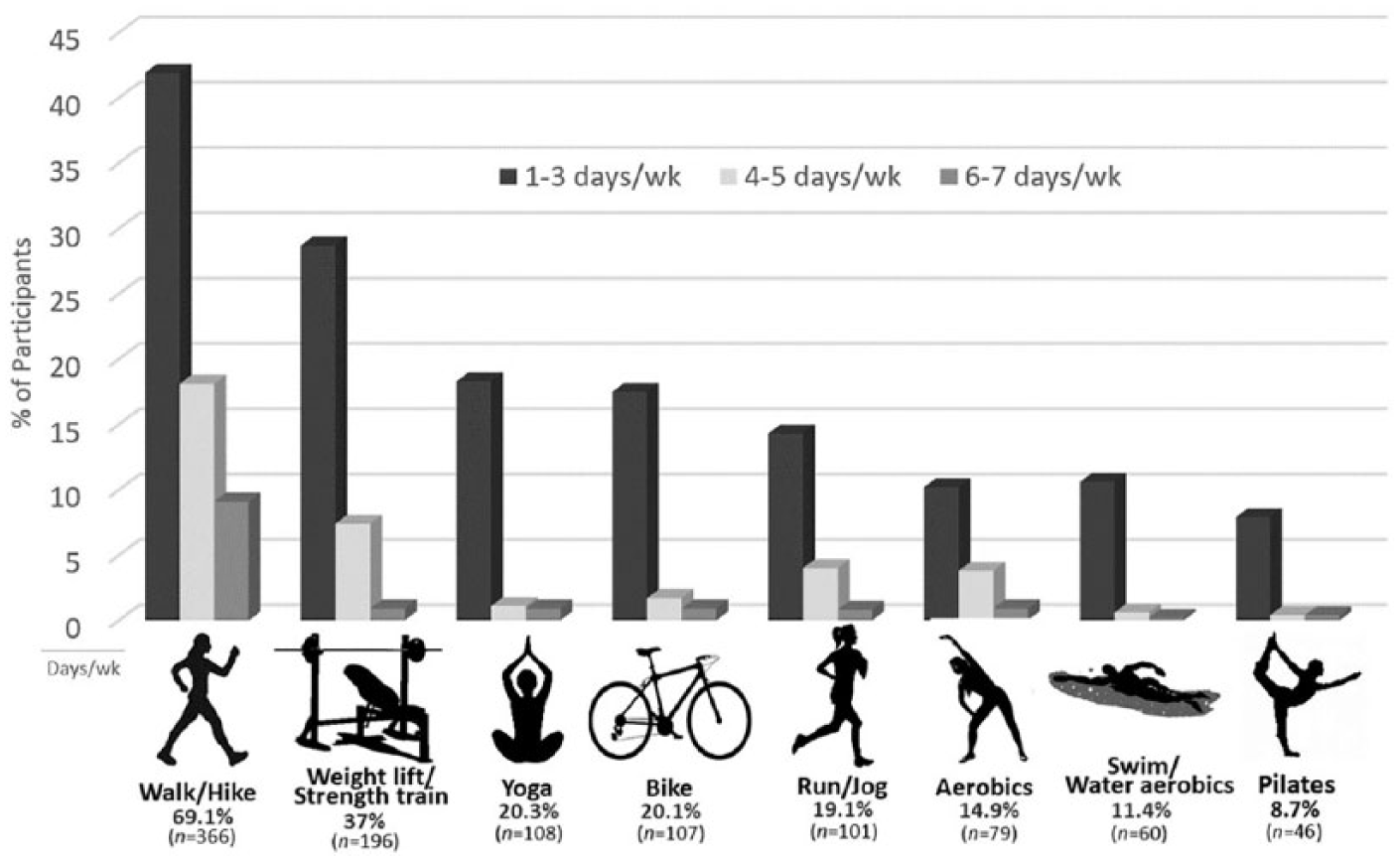
The percentage of respondents (N = 530) who noted participation in the top eight reported types of exercise and the frequency of involvement. Some respondents may have participated in more than one activity.
A majority of respondents reported housework (91.5%) as a leisure activity, most commonly one to three times a week (47.4%), while 68.2% noted working in the yard. Child and/or parental care was noted by 29% of respondents who reported care involved six or seven days a week (17.4%).
Discussion
The majority of respondents reported a high level of physical activity related to everyday endeavors, with moderate activities across all domains predominating. However, work-related behaviors accounted for the largest portion of the total physical activity reported, which was unexpected given sonographers may sit while scanning patients. Nonetheless, the job of a sonographer can be physically demanding and includes activities such as positioning patients who are less mobile, transferring patients from wheelchairs to stretchers and back, scanning individuals in place when they are unable to get out of a wheelchair, and transporting heavy equipment for bedside scans.7,15,37 Sonographers who perform portable examinations often need to rearrange furniture and monitoring equipment to accommodate an ultrasound machine, but the ability to create a suitable environment for ergonomic scanning is not always possible. Therefore, to obtain quality images, there may be a greater need for sonographers to maintain awkward postures when scanning patients at bedside. Consequently, the physicality of portables can be pronounced; however, the percentage of bedside scans reported by respondents was low.
The second highest type of physical activity reported in this cohort of sonographers was domestic-related behaviors (indoor and outdoor). Housework (e.g., cooking, cleaning, vacuuming) and/or child/parental care may also involve awkward postures and repetitive motions, as can gardening and yard work.24,25,38,39 Unfortunately, many individuals often work in the garden and/or yard with little thought about the movements involved and use improper body mechanics, which can cause muscular stress and pain. 25 A more frequent use of awkward postures and repetitive movements can occur when work and domestic-related activity times are combined, suggesting muscles may not have a chance to properly rest and recover.24,39,40 High workloads may exacerbate the issue. Janga and Akinfenwa 41 found a strong correlation between sonographer WRMSD symptoms and no regular breaks, but breaks taken after working hours also enhance muscle recovery time. The lifestyle practices of the respondents suggest muscle recovery time after work is limited, which can further provoke WRMSD development.7,15,42 Therefore, incorporating mini-breaks during leisure time or between patients may help to give muscles additional time to recover.7,15,42 Sonographers can also give a mini-break to one side by scanning ambidextrously,15,37 but consistent with other research, this strategy is little used.11,43 Scanning with one dedicated hand may be more common because of a lack of ambidextrous training and/or space limitations of the scanning environment.44,45 In this cohort, most respondents only scanned with their right hand.
Physical fitness and exercise have been recommended for lowering WRMSD risk and to improve muscular capabilities and efficiency.26,27,43,46 Improved muscle strength enhances physical performance and balance, supports posture, and helps prevent injuries. While a large number of respondents walked or hiked, a smaller number of participants were regularly involved with muscle-strengthening exercises, such as weightlifting, yoga, or Pilates. Musculoskeletal discomfort was found to be lower when strength training incorporated multiple muscular groups (e.g., yoga, Pilates) and mimicked movements used with everyday activities. 47 Pilates, which improves flexibility and balance, and exercise programs using kettlebells and/or elastic tubing, which may include bending, twisting, and pulling, have helped reduce WRMSD pain in health care workers and patients.48–50 There is also evidence that exercise programs involving stretching have been helpful in preventing WRMSD development. 51 Stretching has also been reported as beneficial for sonographers 27 ; therefore, regular stretching could help lower the pain associated with a WRMSD. While 65% of respondents reported occasionally (i.e., sometimes) stretching while at work, how individuals perceive sometimes can vary. Importantly, only a small portion of participants made stretching a routine work practice. An additional benefit of exercise is that it can have a positive effect on an individual’s sense of well-being and is often used to lower stress levels. Job stress can add to WRMSD development, 15 but a positive sense of well-being can be enhanced with exercise and decrease the risk.42,52
When assessing overall physical activity levels of a population, the amount of inactivity should also be considered. Physical inactivity, also known as sedentary behavior, can have detrimental effects on an individual’s health and is associated with an increased risk for chronic conditions, such as heart disease and osteoporosis.21,53 Unfortunately, the health benefits of exercise can be negated by a high amount of sedentary behavior, such as sitting. 53 In addition, prolonged sitting can heighten musculoskeletal discomfort and potentially increase WRMSD risk. 54 Sonograms can be performed either seated or standing; consequently, some sonographers may have a greater amount of sitting time. Respondents reported sitting for about seven hours per day, which included transportation time. Assimilated data from the 2015 to 2016 National Health and Nutrition Examination Survey revealed more than 61% of adults in the United States sit 6 hours a day or greater 55 ; therefore, it is not surprising sitting time for respondents fell within this range. Although previous studies have found sitting time to be underestimated, and it is possible the respondents here did the same, there is no documented threshold for what is considered an acceptable level of sitting time.53,56 Nonetheless, a high volume of physical activity at a moderate to vigorous level can help offset the effects of sedentary behavior. 57
The percentage of sonographers who scan in pain or have an WRMSD was found to be consistent with previous research.3–6,16 The shoulder and neck were also the most common locations affected.3,6 This research supports previous findings that ergonomic principles and techniques are not always used.7,15,16 Importantly, not employing ergonomic techniques increases muscle work and the need for muscle recovery time. 7
Implications of Findings
The findings of this study are clinically significant for both sonographers and employers. It is suggested for sonographers to incorporate time into their daily routine for muscle recovery and stretching and strengthening exercises, but finding the time may be challenging. Taking breaks on the job, when the workload is high or the department is short staffed, can be difficult. Also, the time allotted for examinations may not be adequate. Many departments schedule patients every 15 to 30 minutes, 37 even though 45 to 60 minutes (time from patient encounter to departure) has been recommended for some sonographic examinations. 58 Employers need to recognize excessive sonographer workloads can fuel stress, limit muscle recovery time, increase WRMSD pain, and may lead to employee dissatisfaction and absenteeism. Collaboration between employers and sonographers is needed to improve patient and staff scheduling practices. Adding workplace intervention programs that involve stretching and/or resistance training can help lower the occurrence of WRMSDs and its symptoms. 51 Workplace interventions not only improve employee fitness but also lower absenteeism, stress, and disability costs. 59
This study also has educational implications. Sonography programs accredited by the Commission on Accreditation of Allied Health Education Programs 60 are required to include instruction on ergonomic principles. However, the requirements are vague, and it is possible ergonomic education is deficient in teaching the importance of strengthening exercises and personal health. 28 Many respondents in this study did not participate in a regular exercise program even though movement, stretching, and exercise are recommended to lower WRMSD risk.7,9 Individuals who consider a career in sonography need to understand the physicality of the job and the ongoing need for personal health and fitness. Teaching students proper ambidextrous scanning techniques may also help improve muscle balance, help body alignment, and lower WRMSD risk. 44 Educational programs should reevaluate how ergonomics is taught and ensure a healthy lifestyle that includes regular exercise is part of the curriculum.
Study Limitations and Recommendations for Future Research
This study had several limitations. For example, respondents’ levels of pain and physical fitness were not assessed, and individual perceptions of pain and physical fitness can vary. Individuals with a higher or more persistent level of pain or who are in poor physical shape may perceive physical activity to be more demanding than persons who regularly exercise. 61 Physical activity has been overestimated in previous self-reported activity studies, and this may hold true for these respondents.53,55 Individuals with higher levels of pain and/or in poor physical condition may have found awkward postures, patient transfers, and positioning patients more taxing and overestimated their level of physical activity. Conversely, sonographers in good physical shape and/or less pain may have underestimated their physical activity level.
The length of the instrument, which was estimated to take at least 15 minutes, may have deterred some individuals from completing the questionnaire. It is also possible that only sonographers who were interested in WRMSDs and/or suffer from a WRMSD were willing to complete the voluntary survey, which may have introduced selection bias. Data collection also began in mid-August when many individuals take vacation and extended into the beginning of the school year; therefore, sonographers with family obligations may not have participated.
Future research should include assessments of the levels of pain and physical fitness of sonographers. Even though stretching and exercise have been recommended, correlational studies to assess the relationship (occurrence or absence) of a WRMSD and/or pain compared to (a) whether sonographers stretched during working hours, (b) the type and frequency of exercise performed, and (c) domestic-related physical activities are needed. Research to assess the frequency, duration, and intensity of stretching and structured exercises could build evidence for preventive care and be used to support and create sonographer-specific guidelines for the types of exercise and workouts that would best reduce and/or relieve WRMSD pain.
Conclusion
The purpose of this quantitative descriptive study was to explore the level of sonographer physical activity and identify the types and frequency of regular exercise performed. This study illustrated the potential additive effect of work and nonwork-related activities on WRMSD development. Being highly active does not necessarily mean the types of activities are appropriate for lowering WRMSDs. Therefore, improving muscular fitness through stretching and strengthening exercises and taking time for muscles to rest and recover, by incorporating breaks between scans and/or domestic activities, may help lower WRMSD risk. In addition, collaborative scheduling practices between employers and sonographers and early sonographer education on a healthy lifestyle may also increase a sonographer’s ability to offset the risk of a WRMSD.
Footnotes
Acknowledgements
The authors would like to thank the Society of Diagnostic Sonography for distributing the survey to its members.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.